Urinary Tract Infections (UTIs)
Urinary Tract Infections (UTIs)
Welcome to the comprehensive master guide on Urinary Tract Infections (UTIs). This guide covers everything from the microscopic battleground between bacterial virulence factors and host defenses, to step-by-step diagnostic workups and evidence-based treatment guidelines.
1. The Definitions
Before diving into pathology, you must master the precise terminology used to describe urinary infections.
- Bacteriuria: Simply means the presence of bacteria in the urine.
- Significant Bacteriuria: The number of bacteria in voided urine exceeds what would be expected from normal contamination by the anterior urethra. Cutoff: ≥ 105 bacteria/mL. If you see this, infection must be seriously considered.
- Asymptomatic Bacteriuria: Significant bacteriuria (≥ 105) in a patient with absolutely ZERO symptoms. (We will discuss later who gets treated for this and who does not!)
- Location: UTIs can be confined to the lower tract (bladder/urethra) or involve both the upper (kidneys) and lower tracts.
- Cystitis (Lower UTI): A clinical syndrome involving dysuria (painful urination), frequency, urgency, and occasionally suprapubic (lower abdominal) tenderness.
- Acute Pyelonephritis (Upper UTI): A more severe clinical syndrome characterized by flank pain or tenderness (costovertebral angle), fever, often associated with the lower tract symptoms (dysuria, urgency, frequency).
- Uncomplicated UTI: Infection in a structurally and neurologically normal urinary tract.
- Complicated UTI: Infection in a urinary tract with functional or structural abnormalities (e.g., indwelling catheters, neurogenic bladder, or kidney stones/calculi).
Uncomplicated vs. Complicated
Patient A: A healthy 22-year-old female presents with painful urination and urgency for 2 days. She has no medical history. This is an Uncomplicated UTI (Cystitis).
Patient B: A 65-year-old male with an enlarged prostate (BPH) and a history of kidney stones presents with the same symptoms. Because his urinary tract has structural blockages that prevent normal urine flushing, this is a Complicated UTI and requires much more aggressive management.
Urosepsis is the sepsis syndrome caused by a UTI. It is a life-threatening medical emergency. To diagnose it, you need clinical evidence of a UTI PLUS two or more of the following SIRS (Systemic Inflammatory Response Syndrome) criteria:
- Temperature: > 38°C (Fever) OR < 36°C (Hypothermia)
- Heart Rate: > 90 beats per minute (Tachycardia)
- Respiratory Rate: > 20 breaths/minute, OR PaCO2 < 32 mm Hg (Tachypnea/hyperventilation)
- White Blood Cell Count: > 12,000/mm3 (Leukocytosis), OR < 4,000/mm3 (Leukopenia), OR > 10% band forms (immature neutrophils).
2. Epidemiology & Common Bugs
- Females: UTI is much more common in women. 1-2% of young, non-pregnant women have it at any given time. 40% of all females will have a symptomatic UTI in their lifetime.
- Males: Extremely rare in young men (prevalence is only 0.04%). Clinical Pearl: If a young man gets a UTI, look for a structural defect or a Sexually Transmitted Disease (STD)!
- Older Age: Incidence skyrockets in the elderly (10% of men, 20% of women) due to functional impairments, prostate enlargement, and estrogen loss.
The "Ojambo 2008" Ugandan Data:
Over 95% of UTIs are caused by a single bacterial species. According to Ojambo 2008, the predominant organisms are:
- Escherichia coli (45%) - The undisputed king of UTIs.
- Klebsiella species (17%)
- Staphylococcus species (8%) - Most common Gram-positive.
- Enterococcus (5%)
Other common offenders: Proteus, Pseudomonas, Enterobacter, and Candida (fungus, usually seen in diabetics or patients with chronic indwelling catheters).
3. Pathogenesis:
A UTI is an epic battle between bacterial virulence factors and host defense mechanisms.
The Routes of Invasion
- Ascending Route (Most Common): Bacteria from the gut colonize the perineum/urethra and climb up into the bladder. Why women? The female urethra is short and anatomically very close to the warm, moist vulvar and perianal areas, making fecal contamination highly likely.
- Hematogenous Route (Blood-borne): Infection of the kidney tissue by organisms traveling in the blood.
- Clinical Scenario: A patient with Staphylococcus aureus endocarditis (heart valve infection) throws infected blood clots into the kidneys, causing renal abscesses.
- Lymphatic Route: Rare, spread via lymphatic channels.
Parasite Virulence Factors
Not all E. coli cause UTIs. The ones that do are called Uropathogenic E. coli (UPEC) clones (Serogroups O1, O2, O4, O6, O7, O8, O75, O150, and O18ab). They possess specific genetic superpowers:
- Adhesins (Fimbriae/Pili): Prevent the bacteria from being washed away by urine.
- P fimbriae: Bind to Gal-α 1-4 (P blood group antigen). Strongly associated with Pyelonephritis and bacteremia.
- Type 1 fimbriae: Bind to mannosylated proteins (uroplakin Ia) on bladder cells. Associated with cystitis.
- Resistance to serum bactericidal activity.
- K Antigen (Capsules): High quantities of K1, K5, K12 capsular antigens physically protect bacteria from leukocyte phagocytosis.
- Aerobactin: An iron-scavenging protein (siderophore). Iron is scarce in urine; aerobactin steals it for the bacteria to grow.
- Hemolysin & Cytotoxic Necrotizing Factor type 1 (CNF-1) & Sat Toxin: Toxins that facilitate tissue invasion, cause severe renal tubular damage, and lyse red blood cells to make even more iron available to the invading E. coli.
- Urease (Specifically in Proteus species): Proteus produces urease, which splits urea into ammonia. This strongly correlates with its ability to cause severe pyelonephritis and struvite kidney stones.
- Deep Dive: Ammonia makes the urine highly alkaline. This change in pH causes magnesium, ammonium, and phosphate to crystallize, forming massive "staghorn" struvite stones that fill the entire renal pelvis!
Master Table: Uropathogenic E. coli Adhesins
| Adhesin | Genetic Sequence | Receptor Target | Clinical Comments |
|---|---|---|---|
| Type 1 fimbriae (MS) | Pil, fimH | Mannosylated proteins on epithelial cells (uroplakin Ia) & PMNs | Binds to Tamm-Horsfall protein (THP) and SIgA. |
| P fimbriae (MR) | papG (class Ia, II, III) | Gal-α 1-4 (P blood group antigen) | Class II: Strongly associated with pyelonephritis & bacteremia. Class III: Cystitis in patients with urinary tract abnormalities. |
| S/F1C fimbriae (MR) | Sfa/fac | Sialyl-(α-2-3) galactoside | Adherence is inhibited by THP. |
| Type 1C (MR) | Fac | Undetermined | Possibly associated with pyelonephritis. |
| G fimbriae (MR) | — | Terminal N-acetyl-D-glucosamine | — |
| M fimbriae (MR) | — | Galactose-N-acetyl-galactosamine / Blood group M (glycophorin A) | — |
| Dr family | Drb operon, Afa E1-5, Afa F | Dr blood group antigen (decay accelerating factor - DAF) & type IV collagen | Found in 16% of first-time cystitis isolates. |
The Host's Defenses (Why we don't always have a UTI)
The normal urinary tract efficiently and rapidly eliminates microorganisms through:
- Urine Flow & Micturition: The physical flushing mechanism of the bladder is the single major protective effect. (Think of it like a powerful river continuously washing away mud from the riverbanks).
- Urine Chemistry: Extreme osmolality, high urea concentration, and low pH are highly inhibitory to fastidious and anaerobic bacteria.
- Urinary Inhibitors of Adherence: Your body secretes Tamm-Horsfall protein (THP), bladder mucopolysaccharides, low-molecular-weight oligosaccharides, SIgA, and Lactoferrin to bind up bacterial fimbriae so they can't stick to your cells!
- Inflammatory Response: When bacteria stick, epithelial cells release cytokines, summoning Polymorphonuclear neutrophils (PMNs) to eat the bacteria.
- Prostatic Secretions: In men, these have natural antibacterial properties.
The kidney is NOT uniformly susceptible to infection. The Medulla is highly vulnerable (very few organisms needed to infect), while the Cortex is highly resistant (requires 10,000 times more organisms!). Why?
- High concentration of ammonia in the medulla inactivates complement proteins.
- High osmolality, low pH, and low blood flow cause poor chemotaxis of neutrophils (PMNs). Analogy: The medulla is a harsh, salty desert. The immune cells literally shrink up and get stuck before they can reach the bacteria!
Also, remember: The greater the number of organisms delivered to the kidneys, the greater the chance of infection.
STEP 1: THE CLINICAL HISTORY (Manifestations & Risk Factors)
When a patient walks in, you must evaluate their risk factors and symptoms to distinguish between Cystitis, Pyelonephritis, or Asymptomatic Bacteriuria.
Reviewing Risk Factors
Obstruction inhibits normal urine flow; stasis is the most important factor in increasing susceptibility.
- Extrarenal Obstruction: Congenital anomalies (valves, bands, stenosis), calculi (stones), benign prostatic hypertrophy (BPH), extrinsic ureteral compression.
- Intrarenal Obstruction: Nephrocalcinosis, uric acid nephropathy, analgesic nephropathy, polycystic kidney disease, hypokalemic nephropathy, sickle cell trait/disease.
- Adult Females: Sexual intercourse (honeymoon cystitis), lack of post-coital urination, spermicides, diaphragms, pregnancy, diabetes, HIV (high viral load).
- Older Age: Estrogen deficiency leads to a loss of vaginal lactobacilli (the good bacteria), allowing E. coli to overgrow. Mental impairment, bladder prolapse, and catheterization also highly increase risk.
Clinical Manifestations by Age & Type
- Neonates & Children < 2 years: Symptoms are totally nonspecific. Look for failure to thrive, vomiting, and unexplained fever.
- Children > 2 years: Frequency, dysuria, and abdominal or flank pain.
Frequent and painful urination of small amounts of turbid (cloudy) urine, suprapubic heaviness/pain. Urine may be grossly bloody or show a bloody tinge at the end of micturition (hemorrhagic cystitis).
The "Classic Triad" of upper tract infection:
- Fever (with chills)
- Flank pain (costovertebral angle tenderness)
- Lower tract symptoms (frequency, urgency, dysuria).
The vast majority are actually asymptomatic! If they do present, the classic burning urination might be absent. Instead, their only symptom may be sudden confusion or delirium.
STEP 2: THE DIAGNOSTIC WORKUP (Presumptive & Culture)
A. Presumptive Diagnosis (Urinalysis / Dipstick)
Microscopic examination of the urine is the absolute first step in the lab diagnosis.
- Pyuria (Pus/WBCs in urine): The preferred definition is ≥ 10 leukocytes/mm3 of midstream urine using a counting chamber.
- Leukocyte Esterase Test: A rapid dipstick screening test for detecting pyuria. (Pyuria alone is non-specific, but highly suggestive when symptoms are present).
- Hematuria: Microscopic or gross blood indicates mucosal irritation (hemorrhagic cystitis).
- White Cell Casts: Pathognomonic for Pyelonephritis (indicates inflammation is happening high up in the kidney tubules, where casts are formed).
- Proteinuria: Common in UTI, but usually mild (< 2 g/24 hrs).
- Direct Gram Stain: Finding at least 1 bacterium per High Power Field (HPF) in an uncentrifuged, clean-catch urine specimen correlates perfectly with ≥ 105 bacteria/mL.
Bacterial Count Extrapolation: 1 Bacterium per Microscopic Field = CFU/mL
| Sample Preparation | Unstained (×400) | Stained (×1000) |
|---|---|---|
| Uncentrifuged sample | ≥ 106 | ≥ 105 |
| Centrifuged sample | ≥ 105 | ≥ 104 |
B. Diagnosis by Culture
Urine is easily contaminated by skin flora. Culturing quantifies the bacteria to statistically separate true infection from contamination.
Collection Techniques
- Midstream Clean Catch (Preferred):
- Women: Wash hands, straddle commode. Wash vulva front-to-back 4 times with 4 different sterile gauze pads soaked in green soap. Rinse with 2 sterile water sponges. Spread labia, void, discard first portion, collect the second (midstream).
- Men: Retract prepuce, clean, collect midstream.
- Catheterization: Used for patients with altered sensorium. Requires scrupulous aseptic technique.
- Suprapubic Aspiration: Inserting a needle directly through the abdomen into a full bladder. Highly safe and sterile. Used in premies, neonates, children, adults, and even pregnant patients.
- Note on infants: Sterile adhesive bags are used, but contamination is highly common.
- Lab Processing: Process immediately. If delayed, refrigerate at 4°C and culture within 24 hours.
Culture Methodology & Interpretation
The lab uses platinum calibrated loops (0.01 mL or 0.001 mL) to streak urine onto agar. After 24 hours at 37°C, Colony Forming Units (CFUs) are counted and multiplied by 100 or 1000 respectively.
- Asymptomatic Women: 1 clean-catch with > 105 bacteria/mL = 80% probable true bacteriuria. You MUST get 2 separate specimens showing > 105 of the same bacterium to reach 95% probability and confirm the diagnosis!
- Symptomatic Women: While > 105 is classic, a third of young women with lower UTI symptoms have fewer than 105.
- IDSA Consensus Guidelines:
- Cystitis: > 103 CFU/mL of a uropathogen.
- Pyelonephritis: > 104 CFU/mL.
- Men: > 103 organisms/mL is highly suggestive of infection.
- False-Negative Cultures: Caused by patient taking antibiotics, soap falling into the urine cup, total obstruction below the infection site, fastidious organisms, renal tuberculosis, or heavy diuresis (diluting the urine).
Note: The high count criteria mainly apply to Enterobacteriaceae. Gram-positives, fungi, and fastidious bugs might cause true infection at only 104 to 105 /mL. Mixed infections occur in ~5% of cases.
6. Natural History & Management (Treatment)
Natural History
- Uncomplicated UTI: Treatment leads to complete cure. Recurrences may happen in clusters (usually within 2-3 months), but they do not lead to chronic renal impairment.
- Complicated UTI: Recurrent complicated UTIs can lead to renal failure and accelerate the progression of underlying renal diseases.
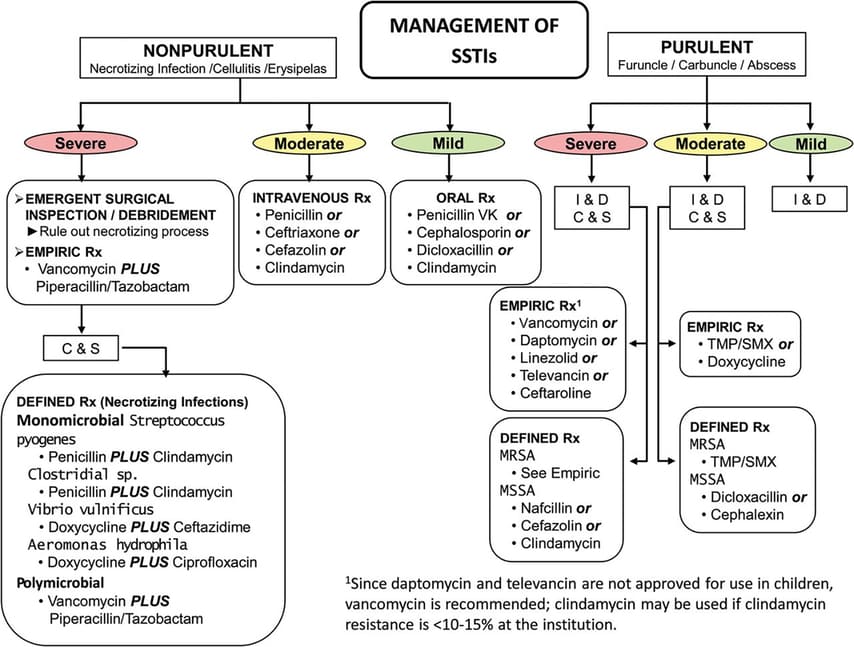
Treatment Guidelines
1. Acute Pyelonephritis
- Mild: Treat orally (Fluoroquinolones, Co-trimoxazole, Cefuroxime).
- Moderate-Severe: Parenteral/IV treatment (Aminoglycosides, Ceftriaxone, Aztreonam, Tazocin). Therapy leads to marked decline in count after 48 hours.
- Red Flags: If there is persistent fever or a positive blood culture after 3 days of therapy, rule out obstruction or kidney abscess!
- Step-down: After defervescence (fever breaks), switch to oral therapy to complete a full 2 weeks. Follow-up culture 2 weeks after finishing antibiotics.
- In males: always look for a predisposing structural cause.
2. Cystitis
- Young Females (Uncomplicated): 3 days of oral therapy (Fluoroquinolone, Cotrimoxazole, Cefuroxime, Augmentin).
- Females with delayed presentation: If symptoms have lasted x 7 days OR history of previous infection → treat for 7 days.
- Males: Treat orally for 7-10 days.
To Treat or Not To Treat?
There is NO urgency to treat. Confirm with 2 cultures first.
YES - INDICATED TO TREAT IN:
- Pregnancy (Massive risk of progressing to pyelonephritis and causing premature labor).
- Children with Vesicoureteral (VU) reflux.
- Patients with Urinary Obstruction.
NO - NOT INDICATED IN:
- Young non-pregnant women without structural abnormalities.
- Elderly patients (Very high yield! Treating asymptomatic elderly patients just causes antibiotic resistance. Do not treat a positive culture in a nursing home patient who has no symptoms!).
3. Relapse vs Recurrent UTI
The Definition: The exact same organism re-emerges because it was never fully eradicated. It was hiding in a kidney stone, a structural abnormality, or the prostate (chronic bacterial prostatitis).
Treatment for Relapse: Needs 2 weeks of antibiotics. Obstruction MUST be corrected. If uncorrectable, treat for 4-6 weeks (or longer), do monthly follow-up cultures, and annually assess the kidneys. In males, specifically rule out chronic prostatitis.
The Definition: A brand new infection from outside, usually introduced weeks or months after the first one completely cleared.
Treatment for Recurrence: If infrequent, treat the individual attacks. In females, if related to sex, advise: avoiding spermicides, voiding after intercourse, or taking a post-coital single-dose antibiotic.
If no precipitating factors exist, or for frequent asymptomatic infections in kids with VU reflux / patients with obstructive uropathy → start Long-term prophylaxis.
Quick Quiz
UTI\'S Quiz
Microbiology - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
UTI\'S Quiz
Microbiology
Preparing questions...
Choose your answer and keep your streak alive.
Great effort.
Here is your quick performance summary.
Urinary Tract Infections (UTIs) Read More »