
A tumor is a lump or mass made of abnormal cells that grow when they should not grow. In children, these cells usually grow very fast and can spread to other parts of the body. Normal cellular apoptosis (programmed cell death) fails.
- Benign tumor: Not cancer. It grows in one place, is usually encapsulated, and does not spread. Usually not life-threatening, though it can cause issues if it presses on vital organs (like the brain).
- Malignant tumor: This is cancer. It can grow into nearby tissues and spread (metastasize) to distant parts of the body through blood or lymph fluid.
- Children are still growing: Cancer treatment (especially radiation and steroids) severely affects their physical growth, bone development, and cognitive development.
- Children's bodies handle medicines differently: They have a higher percentage of total body water and immature liver/kidney enzyme systems, altering how chemotherapy is metabolized and excreted.
- Different types of cancer: Adults mostly get carcinomas (epithelial cancers from aging/lifestyle), while children get embryonal tumors, leukemias, and sarcomas (cancers of developing mesoderm/tissues).
- Better chances of cure: Because pediatric cancers are fast-growing, they are actually more responsive to chemotherapy (which targets rapidly dividing cells). Children also tolerate higher relative doses of chemotherapy than adults.
- Not caused by lifestyle: Children's cancers are usually not caused by lifestyle (smoking, alcohol, diet) but by genetic changes (mutations) that happen spontaneously during fetal or early childhood development.
- Burkitt lymphoma: Very common, highly aggressive B-cell lymphoma. Strongly linked to endemic malaria and the Epstein-Barr virus (EBV). Often presents as a massive jaw or abdominal tumor.
- Leukemia: Specifically ALL (Acute Lymphoblastic Leukemia).
- Retinoblastoma: Eye tumor. Often noticed late due to lack of screening; presents as a white pupil (leukocoria).
- Wilms tumor (Nephroblastoma): Kidney tumor, usually presenting as an asymptomatic, smooth abdominal mass.
- Kaposi sarcoma: Endothelial cancer, especially prevalent in HIV-positive children (HHV-8 virus).
- Brain tumors: Medulloblastoma, astrocytomas.
Teach parents and community health workers to look for these early indicators:
- Swelling or lump that does not go away.
- Sores that do not heal.
- Sudden weight loss.
- Severe or persistent headaches, especially with vomiting in the morning (Pathophysiology: Lying flat at night increases Intracranial Pressure (ICP) from a brain tumor, triggering the vomiting center upon waking).
- Swelling of the abdomen (tummy) (Could indicate Wilms tumor or Burkitt lymphoma).
- Sudden eye changes (white pupil, squint) (Classic for Retinoblastoma).
- Severe fatigue and paleness (Anemia from Leukemia).
- Severe bone pain (Marrow expansion from Leukemia cells).
- Seizures that start suddenly.
Remember CHILD CANCER:
- Continued, unexplained weight loss
- Headaches with vomiting in the morning
- Increased swelling or persistent pain in bones/joints
- Lump or mass in abdomen, neck, or elsewhere
- Development of a whitish appearance in the pupil
- Constant infections
- A whitish color behind the pupil
- Nausea that persists
- Constant tiredness or noticeable paleness
- Eye or vision changes occurring suddenly
- Recurrent fevers of unknown origin
As a pediatric oncology nurse, you wear many hats:
- Caregiver: Giving highly toxic medicines, managing severe symptoms and side effects.
- Educator: Teaching the family about the disease, treatment phases, and critical home care (infection prevention).
- Advocate: Speaking for the child when they cannot speak (especially regarding pain management).
- Counselor: Supporting the child and family emotionally through a terrifying diagnosis.
- Coordinator: Connecting the family with social services, transport, and food support (abandonment of treatment is high in resource-limited settings due to financial strain).
- Aseptic Technique: Always use clean hands, clean gloves, and clean equipment. Cancer treatment destroys the child's immune system (neutropenia), so even small, normally harmless germs (commensal flora) can cause deadly systemic sepsis.
- Vascular Access Devices: Chemotherapy requires reliable venous access.
- Peripheral IV: Short-term access in hand or foot veins. Highly risky for vesicant chemotherapies (can cause tissue necrosis if they leak).
- Central Line (CVAD): Long-term catheter placed in large chest veins (Superior Vena Cava). Used for chemotherapy, frequent blood draws, and TPN/fluids.
- Port-a-cath: Small device surgically placed completely under the skin with a chamber that is accessed with a special non-coring (Huber) needle. Lowest infection risk.
- Nursing Care for Central Lines:
- Keep the dressing clean, dry, and intact.
- Check for signs of infection (CLABSI): redness, warmth, pus, fever.
- Flush with heparin or saline as per protocol to maintain patency and prevent clots.
- Never use the line for anything except what it is prescribed for.
- EMERGENCY: If the line comes out accidentally, apply immediate deep pressure to the vein and call the doctor immediately (risk of severe hemorrhage or air embolism).
- Chemotherapy Safety (Protecting Yourself):
- Wear specialized chemotherapy gloves when handling drugs or body fluids for 48 hours after treatment.
- Chemotherapy drugs are toxic and mutagenic – they can harm healthy skin and absorb into your bloodstream.
- Dispose of contaminated materials in special yellow/purple cytotoxic waste bins.
- Pregnant nurses should absolutely not handle chemotherapy due to the risk of teratogenicity (fetal malformation).
- Body Fluid Precautions (Protecting the Family):
- For 48-72 hours after chemotherapy administration: The child's urine, vomit, stool, and saliva may contain toxic drug residue.
- Family should wear gloves when cleaning these fluids.
- Flush toilet twice after use with the lid down to prevent aerosolization.
- Wash soiled clothes separately with hot water and soap.
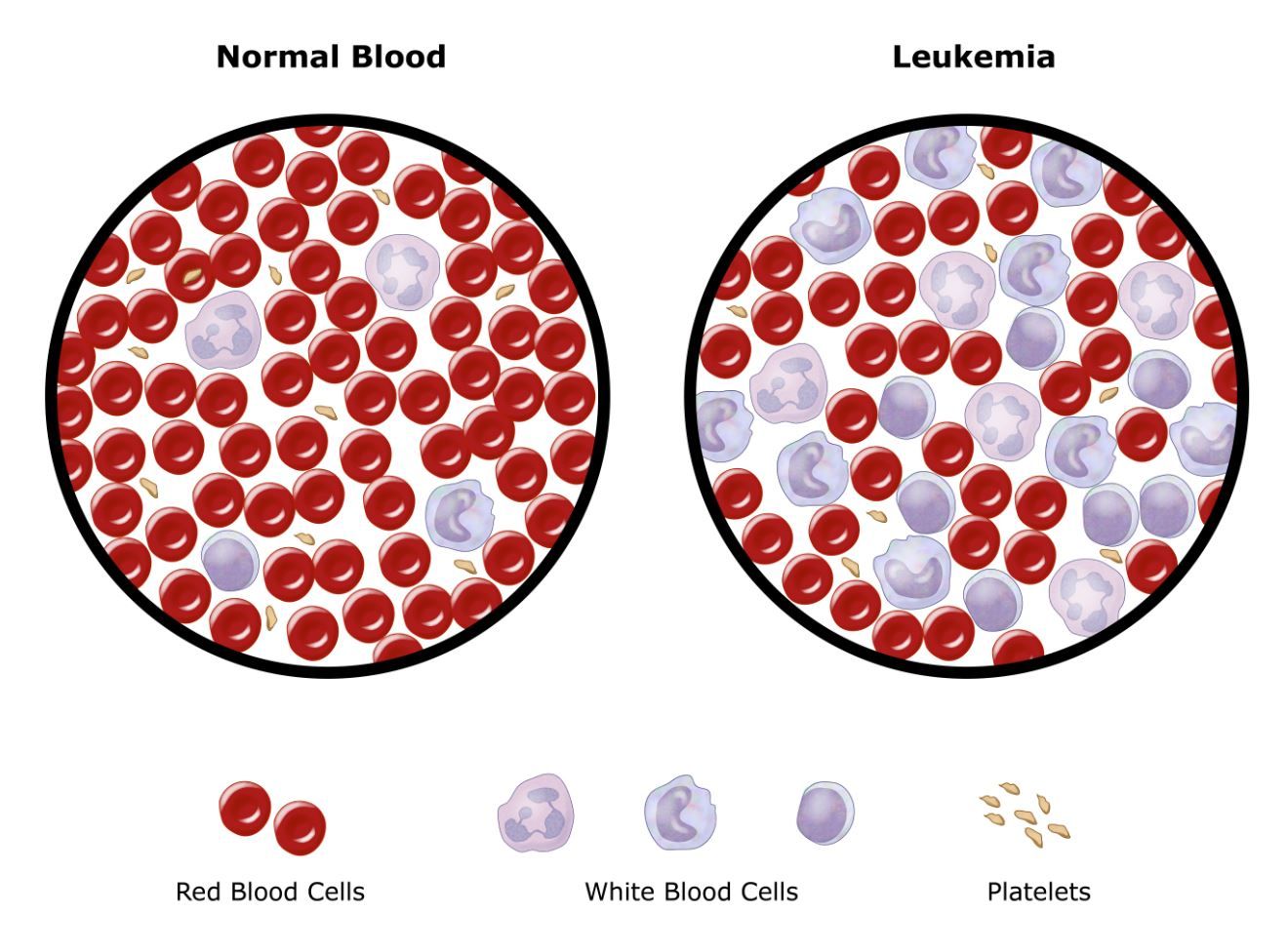
Leukemia is cancer of the blood and bone marrow. Bone marrow is the soft spongy tissue inside bones where all blood cells are made (hematopoiesis). In leukemia, a genetic mutation causes the bone marrow to make too many immature, non-functional white blood cells called blasts. These abnormal blast cells divide uncontrollably and crowd out the healthy blood cells, leading to bone marrow failure.
- Acute Lymphoblastic Leukemia (ALL): The most common cancer in children (75-80% of childhood leukemias). Affects the lymphoid cell line (B-cells and T-cells).
- Acute Myeloid Leukemia (AML): Affects the myeloid cell line (precursors to red blood cells, platelets, and granulocytes). It is more aggressive and harder to treat than ALL.
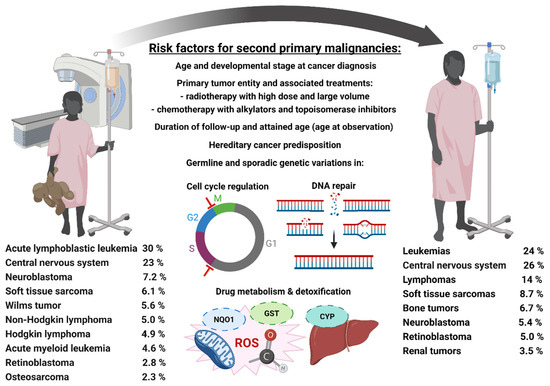
- Genetic changes (mutations or translocations) in developing blood cells.
- Some genetic conditions greatly increase risk (Children with Down syndrome have a 10-20x higher risk of developing leukemia).
- Exposure to radiation or certain chemicals (benzene).
- In Uganda, some association with Epstein-Barr virus (EBV) and malaria in certain types of hematological malignancies.
Understand that leukemia cells don't usually attack other cells directly. Instead, they act like weeds in a garden. They grow so fast that they consume all the nutrients and physical space inside the bone marrow. As a result, the "good plants" (normal Red Blood Cells, Platelets, and healthy White Blood Cells) cannot grow. This marrow failure is what causes 100% of the clinical symptoms!
Because leukemia affects the bone marrow, symptoms are directly related to the lack of normal blood cells (Pancytopenia):
- Low Red Blood Cells (Anemia):
- Pale skin, lips, tongue (always check palms and conjunctiva/nail beds in dark-skinned children).
- Extreme tiredness, weakness, and lethargy.
- Shortness of breath with little activity (tissue hypoxia).
- Fast heartbeat (tachycardia) – the heart pumps faster to compensate for low oxygen carrying capacity.
- Dizziness.
- Low Platelets (Thrombocytopenia):
- Easy bruising (bruises appear without any history of trauma/injury).
- Tiny, pinpoint red/purple spots on skin (petechiae) that do not blanch when pressed.
- Bleeding from nose (epistaxis) or gums.
- Blood in urine (hematuria) or stool (melena).
- Heavy, prolonged bleeding from very small cuts.
- Low Functional White Blood Cells (Infection Risk / Neutropenia):
- Even though the total WBC count might be massively high, these are useless "blast" cells. The child lacks mature neutrophils to fight bacteria.
- Frequent infections (fever, persistent cough, severe mouth sores).
- Infections that do not respond to normal, standard antibiotics.
- Fever without an obvious focal cause.
- Other Signs (Due to Infiltration of Leukemia Cells):
- Bone pain: Caused by the massive expansion of marrow pressing against the periosteum (child refuses to walk, limps, or cries of leg pain).
- Joint pain and swelling.
- Swollen lymph nodes (Lymphadenopathy): Especially in neck, armpits, groin.
- Swollen belly (Hepatosplenomegaly): Enlarged liver and spleen as leukemia cells infiltrate these extramedullary organs.
- Loss of appetite and Weight loss.
- Night sweats.
Confirming leukemia requires a systematic approach from basic blood tests to invasive marrow sampling.
- Full Blood Count (FBC/CBC): Shows low hemoglobin, low platelets, and usually an abnormal white blood cell count (can be very low, or massively high). Crucially, it may show blast cells (immature WBCs) in the peripheral blood, which should normally never leave the marrow.
- Peripheral Blood Film: Looking at blood cells under a microscope by a hematologist. Shows abnormal cell shapes, sizes, and the presence of blasts.
- Bone Marrow Aspiration and Biopsy (The Gold Standard):
- Procedure: A specialized Jamshidi needle is forcefully inserted into the hip bone (posterior superior iliac spine) or breastbone (sternum) to extract liquid marrow and a small core piece of bone.
- Nursing care before: Explain to child using age-appropriate language (e.g., "taking a picture of your bones"), apply EMLA cream (numbing cream) 1 hour before if available, give IV sedation if ordered, ensure informed consent form is signed by parents.
- Nursing care during: Position child properly (side-lying/lateral decubitus or prone), hold and physically comfort the child, continuously monitor vital signs (respirations during sedation), assist the doctor with sterile field.
- Nursing care after: Apply a firm pressure dressing, keep child lying flat for 30-60 minutes to prevent bleeding, check site frequently for oozing/bleeding, give pain medicine (paracetamol/ibuprofen), monitor for infection, allow parent to comfort child.
- Results: If there are more than 25% blast cells in the marrow, acute leukemia is definitively diagnosed.
- Lumbar Puncture (Spinal Tap):
- Checks if leukemia cells have crossed the blood-brain barrier and spread to the brain/spinal fluid (CNS involvement).
- Procedure: Needle inserted between vertebrae (L3/L4 or L4/L5) in the lower back to collect cerebrospinal fluid (CSF).
- Nursing care: Position child in a tight fetal position (knees to chest) or sitting bent forward to open vertebral spaces. Apply EMLA cream, give sedation, hold child completely still. After procedure, keep child strictly flat for 1-4 hours to prevent post-dural puncture headache. Monitor for signs of infection, check puncture site for CSF leakage.
- Chest X-ray: Checks for an enlarged thymus gland (mediastinal mass, common in T-cell ALL) which can compress the airway, or checks for lung infections.
- Ultrasound: Checks for the extent of liver, spleen, and kidney enlargement (leukemic infiltration).
- Flow Cytometry: Special computerized test to identify the exact type of leukemia by looking at proteins (CD markers) on the cell surface. Distinguishes ALL from AML, and B-cell from T-cell.
- Cytogenetics: Looks at chromosome changes (DNA mutations) inside the cancer cells to guide treatment intensity and predict prognosis.
Leukemia is not "staged" like solid tumors (Stage 1, 2, 3, 4) because it is already everywhere in the blood. Instead, it is grouped by Risk:
- Standard risk: Good features. Ages 1 to 10 years old, low white blood cell count at diagnosis (< 50,000).
- High risk: Age under 1 or over 10 years, high white blood cell count (> 50,000), certain genetic changes, or slow response to the first few weeks of treatment.
- Very high risk: Specific aggressive chromosome changes (like the Philadelphia chromosome t(9;22)), or infant leukemia (under 1 year old).
A 4-year-old child comes to the clinic with severe leg pain, pale skin, and tiny red spots covering his abdomen. The mother says he has had a fever for two weeks that won't go away. The doctor suspects ALL and orders a bone marrow biopsy.
- What are the tiny red spots called, and why are they happening?
- What percentage of blasts in the bone marrow will confirm the diagnosis of Leukemia?
Answers:
- They are petechiae. They happen because the bone marrow is full of leukemia cells and cannot produce platelets (Thrombocytopenia), leading to micro-hemorrhages under the skin.
- Greater than 25% blasts in the marrow confirms leukemia.
OVERALL GOAL: Kill all leukemia cells, allow normal blood cells to return, and prevent the spread to "sanctuary sites" (the brain/CNS and the testicles, where normal IV chemotherapy cannot easily reach due to the blood-brain and blood-testis barriers).
Purpose: To rapidly kill the vast majority of leukemia cells in the blood and bone marrow and achieve remission (defined as having less than 5% blast cells in the marrow and the return of normal blood counts).
Medicines used (The Induction Regimen):
- Vincristine: IV injection weekly. Mechanism: Stops cells from dividing by inhibiting microtubules. Side effects: Highly neurotoxic. Causes constipation (paralytic ileus), hair loss, and severe nerve pain/damage (burning/tingling, jaw pain, loss of deep tendon reflexes, foot drop). NEVER give intrathecally—it is fatal!
- Prednisone or Dexamethasone: Oral steroids daily. Mechanism: Directly toxic to lymphoid cancer cells (lymphocytotoxic). Side effects: Extreme mood changes (crying, rage), massively increased appetite, weight gain (Cushingoid "moon face"), high blood sugar (steroid-induced diabetes), severe stomach irritation, muscle weakness, and profound susceptibility to infection.
- L-asparaginase: IV or IM injection. Mechanism: Starves the cancer cells of the amino acid asparagine, which they need to survive. Side effects: Severe allergic reactions (anaphylaxis), blood clotting problems, severe pancreas inflammation (pancreatitis - watch for severe abdominal pain), and liver problems.
- Daunorubicin or Doxorubicin (Anthracyclines): IV chemotherapy (the "red drugs"). Mechanism: Damages cancer DNA. Side effects: Severe heart damage (cardiotoxicity)—must be monitored with an echocardiogram before and during treatment. Also causes red urine (teach parents this is NOT blood – just the drug color flushing out), mouth sores, massive hair loss, and low blood counts. Highly vesicant (burns tissue if IV leaks).
- Intrathecal (IT) chemotherapy: Chemotherapy injected directly into the spinal fluid during a lumbar puncture to prevent or treat brain involvement. Medicines used include methotrexate, cytarabine, and hydrocortisone.
- Pathophysiology: During Induction, chemotherapy is highly effective. Millions of leukemia cells burst open (lyse) at the exact same time, releasing their intracellular contents straight into the bloodstream. The kidneys become completely overwhelmed and fail.
- Signs (The 4 Chemical Changes): High potassium (Hyperkalemia), high phosphorus (Hyperphosphatemia), low calcium (Hypocalcemia - because it binds to the high phosphorus), and high uric acid (Hyperuricemia).
- Child may exhibit: Irregular heartbeat/cardiac arrest (from potassium), severe muscle cramps/tetany/seizures (from low calcium), and decreased/cloudy urine (uric acid crystals blocking the kidneys).
- Prevention & Management: Give massive amounts of IV fluids (hyperhydration) before and during chemo to flush kidneys. Give Allopurinol or Rasburicase to destroy/lower uric acid. Monitor electrolytes 2-3 times daily. Monitor urine output hourly. If suspected, notify doctor immediately, increase IV fluids, and prepare for emergency dialysis if kidneys shut down.
Nursing Management During Induction:
- Monitor blood counts daily: Transfuse packed red cells (PRBCs) if hemoglobin < 7 g/dL (or < 8 if symptomatic). Transfuse platelets if < 10,000 or if actively bleeding.
- Infection prevention: Strict hand hygiene! Protect from visitors with colds. Monitor temperature every 4 hours. Start broad-spectrum antibiotics IMMEDIATELY if fever > 38°C (neutropenic fever protocol).
- Nutrition support: Small frequent meals, high-protein foods (eggs, beans, groundnuts, milk if tolerated). Give oral supplements. Crucially, administer anti-nausea medicines (antiemetics like ondansetron, metoclopramide) before meals and before chemo.
- Emotional support: Child may feel scared, parents may be in shock. Provide honest but hopeful information. Allow parents to stay with child constantly.
- Medication administration: Double-check all chemotherapy doses (pediatric doses are strictly calculated by Body Surface Area - BSA, not just weight). Verify with a second RN. Ensure the IV line is patent and has a brisk blood return before pushing drugs to prevent vesicant tissue necrosis.
Purpose: To kill any microscopic, stubborn leukemia cells that survived the induction phase. It uses different drugs to prevent the cancer from mutating and developing resistance.
Additional medicines:
- Cyclophosphamide: IV. Side effects: Profound low blood counts, severe nausea, and bladder irritation (Hemorrhagic Cystitis). Nursing intervention: Give plenty of IV fluids and administer the rescue drug Mesna to bind the toxic metabolites and protect the bladder lining.
- Cytarabine (Ara-C): IV or subcutaneous. Side effects: Fever, mouth sores, eye irritation (chemical conjunctivitis - may need steroid eye drops), and severe neurotoxicity (cerebellar toxicity causing unsteady gait).
- 6-Mercaptopurine (6-MP): Oral daily. Side effects: Low blood counts, severe liver damage (hepatotoxicity).
- Methotrexate: High-dose IV. Mechanism: Blocks folic acid, preventing DNA synthesis. Side effects: Massive mouth sores, kidney damage, liver damage. Nursing intervention: Must give Leucovorin rescue exactly on time to save the patient's normal cells from fatal toxicity, and hydrate aggressively with IV sodium bicarbonate to alkalinize the urine and protect the kidneys.
Nursing Care for Consolidation:
- Monitor for mucositis (mouth sores): Inspect mouth every shift. Use an ultra-soft toothbrush, saline or bicarbonate mouth rinses (NO alcohol-based mouthwashes!). Give topical anesthetic gels before meals. Avoid spicy/acidic/rough foods.
- Monitor liver function: Check for yellow eyes/skin (jaundice), dark urine, and right upper quadrant abdominal pain.
- Ensure aggressive hydration to protect kidneys from methotrexate and cyclophosphamide.
- Monitor for neurotoxicity from high-dose cytarabine: check for confusion, difficulty walking (ataxia), or seizures.
Purpose: To prevent or treat leukemia hiding in the brain and spinal cord behind the blood-brain barrier.
Methods:
- Intrathecal chemotherapy via Lumbar Puncture (as described above).
- Cranial radiation: Only used for high-risk cases or if CNS is already involved. It is rarely used in very young children (under age 3) because it causes permanent, severe brain damage and cognitive stunting.
Nursing Care for Radiation:
- Mark radiation fields with ink (instruct parents DO NOT wash off the marks).
- Protect unaffected areas of the body with lead shields.
- Apply gentle moisturizer to irradiated skin (aloe vera, aqueous cream) – avoid perfumes, powders, or harsh soaps.
- Monitor for skin redness (erythema), peeling, and blistering.
- Monitor for extreme fatigue (somnolence syndrome), headache, and nausea.
- Reassure the child during treatments (they must be alone in the radiation room but can hear you talk through the intercom).
Purpose: To keep the leukemia from coming back (relapse). Cancer cells can go dormant; this long, low-dose phase kills them when they wake up.
Medicines (The "Backbone" Regimen):
- 6-Mercaptopurine (6-MP): Oral every evening. Give on an empty stomach (especially without milk/dairy) for better absorption.
- Methotrexate: Oral or IM weekly.
- Vincristine: IV monthly.
- Prednisone/Dexamethasone: Oral for 5 days every 4 weeks (pulse therapy).
Nursing Care for Maintenance:
- Adherence is life or death: Teach parents to give medicines at home EXACTLY as prescribed. Emphasize: Do not skip doses, do not give extra doses, give at the same time daily.
- Monitor blood counts every 2-4 weeks in the clinic. If neutrophils drop too low, the doctor may temporarily reduce the dose.
- Continue infection precautions.
- Monitor growth and development (long-term steroids can stunt height and weaken bones).
- Support school attendance when blood counts are safe! The child is not contagious and desperately needs social normalcy.
If leukemia returns (relapses), the cells have mutated and become resistant to the standard drugs.
- Action: Requires much more intensive chemotherapy.
- Bone Marrow Transplant (BMT) / Hematopoietic Stem Cell Transplant (HSCT):
- Process: The child receives ultra-high-dose chemotherapy (and sometimes total body radiation) to deliberately destroy 100% of their bone marrow (myeloablation). Then, an infusion of healthy stem cells is given via IV to rescue them.
- Types: Allogeneic (cells from a donor/sibling) or Autologous (the child's own cells collected when they were in remission).
- Nursing care: Strict reverse isolation (positive pressure room). Monitor for Graft-Versus-Host Disease (GVHD) – a deadly complication where the donor's immune cells wake up, realize they are in a foreign body, and attack the child's skin, gut, and liver. Severe infection risk requires a very long hospitalization.
- Neutropenia (Low Neutrophils < 500/μL):
- Risk: Overwhelming, rapid, life-threatening bacterial and fungal infections (Sepsis).
- Signs: Fever > 38°C (100.4°F) is an absolute MEDICAL EMERGENCY in a neutropenic child.
- Management: Draw blood cultures immediately. Start broad-spectrum IV antibiotics within 1 hour (e.g., ceftazidime, piperacillin-tazobactam, meropenem). Add vancomycin if a central line infection is suspected. Add antifungals (amphotericin or voriconazole) if fungal infection is suspected. Monitor closely in the hospital.
- Nursing care: No fresh flowers, dirt, or plants in the room (they carry Aspergillus mold). Cooked food only (no raw fruits/vegetables or unpasteurized dairy if severely neutropenic). Strict hand hygiene. Daily mouth and perineal care. Absolutely NO rectal temperatures, enemas, or suppositories (the rectal mucosa is fragile, and tearing it introduces gut bacteria directly into the blood, causing fatal sepsis).
- Thrombocytopenia (Low Platelets < 20,000/μL):
- Risk: Spontaneous, fatal bleeding, especially in the brain (intracranial hemorrhage) or gut.
- Signs: New bruises, petechiae, bleeding gums, blood in urine/stool, severe headache or changes in consciousness (brain bleed).
- Management: Administer Platelet transfusions. Avoid IM injections (they will cause massive hematomas). Avoid aspirin and ibuprofen (which inhibit platelet function). Use an ultra-soft toothbrush. No contact sports. Apply firm pressure for a full 10 minutes after any needle stick.
- Nursing care: Pad the side rails of the crib/bed. Avoid constipation (give stool softeners, as straining can burst vessels and cause bleeding). Monitor all stool, urine, and emesis for blood. Check skin daily for new bruises.
- Anemia (Low Hemoglobin):
- Signs: Severe pallor, fast heartbeat (tachycardia), shortness of breath, chest pain, extreme fatigue.
- Management: Transfuse packed red blood cells (PRBCs) if symptomatic or if Hb < 7 g/dL.
- Nursing care: Pre-medicate with an antihistamine and paracetamol to prevent allergic/febrile transfusion reactions. Monitor vital signs every 15 minutes for the first hour of transfusion. Watch strictly for fever, rash, back pain, dark urine, or wheezing (signs of a hemolytic transfusion reaction). Give the blood slowly in children with heart problems to avoid fluid overload.
- Tumor Lysis Syndrome (TLS):
- Already described above – remember the classic electrolyte triad: High K+, High Phos, High Uric Acid, Low Ca+. A medical emergency requiring hydration and allopurinol!
- Disseminated Intravascular Coagulation (DIC):
- Especially common in a specific type of AML (the M3 subtype / APML).
- Pathophysiology: The leukemia cells release tissue factor, causing microscopic blood clots all over the body. This uses up all the body's clotting factors, leading to massive, paradoxical bleeding.
- Signs: Bleeding from multiple sites simultaneously, oozing from old IV sites, petechiae, very low blood pressure.
- Management: Replace clotting factors with Cryoprecipitate, Fresh Frozen Plasma (FFP), and platelets. Treat the underlying leukemia immediately.
- Hyperleukocytosis:
- Very high white blood cell count (> 100,000/μL).
- Pathophysiology: The blood becomes physically thick (viscous) like sludge and gets stuck in the microscopic capillaries (Leukostasis).
- Signs: Confusion/coma (brain vessels blocked), difficulty breathing (lung vessels blocked), priapism (painful prolonged erection due to blocked penile veins), stroke symptoms.
- Management: Massive aggressive IV hydration. Careful exchange transfusion or leukapheresis (filtering WBCs out of blood) in specialized centers. Crucial Nursing Note: Avoid transfusing red blood cells initially until the WBC count is lowered, because adding red cells makes the blood thickness (viscosity) even worse and can trigger a stroke!
- ALL: 80-90% cure rate in developed countries. 50-60% cure rate in resource-limited settings (due to late presentation, malnutrition, infection, or abandonment of treatment).
- AML: 60-70% cure rate with intensive treatment (much harsher chemo required).
- Prognosis is generally worse if: Infant age (under 1), extremely high white count at diagnosis, certain bad genetic mutations (Philadelphia chromosome), slow response to the first 4 weeks of treatment, or if the leukemia relapses.
Case: You are the pediatric oncology nurse. You have four patients. Which child must you assess and intervene with FIRST?
- A child on Consolidation chemotherapy complaining of a sore mouth.
- A child in Maintenance phase with a platelet count of 35,000 and two new bruises on his leg.
- A child admitted for Induction therapy who has an Absolute Neutrophil Count (ANC) of 200 and just spiked a temperature of 38.2°C.
- A child receiving IV Vincristine complaining of tingling in their fingers.
Answer: You must see Patient 3 FIRST. A fever in a neutropenic patient is an absolute life-threatening emergency. They can progress to septic shock and die within hours. You have less than 60 minutes to draw blood cultures and hang broad-spectrum IV antibiotics.