Catatonic stupor syndrome in schizophrenic patients
Catatonic schizophrenia is also the same as catatonic stupor syndrome. So before we start with catatonic stupor, let's begin by understanding Schizophrenia😊😊😊
Schizophrenia stands as one of the most severe and debilitating mental illnesses, often characterized by a progressive and chronic course. It impacts approximately 1% of the global population, transcending cultural and socioeconomic boundaries. The term "schizophrenia" was coined in 1908 by the Swiss psychiatrist Eugen Bleuler. He derived the word from the Greek roots "schizo," meaning "split," and "phren," meaning "mind," to describe the fragmentation of mental functions observed in affected individuals, not a "split personality" as is often mistakenly believed.
Schizophrenia is fundamentally a functional psychosis marked by profound disturbances across multiple domains of mental functioning.
- Disturbances in Thinking (Cognition): This can manifest as disorganized thought processes, delusions (fixed false beliefs), and impaired executive function.
- Emotional Dysregulation: Individuals may experience flattened affect (reduced emotional expression), inappropriate emotional responses, or anhedonia (inability to experience pleasure).
- Volitional Impairment: This refers to difficulties in initiating and sustaining goal-directed activities, leading to apathy and lack of motivation.
- Perceptual Aberrations: Hallucinations, particularly auditory ones, are a hallmark symptom, where individuals perceive sensory experiences that are not real.
- Deterioration of Interpersonal Relationships: Social withdrawal, difficulty with social cues, and impaired communication often lead to significant challenges in maintaining relationships.
While the precise etiology of schizophrenia remains unknown (idiopathic), current research strongly suggests a multifactorial interplay of genetic, neurobiological, developmental, and environmental factors. It's not caused by any single factor but rather an interaction of vulnerabilities and stressors.
- Family Studies: Extensive research demonstrates a significantly higher probability of developing schizophrenia among biological relatives of affected individuals compared to the general population. The closer the genetic relationship, the higher the risk.
- Twin Studies: These studies provide compelling evidence for a genetic component. The concordance rate for schizophrenia in monozygotic (identical) twins (sharing 100% of their genes) is substantially higher (often cited as four to six times) than in dizygotic (fraternal) twins (sharing approximately 50% of their genes), even when raised in similar environments. This highlights the strong genetic influence.
- Ventricular Enlargement: Enlargement of the brain's ventricles (fluid-filled cavities) is one of the most consistent findings. This suggests a loss of brain tissue (gray matter) surrounding these areas and is often associated with more severe cognitive impairment and negative symptoms.
- Reduced Gray Matter Volume: Reductions in gray matter density have been observed in various brain regions, including the frontal lobes (involved in executive function), temporal lobes (involved in auditory processing and memory), and hippocampus (involved in memory and emotion).
- Abnormal Brain Connectivity: Disruptions in the connectivity between different brain regions, particularly in neural networks involved in cognitive control, attention, and social processing, are also increasingly recognized.
These factors can contribute to neurodevelopmental vulnerabilities.
- Viral Infections: Exposure to certain viral infections (e.g., influenza) during critical stages of fetal development has been linked to an increased risk.
- Birth Injuries/Complications: Obstetric complications such as oxygen deprivation (hypoxia), low birth weight, and premature birth can also increase vulnerability.
- Nutritional Deficiencies: Maternal malnutrition during pregnancy, particularly deficiencies in essential nutrients, may play a role.
- Alcohol and Substance Abuse: Chronic substance abuse, especially of cannabis and stimulants, can trigger psychotic episodes in vulnerable individuals and worsen the course of the illness.
- Cerebral Vascular Accidents (Strokes): Brain damage from strokes can lead to a range of neurological and psychiatric symptoms.
- Myxedema (Severe Hypothyroidism): Untreated hypothyroidism can cause cognitive and psychiatric symptoms that might be mistaken for or coexist with schizophrenia.
- Parkinsonism: While distinct, some medications used to treat schizophrenia can induce Parkinsonian-like side effects, and some brain pathologies involved in Parkinson's can have psychiatric manifestations.
- Head Injury in Adulthood: Severe head trauma, particularly to the frontal lobes, can sometimes precipitate or unmask psychotic symptoms.
- Cerebral Tumors: Brain tumors can cause a variety of neurological and psychiatric symptoms depending on their location and size.
While not direct causes, certain psychological stressors and family dynamics can interact with biological predispositions.
- Poor Parent-Child Relationships: Extremely critical, hostile, or emotionally unavailable parenting, while not causing schizophrenia, can contribute to higher stress levels and poorer coping mechanisms in individuals already vulnerable.
- Dysfunctional Family Systems: Chronic family conflict, lack of clear communication, and high expressed emotion (criticism, hostility, over-involvement) in the family environment can exacerbate symptoms and increase the risk of relapse.
- Social Drift Hypothesis: Individuals with schizophrenia may "drift" into lower socioeconomic classes due to the debilitating effects of the illness on their education, employment, and social functioning.
- Social Causation Hypothesis: Adverse environmental factors associated with poverty and urban living (e.g., chronic stress, discrimination, limited access to resources, exposure to crime, inadequate nutrition, absence of prenatal care, poor living conditions, congested housing) can act as stressors that trigger or exacerbate schizophrenia in vulnerable individuals.
- Feeling of Hopelessness: The pervasive feeling of hopelessness about improving one's life circumstances, often prevalent in marginalized communities, can contribute to chronic stress and poor mental health outcomes.
- Role of Stress: Stress, whether acute or chronic, does not cause schizophrenia but is widely recognized as a significant contributing factor to the onset of psychotic episodes and relapses in individuals who are genetically or biologically vulnerable. Major life changes, traumatic experiences, and ongoing daily stressors can overwhelm an individual's coping mechanisms and precipitate symptom exacerbation.
While historical classifications often distinguished between "acute" and "chronic" schizophrenia, modern diagnostic frameworks (like the DSM-5-TR) primarily focus on the overall clinical course and symptom presentation over time.
Refers to a sudden and rapid onset of prominent psychotic symptoms, such as delusions, hallucinations, disorganized speech, and severely disorganized or catatonic behavior. These symptoms appear relatively quickly, often over days or weeks, in an individual who may or may not have had prior psychiatric difficulties.
- Abrupt Onset: Symptoms emerge rapidly, often in response to significant stress or a precipitating event.
- Prominent Positive Symptoms: Hallucinations (especially auditory), delusions (persecutory, grandiose, bizarre), and thought disorder are typically very pronounced.
- Good Prognosis (Potentially): Individuals experiencing acute episodes often have a better prognosis, particularly if they receive prompt treatment, had good premorbid functioning (their functioning before the illness began), and have strong social support. They may achieve significant remission of symptoms.
- Affective Symptoms: Can be accompanied by intense anxiety, depression, or even manic-like features during the acute phase.
Describes a prolonged and persistent course of schizophrenia, involving a gradual onset of symptoms and a more enduring presence of both positive and negative symptoms (e.g., apathy, social withdrawal, flattened affect). The illness significantly impacts daily functioning over an extended period.
- Insidious Onset: Often begins subtly with a gradual decline in functioning and an increase in negative symptoms, sometimes years before a full-blown psychotic episode.
- Persistent Symptoms: Symptoms may fluctuate in intensity but are generally present for a long duration, often meeting diagnostic criteria for continuous periods.
- Prominent Negative Symptoms: Characterized by a significant presence of negative symptoms, such as alogia (poverty of speech), avolition (lack of motivation), anhedonia (inability to experience pleasure), and affective flattening.
- Functional Impairment: Often associated with significant and long-lasting impairments in social, occupational, and academic functioning.
- Less Favorable Prognosis: Generally implies a more challenging course with greater difficulty achieving full remission and a higher likelihood of persistent functional deficits.
It is important to note that the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR), published by the American Psychiatric Association, 👉👉eliminated the traditional subtypes of schizophrenia (paranoid, disorganized/hebephrenic, catatonic, undifferentiated, residual). This change was made because these subtypes were found to have limited diagnostic stability, overlapping symptoms, and poor predictive validity for treatment response or outcome.
Instead, the DSM-5-TR focuses on a dimensional approach, assessing the severity of core symptoms (e.g., delusions, hallucinations, disorganized speech, negative symptoms, catatonia) on a spectrum. However, understanding these historical subtypes remains valuable for grasping the diverse clinical presentations of schizophrenia and for comprehending older literature or discussions.
Here are the traditional/old subtypes:
(Historically a contentious diagnosis, often overlapping with prodromal phases or other disorders): Characterized by a slow, insidious onset and a progressive decline in functioning without prominent delusions or hallucinations. It is often considered a less severe form in terms of acute psychotic symptoms but can lead to profound social withdrawal and functional impairment.
- Gradual Onset: Symptoms develop very slowly over years, making it difficult to pinpoint the exact beginning.
- Subtle Behavioral Changes: Individuals exhibit increasing apathy, lack of drive, and disinterest in previously enjoyed activities.
- Odd Behaviors: May include peculiar mannerisms, unconventional speech patterns, or unusual interests.
- Wandering Tendency: Some individuals may become aimless and drift, with no clear purpose or destination.
- Self-Absorbed and Isolated: A profound withdrawal from social interactions, leading to a solitary existence. They become increasingly preoccupied with internal experiences rather than external reality.
- Idle and Aimless Activity: Lacks initiative and engagement in productive activities; behavior often appears purposeless.
- Onset: Typically observed in late adolescence or early adulthood, often between the late 20s and early 30s.
- Absence of Prominent Psychosis: Distinct from other subtypes in its lack of clear-cut delusions or hallucinations, making diagnosis challenging and sometimes leading to misdiagnosis as personality disorders or severe depression.
Characterized by prominent disorganized speech and behavior, and a markedly inappropriate or flattened affect. Delusions and hallucinations, if present, are typically fragmented and not systematized.
- Onset: Tends to have an early onset, usually between the ages of 15 and 25 years, often during adolescence or early adulthood, coinciding with critical developmental stages.
- Insidious Onset: Similar to simple type, the onset is often gradual, with a slow deterioration of personality and functioning.
- Disorganized Speech (Thought Disorder): Speech is incoherent, tangential, associative loose, or completely incomprehensible (word salad).
- Disorganized Behavior: Behavior is aimless, unpredictable, and often inappropriate for the situation. It can range from silliness and giggling to severe agitation.
- Extreme Social Impairment: Significant difficulty maintaining relationships, engaging in meaningful social interactions, and fulfilling social roles.
- Poor Premorbid Personality: Often associated with a history of social awkwardness, introversion, and academic difficulties prior to the onset of the illness.
- Chronic Course: Tends to follow a chronic and deteriorating course, with significant functional decline.
- Regressive and Primitive Behavior: Individuals may exhibit childlike behaviors, neglect personal hygiene, and engage in socially inappropriate acts.
- Loss of Contact with Reality: Contact with external reality is severely impaired or lost, leading to a subjective world dominated by internal experiences.
- Mood is Inappropriate/Flattened: Affect is often incongruous with the content of speech or situation (e.g., laughing at a tragic event) or markedly flattened and unresponsive.
- Characteristic Affective/Behavioral Manifestations:
- Silly laughter and giggling without apparent reason.
- Bizarre mannerisms and grimaces.
- Neglected personal hygiene and grooming.
- Extreme social impairment, making independent living challenging.
Characterized by a preoccupation with one or more delusions (often persecutory or grandiose) or frequent auditory hallucinations, in the absence of prominent disorganized speech, disorganized behavior, or flat/inappropriate affect.
- Dominant Symptoms: The defining characteristic is the presence of well-formed, often systematized delusions, typically of persecution (belief that one is being harmed or conspired against) or grandeur (exaggerated belief in one's own importance or abilities).
- Auditory Hallucinations: Frequent auditory hallucinations, often voices conversing with each other or commenting on the individual's thoughts or actions.
- Suspiciousness and Mistrust: Individuals are often profoundly suspicious of others, leading to social isolation and difficulty trusting even close family members or healthcare providers.
- Hostility and Aggression: Due to their delusions of persecution, individuals can become hostile, irritable, and occasionally aggressive when they perceive threats or feel their beliefs are challenged.
- Tension and Agitation: Often experience high levels of tension, anxiety, and agitation stemming from their internal experiences.
- Argumentative: May engage in frequent arguments, especially when their delusional beliefs are questioned.
- Later Onset: Typically has a later age of onset compared to other subtypes, often in the 20s or 30s.
- Less Regression in Mental Faculties: Compared to disorganized type, individuals with paranoid schizophrenia tend to maintain better intellectual and emotional functioning, at least initially. Their cognitive abilities might be relatively preserved outside of their delusional system.
- Preserved Emotional and Behavioral Responses: While their beliefs are distorted, their emotional responses and overall behavior might appear more congruent and less overtly disorganized than in the hebephrenic type. This often leads to a relatively better prognosis and higher level of functioning in some areas.
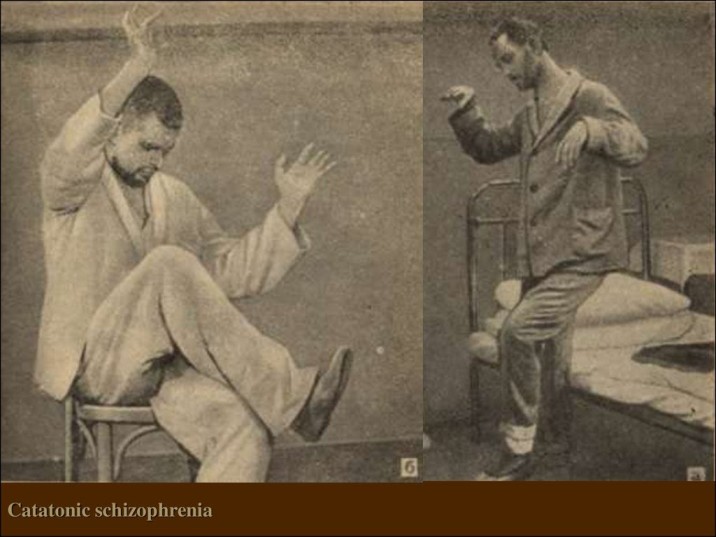
Primarily characterized by marked disturbances in psychomotor behavior, which can range from extreme immobility (stupor) to excessive motor activity (excitement), often in a seemingly purposeless manner.
- Motor Abnormalities: The defining feature is a profound disturbance in voluntary movement.
- Stupor (Decreased Motor Activity):
- Catalepsy: Passive induction of a posture held against gravity (e.g., if an arm is lifted, it remains there).
- Waxy Flexibility: A decrease in response to stimuli and a tendency to remain in an immobile posture, often described as a "waxy" resistance to movement.
- Mutism: Absence or very little verbal response (not due to aphasia).
- Negativism: Opposition to instructions or external stimuli, or resistance to passive movement.
- Posturing: Spontaneous and active maintenance of a posture against gravity.
- Grimacing: Distorted facial expressions.
- Echolalia: Mimicking another's speech.
- Echopraxia: Mimicking another's movements.
- Excitement (Increased Motor Activity):
- Catatonic Agitation: Apparently purposeless and excessive motor activity not influenced by external stimuli.
- Stereotypy: Repetitive, abnormally frequent, non-goal-directed movements.
- Mannerisms: Odd, circumstantial caricatures of normal actions.
- Combativeness: Can become physically aggressive, especially if attempts are made to alter their position or restrain them.
- Associated Symptoms: Can include bizarre delusions, hallucinations, and rapid shifts between states of stupor and excitement.
- Medical Emergency: Severe catatonia can be a medical emergency due to associated risks like dehydration, malnutrition, and self-injury, often requiring hospitalization and rapid intervention (e.g., benzodiazepines, electroconvulsive therapy).
The DSM-5-TR now views schizophrenia as a single disorder on a spectrum of severity, characterized by specific core symptoms. The diagnosis of "Schizophrenia" itself requires the presence of at least two of the following symptoms for a significant portion of time during a one-month period (or less if successfully treated), with at least one of these being delusions, hallucinations, or disorganized speech:
- Delusions
- Hallucinations
- Disorganized Speech (e.g., frequent derailment or incoherence)
- Grossly Disorganized or Catatonic Behavior
- Negative Symptoms (i.e., diminished emotional expression or avolition)
The DSM-5-TR emphasizes assessing the severity of these individual symptoms on a dimensional scale (e.g., from 0 to 4, where 0 is not present and 4 is severe). This allows for a more nuanced description of each patient's unique presentation.
- With Catatonia: Catatonia is no longer a subtype of schizophrenia but rather a specifier that can be applied to schizophrenia (and other mental disorders, such as bipolar disorder or major depressive disorder) when certain catatonic symptoms are present.
- First Episode, Currently in Acute Episode; First Episode, Currently in Partial Remission; First Episode, Currently in Full Remission: These describe the stage and current status of the illness.
- Multiple Episodes, Currently in Acute Episode; Multiple Episodes, Currently in Partial Remission; Multiple Episodes, Currently in Full Remission: For individuals who have experienced more than one episode.
- Continuous: If symptoms have been continuously present for the past year.
- With Unspecified Catatonia: If catatonic symptoms are present but don't meet the full criteria for the "with catatonia" specifier.
- With Other Specified Catatonia: For other forms of catatonia.
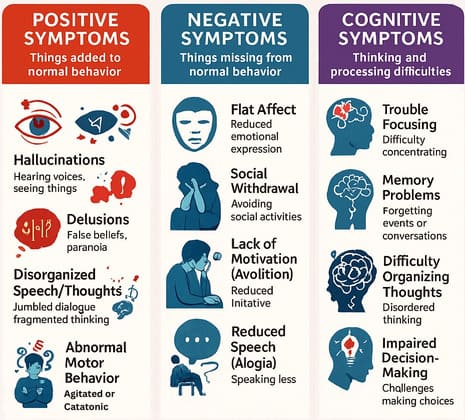
These are experiences and behaviors that are added to a person's normal mental life and are often considered the hallmark of psychosis.
- Persecutory Delusions: Belief that one is going to be harmed, harassed, plotted against.
- Grandiose Delusions: Belief that one has exceptional abilities, wealth, or fame.
- Referential Delusions: Belief that certain gestures, comments, environmental cues are directed at oneself.
- Somatic Delusions: Preoccupations regarding health and organ function.
- Erotomanic Delusions: Belief that another person is in love with them.
- Nihilistic Delusions: Belief that a major catastrophe will occur.
- Control Delusions (Passivity Phenomena):
- Thought Insertion: Belief that one's thoughts have been placed into one's mind by an external source.
- Thought Withdrawal: Belief that thoughts have been removed from one's mind by an external force.
- Thought Broadcasting: Belief that one's private thoughts are being transmitted to others.
- Auditory Hallucinations: The most common type.
- Visual Hallucinations: Seeing things that are not present.
- Olfactory Hallucinations: Smelling odors that are not present.
- Gustatory Hallucinations: Tasting flavors that are not present.
- Tactile (Somatic) Hallucinations: Feeling sensations on or under the skin.
These refer to deficits in normal emotional responses or other thought processes. They are taken away from a person's mental life.
- Affective Flattening/Diminished Emotional Expression: Reduction in the range and intensity of emotional expression.
- Alogia (Poverty of Speech): A lessening of speech fluency and productivity.
- Avolition: Reduction, difficulty, or inability to initiate and persist in goal-directed activities.
- Anhedonia: The inability to experience pleasure in activities.
- Asociality: Apparent lack of interest in social interactions.
- Loosening of Associations/Derailment: Shifting from one topic to another without logical connection.
- Tangentiality: Answering questions obliquely or only slightly related.
- Incoherence ("Word Salad"): Speech that is nearly incomprehensible.
- Neologisms: The creation of new, meaningless words.
- Clanging: Speech governed by sound (e.g., rhyming).
- Echolalia: Meaningless repetition of another person's spoken words.
- Difficulty in Goal-Directed Behavior: Leading to impairments in activities of daily living.
- Unpredictable Agitation or Silliness.
- Social Disinhibition.
- Bizarre Behaviors.
- Neglected Personal Hygiene.
- Wandering Tendency.
- Regression.
- Flexibilitas Cerea (Waxy Flexibility): The capacity to maintain the limbs or other bodily parts in whatever position they have been placed.
- Catalepsy: Passive induction of a posture held against gravity.
- Echopraxia: Mimicking another person's movements.
- Stupor: Lack of psychomotor activity.
- Mutism: Absence or very little verbal response.
- Posturing: Spontaneous and active maintenance of a posture against gravity.
- Negativism: Opposition to instructions or external stimuli.
- Stereotypy: Repetitive, abnormally frequent, non-goal-directed movements.
- Agitation: Apparently purposeless and excessive motor activity.
- Grimacing: Distorted facial expressions.
- Lack of Insight (Anosognosia).
- Disturbed Mood.
- Social Withdrawal/Isolation.
- Neglected Personal Hygiene.
- Acute and Later Onset (e.g., after age 30).
- Obvious Precipitating Factor.
- Good Premorbid Functioning.
- Presence of Affective Symptoms.
- Married Status.
- Family History of Mood Disorder.
- Good Support System.
- Predominance of Positive Symptoms.
- Insidious and Younger Onset.
- No Precipitating Factors.
- Poor Premorbid Social and Work History.
- Withdrawn/Isolated Premorbid Personality.
- Single, Divorced, or Widowed Status.
- Family History of Schizophrenia.
- Poor Support System.
- Predominance of Negative Symptoms.
- Prominent Cognitive Deficits.
- Substance Abuse Comorbidity.
While not used as primary diagnostic criteria in current systems like DSM-5-TR, Schneider's First-Rank Symptoms (FRS) remain historically significant.
- Hearing one's thoughts spoken aloud (Gedankenlautwerden).
- Hearing voices referring to oneself in the third person.
- Auditory hallucinations in the form of a commentary.
- Thought Withdrawal.
- Thought Insertion.
- Thought Broadcasting.
- Feelings or actions experienced as made or influenced by external agents.
- Building a Therapeutic Relationship: Establish trust and rapport, maintain a consistent approach, respect boundaries.
- Education and Psychoeducation: Educate patient/family, provide clear info on meds.
- Reality Orientation and Validation: Consistently maintain focus on reality, do not argue with delusions, minimize environmental stimuli.
- Meeting Basic Needs and Safety: Ensure nutrition/hygiene, prioritize safety from self-harm/aggression.
- Emotional Regulation and Communication: Avoid highly expressed emotions (criticism, hostility), encourage clear communication.
- Interdisciplinary Team: Nurse, psychiatrist, social worker, OT, psychologist.
- Treatment Adherence: Ensure adherence to plan.
- Medication Management: Administer meds, educate, plan for side effects.
- Crisis Intervention: Manage aggression/agitation.
- Advocacy: Advocate for rights and access.
- Psychotherapy (Individual and Group): CBT for Psychosis, Supportive Psychotherapy, Group Therapy.
- Social Skills Training (SST): Teach essential social behaviors.
- Behavior Therapy/Modification: Reduce maladaptive behaviors.
- Family Psychoeducation and Therapy: Reduce expressed emotion, improve communication.
- Occupational Therapy (OT): Improve functional skills (ADLs/IADLs).
- Antipsychotic Medications:
- First-Generation Antipsychotics (FGAs): Chlorpromazine, Haloperidol, Trifluoperazine, Thioridazine.
- Second-Generation Antipsychotics (SGAs): Risperidone, olanzapine, quetiapine, ziprasidone, aripiprazole, lurasidone, paliperidone.
- Long-Acting Injectables (LAIs).
- Clozapine: For treatment-resistant schizophrenia.
- Adjunctive Medications: Anticholinergics (e.g., Artane), Mood Stabilizers, Antidepressants.
- Electroconvulsive Therapy (ECT): For severe, treatment-resistant cases or prominent catatonia.
- Vocational Rehabilitation.
- Supported Education.
- Social Skills Training.
- Habit Training.
- Community Integration.
- Medication Adherence.
- Follow-up Appointments.
- Relapse Prevention Plan.
- Support Systems.
- Stigma Reduction.
- Crisis Plan.
- Functional Independence.
- Healthy Lifestyle.
Catatonia is a severe neuropsychiatric syndrome characterized by profound disturbances in psychomotor behavior. It is no longer considered a subtype of schizophrenia in the DSM-5-TR but rather a specifier that can occur in the context of various mental disorders (e.g., schizophrenia, bipolar disorder, major depressive disorder) and certain medical conditions.
"Catatonic Stupor Syndrome" specifically refers to the presentation of catatonia where stupor is a prominent feature. In this state, an individual is largely unresponsive to their environment, may appear "frozen" in a particular posture, have greatly reduced or absent spontaneous movements, and exhibit mutism. It is a severe manifestation of catatonia and can be life-threatening if not managed due to risks of dehydration, malnutrition, and medical complications from immobility.
A diagnosis of catatonia requires the presence of three or more of the following 12 psychomotor symptoms:
- Stupor: Marked decrease in psychomotor activity; the individual is not actively relating to the environment. This is often what people colloquially refer to as "catatonic stupor."
- Catalepsy: Passive induction of a posture held against gravity. If an arm is lifted, it remains in that position for an extended period.
- Waxy Flexibility (Flexibilitas Cerea): A specific type of catalepsy where there is a slight, even resistance to positioning by the examiner. The limbs or other body parts can be placed in an awkward position and will be maintained there for a prolonged time, much like a wax statue.
- Mutism: No, or very little, verbal response (not due to aphasia or other communication impairment).
- Negativism: Opposition to instructions or external stimuli, or resistance to passive movement.
- Posturing: Spontaneous and active maintenance of a posture against gravity that is often bizarre or uncomfortable.
- Mannerism: Odd, circumstantial caricatures of normal actions (e.g., repeatedly saluting for no reason).
- Stereotypy: Repetitive, abnormally frequent, non-goal-directed movements (e.g., rocking back and forth, head banging).
- Agitation (not influenced by external stimuli): Apparently purposeless and excessive motor activity (this aligns with "Catatonic Excitement").
- Grimacing: Making strange or contorted facial expressions.
- Echolalia: Meaningless repetition of another person's spoken words.
- Echopraxia: Meaningless repetition of another person's movements.
Catatonia can manifest in two contrasting clinical pictures, though these can rapidly fluctuate within the same individual:
- Description: Characterized by a severe reduction or absence of psychomotor activity. The patient is almost entirely unresponsive to external stimuli and may appear "frozen."
- Symptoms Often Present: Profound stupor, mutism, negativism, waxy flexibility, catalepsy, and posturing.
- Awareness: Despite the apparent unresponsiveness, patients in a catatonic stupor are often fully or partially aware of their surroundings and what is happening, which can be extremely distressing. This is a crucial point that differentiates it from a coma or other states of unconsciousness.
- Risk: Can be a life-threatening condition due to the risks of dehydration, malnutrition, aspiration, deep vein thrombosis, and pressure sores from immobility.
- Depressive Stupor: When catatonia, particularly with prominent stupor, occurs in the context of Major Depressive Disorder, it may be referred to as depressive stupor.
- Description: Manifested by extreme psychomotor agitation, restlessness, and purposeless motor activity that is not influenced by external stimuli.
- Symptoms Often Present: Agitation, restlessness, stereotypies, mannerisms, grimacing, and often incoherent speech.
- Risk: Can be dangerous due to the potential for self-harm, aggression towards others, exhaustion, and physical injury.
The exact neurobiological mechanisms underlying catatonia are not fully understood, but several hypotheses exist, often involving dysregulation of key neurotransmitter systems:
- GABAergic Dysfunction:
- This is the most widely accepted hypothesis. Catatonia is thought to be associated with an acute decrease in GABAergic (gamma-aminobutyric acid) activity in specific brain regions, particularly the motor circuits.
- The strong and rapid response of catatonia to benzodiazepines (which enhance GABAergic activity) supports this theory.
- Dopamine Dysregulation:
- Hypodopaminergia: Some theories suggest a state of reduced dopaminergic activity in catatonia, particularly in the basal ganglia. This aligns with conditions like Parkinson's disease (a hypodopaminergic state) that can present with catatonic-like features.
- Hyperdopaminergia (less direct for stupor): While schizophrenia itself is often associated with hyperdopaminergia, the development of catatonia in this context might represent a complex interplay or even a compensatory hypodopaminergic state in certain circuits, perhaps exacerbated by antipsychotic use.
- Glutamate Dysregulation:
- Abnormalities in glutamate, the brain's primary excitatory neurotransmitter, particularly within the N-methyl-D-aspartate (NMDA) receptor system, are also implicated. Conditions like anti-NMDA receptor encephalitis can cause profound catatonia.
- Other Neurotransmitters: Serotonin, norepinephrine, and acetylcholine systems may also play roles in the complex neural networks involved in motor control and behavioral regulation.
Catatonia is not a standalone diagnosis but rather a syndrome that results from various underlying conditions. Identifying the cause is paramount for appropriate treatment.
Catatonia is most commonly associated with psychiatric disorders.
- Schizophrenia: Historically the primary association, now specified as "Schizophrenia, With Catatonia."
- Mood Disorders: Catatonia is actually more common in severe mood disorders than in schizophrenia.
- Bipolar Disorder: Especially during severe manic or depressive episodes.
- Major Depressive Disorder: (e.g., Depressive Stupor).
- Other Psychotic Disorders: Such as schizoaffective disorder.
- Autism Spectrum Disorder: Catatonic features can occur in individuals with autism.
- Other Severe Mental Illnesses: Obsessive-compulsive disorder, post-traumatic stress disorder, eating disorders.
A wide range of medical conditions can induce catatonia, and it's essential to rule these out.
- Neurological Disorders: Encephalitis (especially anti-NMDA receptor encephalitis), Parkinson's disease, seizure disorders (non-convulsive status epilepticus), traumatic brain injury, stroke, brain tumors.
- Systemic Medical Conditions: Severe infections, metabolic derangements (e.g., diabetic ketoacidosis, electrolyte imbalances, hepatic or renal failure), autoimmune disorders, certain vitamin deficiencies (e.g., B12).
- Toxins/Substances: Illicit drugs (e.g., PCP, stimulants), alcohol withdrawal, heavy metal poisoning.
- Antipsychotics: Can induce catatonia, particularly in vulnerable individuals, or in the context of Neuroleptic Malignant Syndrome (NMS), which is a severe and potentially fatal reaction.
- Other Medications: Corticosteroids, disulfiram, some antibiotics.
- Underlying Psychiatric Illness: As listed above, particularly severe mood disorders or psychotic disorders.
- Genetic Predisposition: Family history of psychiatric disorders or catatonia.
- Substance Misuse: Can precipitate or exacerbate catatonic episodes.
- Discontinuation of Medications: Abrupt withdrawal from certain medications (e.g., benzodiazepines).
- Severe Stressors: Extreme psychological or physical stress.
Diagnosing catatonia requires a comprehensive evaluation, as its symptoms can overlap with other conditions. There are no specific lab tests for catatonia itself, but tests are used to identify underlying causes.
- Psychiatric Examination: A thorough evaluation by a psychiatrist using standardized rating scales (e.g., Bush-Francis Catatonia Rating Scale) to assess for the presence and severity of catatonic symptoms.
- Bush-Francis Catatonia Rating Scale (BFCRS):
- Structure: Consists of 23 items. The first 14 items are for diagnosis (each item scored 0 or 1 for presence/absence). The remaining items provide a severity rating for the 14 diagnostic items if present.
- Diagnostic Criteria: A diagnosis of catatonia is supported by the presence of at least 2 items from the first 14 (some guidelines suggest 3, aligning with DSM-5).
- Physical Examination: To identify any medical signs or neurological deficits.
It's crucial to differentiate catatonia from other conditions that might present similarly:
- Movement Disorders:
- Tardive Dyskinesia: Involuntary, repetitive movements resulting from long-term use of certain medications (e.g., antipsychotics). Catatonia typically involves voluntary but abnormal postures/movements, whereas TD is involuntary.
- Tourette's Syndrome: Characterized by tics (sudden, repetitive, nonrhythmic motor movements or vocalizations).
- Dystonia: Sustained or intermittent muscle contractions causing abnormal, often repetitive, movements and postures.
- Non-convulsive Status Epilepticus: A seizure disorder where individuals may appear stuporous or confused without overt convulsions.
- Malingering: Feigning symptoms for external gain.
- Delirium or Coma: States of altered consciousness with global brain dysfunction. Catatonia, especially stupor, is distinct from these as the patient is often internally aware.
- Electroencephalogram (EEG): To rule out non-convulsive status epilepticus or other neurological abnormalities.
- MRI or CT Scan of the Brain: To identify structural brain abnormalities, tumors, or signs of inflammation.
- Blood Tests: To check for metabolic imbalances, infections, autoimmune markers, and drug levels.
- Cerebrospinal Fluid (CSF) Analysis: May be performed to look for infectious or autoimmune causes (e.g., encephalitis).
Catatonic stupor is a medical emergency due to the significant risk of medical complications from prolonged immobility and lack of self-care.
- Regularly monitor temperature, pulse, respiratory rate, blood pressure, and oxygen saturation.
- Monitor for signs of autonomic instability (suggesting NMS or other medical issues).
- Monitor fluid intake and output.
- Patients in stupor are often unable to feed or drink.
- Intravenous fluids (IV fluids): Essential to prevent dehydration.
- Nutritional Support: Nasogastric (NG) tube feeding or parenteral nutrition may be required if the stupor is prolonged.
- Prolonged immobility significantly increases the risk of DVT and subsequent pulmonary embolism (PE), which can be fatal.
- Measures: Sequential compression devices (SCDs), elastic compression stockings, and low-molecular-weight heparin (LMWH) or unfractionated heparin.
- Frequent repositioning: Also aids in circulation.
- Frequent repositioning (every 2 hours if possible).
- Use of pressure-relieving mattresses and cushions.
- Skin care to keep it clean and dry.
- Monitor for urinary retention (bladder scan, catheterization if necessary).
- Monitor for constipation or fecal impaction.
- Ensure proper hygiene.
- Elevate the head of the bed, especially if NG feeding is in place.
- Monitor for signs of aspiration.
- Immediately treat any medical conditions identified during the differential diagnosis (e.g., fluid and electrolyte imbalances, infections, NMS, NCSE). For instance, if NCSE is diagnosed, anticonvulsants are the primary treatment. If NMS, discontinue antipsychotics, provide supportive care, and consider dantrolene or bromocriptine.
The cornerstone of acute catatonia treatment involves benzodiazepines and, if necessary, ECT.
- Purpose: This is both diagnostic and therapeutic. A positive response confirms the diagnosis of catatonia and guides ongoing treatment.
- Procedure: Administer Lorazepam 1-2 mg intramuscularly (IM) or intravenously (IV).
- Response: Observe the patient for 15-30 minutes. A positive response is characterized by a significant, albeit temporary, reduction in catatonic symptoms (e.g., improved eye contact, ability to follow commands, reduced rigidity, less mutism). Even a partial response is considered positive.
- Dosing: If there is a positive response, Lorazepam can be repeated every 4-6 hours, titrating the dose upward (e.g., 2 mg, 4 mg, 6 mg IM/IV) until symptoms resolve or side effects (e.g., excessive sedation, respiratory depression) become prohibitive. Some patients may require high doses (e.g., 8-12 mg/day or even higher).
- Maintenance: Once acute catatonia resolves, the patient may need oral lorazepam, which can be slowly tapered over days to weeks while other definitive treatments for the underlying condition (e.g., antipsychotics for schizophrenia) are initiated.
- Failure of Benzodiazepines: If there is no significant response to adequate doses of benzodiazepines within 24-48 hours.
- Severe or Life-Threatening Catatonia: If the patient's physical health is deteriorating rapidly (e.g., due to severe dehydration, NMS-like features, or prolonged immobility leading to complications), ECT should be considered early, potentially even before a full trial of high-dose benzodiazepines.
- Catatonia with Malignant Features: (e.g., high fever, autonomic instability, severe rigidity) where NMS cannot be definitively ruled out or is co-occurring.
- Antipsychotics should generally be withheld until catatonic symptoms have significantly improved or resolved with benzodiazepines or ECT.
- Once catatonia is improving, a low dose of an atypical antipsychotic (e.g., risperidone, olanzapine, quetiapine, or clozapine) can be cautiously introduced and slowly titrated upwards to manage the underlying schizophrenia symptoms. Atypicals are generally preferred due to a lower risk of extrapyramidal side effects and NMS compared to typicals.
Beyond the medical and pharmacological interventions, ongoing supportive care is vital.
- Continued monitoring and prevention of complications (as outlined in Immediate Interventions).
- Regular bathing, oral care, skin care.
- Even if mute, the patient may be conscious and aware. Speak to them calmly, explain procedures, and reassure them.
- Assume they can hear and understand.
- Use simple, clear language.
- Once responsive, explore their experience of the catatonic state.
- Provide a safe, quiet, and low-stimulation environment to minimize agitation or overstimulation.
The long-term management of catatonic stupor in the context of schizophrenia involves two main aspects: treating the underlying schizophrenia and preventing recurrence of catatonia.
- Maintenance Antipsychotic Therapy: Continuation of an antipsychotic (usually atypical, at the lowest effective dose).
- Psychotherapy: (e.g., CBT, supportive therapy) to address psychotic symptoms, improve coping skills, and enhance social functioning.
- Psychoeducation: For the patient and family about schizophrenia and its management.
- Social Skills Training and Vocational Rehabilitation: To improve functional outcomes.
- Continue Treatment of Underlying Schizophrenia: Effective management of schizophrenia is crucial, as uncontrolled psychosis can trigger catatonia.
- Avoid Precipitating Factors: Identify and, if possible, avoid factors that may have triggered the catatonic episode (e.g., certain medications, stressors).
- Education: Educate the patient and family about the early signs of catatonia so that prompt intervention can be sought if symptoms recur.
- Consider Maintenance Benzodiazepines (in some cases): For patients with recurrent catatonia, a low dose of a long-acting benzodiazepine (e.g., clonazepam) might be considered as a preventative measure, but this is less common and must be carefully weighed against risks of dependence.
- Regular Monitoring: Ongoing assessment for any re-emergence of catatonic symptoms.
Catatonic stupor syndrome in schizophrenic patients Read More »