Mood Disorders in Children and Adolescents
In psychiatry, mood disorders (also known as affective disorders) are a group of mental health conditions characterized by a significant disturbance in a person's emotional state or mood.
This disturbance is severe enough to cause considerable distress and impair functioning in various aspects of life, such as school, family, social relationships, and daily activities.
For children and adolescents, these mood disturbances are often expressed differently than in adults, making diagnosis challenging. While adults might overtly express sadness or euphoria, youth might present with irritability, somatic complaints, behavioral problems, or school refusal.
The key feature is a sustained change in mood that represents a departure from the individual's typical emotional baseline and is not attributable to a transient situation or normal emotional fluctuations.
Primary Mood Disorders in Children and Adolescents:
The primary mood disorders we focus on are depressive disorders and bipolar disorders.
A. Depressive Disorders:
These are characterized by persistent sadness, loss of interest or pleasure (anhedonia), and a range of associated emotional, cognitive, behavioral, and physical symptoms.
- Major Depressive Disorder (MDD): Characterized by one or more Major Depressive Episodes. A Major Depressive Episode involves a period of at least two consecutive weeks where an individual experiences five or more of the following symptoms, with at least one symptom being either (1) depressed mood or (2) loss of interest or pleasure:
- Depressed mood most of the day, nearly every day (often irritable mood in children/adolescents).
- Markedly diminished interest or pleasure in all, or almost all, activities most of the day, nearly every day.
- Significant unintentional weight loss or gain, or decrease/increase in appetite.
- Insomnia or hypersomnia nearly every day.
- Psychomotor agitation or retardation nearly every day.
- Fatigue or loss of energy nearly every day.
- Feelings of worthlessness or excessive or inappropriate guilt nearly every day.
- Diminished ability to think or concentrate, or indecisiveness, nearly every day.
- Recurrent thoughts of death, recurrent suicidal ideation without a specific plan, or a suicide attempt or a specific plan for committing suicide.
In Youth: Depressed mood is often manifested as irritability, anger, or temper outbursts rather than overt sadness. Other common presentations include social withdrawal, academic decline, somatic complaints (headaches, stomachaches), and an increase in disruptive behaviors. - Persistent Depressive Disorder (PDD) / Dysthymia:
- Core Feature: A chronic form of depression, characterized by a depressed mood (or irritable mood in children/adolescents) for most of the day, for more days than not, for at least one year (for children and adolescents; two years for adults).
- Symptoms: While less severe than MDD, individuals experience at least two additional depressive symptoms (e.g., poor appetite/overeating, insomnia/hypersomnia, low energy/fatigue, low self-esteem, poor concentration/difficulty making decisions, feelings of hopelessness).
- In Youth: Can be insidious in onset and often perceived as part of the child's "personality," leading to delayed diagnosis. Impairs functioning over a prolonged period.
B. Bipolar Disorders:
These are characterized by significant mood swings that include episodes of both depression and abnormally elevated, expansive, or irritable mood (mania or hypomania).
- Bipolar I Disorder: Defined by the occurrence of at least one Manic Episode. A Manic Episode is a distinct period of abnormally and persistently elevated, expansive, or irritable mood and abnormally and persistently increased goal-directed activity or energy, lasting at least one week and present most of the day, nearly every day.
- Symptoms: During this period, three or more of the following symptoms (four if the mood is only irritable) are present to a significant degree and represent a noticeable change from usual behavior:
- Inflated self-esteem or grandiosity.
- Decreased need for sleep.
- More talkative than usual or pressure to keep talking.
- Flight of ideas or subjective experience that thoughts are racing.
- Distractibility.
- Increase in goal-directed activity or psychomotor agitation.
- Excessive involvement in activities that have a high potential for painful consequences (e.g., unrestrained buying sprees, sexual indiscretions, foolish business investments).
- In Youth: Manic episodes in children and adolescents often present with severe irritability, explosive temper outbursts, aggressive behavior, rapid mood shifts, and distractibility rather than classic euphoria. Grandiosity might involve exaggerated claims of ability or possessions. Psychotic features can occur. Depressive episodes also typically occur.
- Symptoms: During this period, three or more of the following symptoms (four if the mood is only irritable) are present to a significant degree and represent a noticeable change from usual behavior:
- Bipolar II Disorder: Defined by at least one Hypomanic Episode and at least one Major Depressive Episode. A Hypomanic Episode is similar to a manic episode but is less severe and shorter in duration (at least four consecutive days). It does not cause marked impairment in social or occupational functioning or necessitate hospitalization.
In Youth: Often presents with chronic or recurrent depression punctuated by episodes of elevated energy, decreased need for sleep, and irritability. Hypomanic episodes can be easily missed or misinterpreted as normal "highs" or behavioral problems.
- Cyclothymic Disorder: A chronic, fluctuating mood disturbance involving numerous hypomanic symptoms and numerous depressive symptoms for at least one year (for children and adolescents; two years for adults), that do not meet the full criteria for a hypomanic or major depressive episode.
- In Youth: Characterized by recurrent mood swings that are less extreme but more persistent than those in Bipolar I or II.
- Premenstrual Dysphoric Disorder (PMDD): This includes depressive symptoms, irritability, and tension before menstruation.
Consideration for Children/Adolescents: PMDD is primarily diagnosed in post-menarcheal adolescents and adult women. While it can certainly affect adolescent females, especially after the onset of regular menstrual cycles, it's generally considered a diagnosis for individuals who are experiencing regular menstruation. Its symptoms are specifically timed to the luteal phase of the menstrual cycle and remit shortly after the onset of menses. It would be an important consideration for adolescent girls presenting with cyclical mood symptoms.
- Mood Disorder Due to a General Medical Condition: Many medical illnesses, including cancer, injuries, and chronic medical illnesses, can trigger symptoms of depression.
Consideration for Children/Adolescents: This is absolutely critical in pediatric and adolescent psychiatry. Any child or adolescent presenting with mood symptoms must undergo a thorough medical workup to rule out underlying medical causes.
Examples include:
- Endocrine disorders: Thyroid dysfunction, diabetes.
- Neurological conditions: Epilepsy, traumatic brain injury, multiple sclerosis.
- Chronic illnesses: Autoimmune diseases (e.g., lupus), cancer, chronic pain conditions, inflammatory bowel disease.
- Nutritional deficiencies: Vitamin D, B12 deficiency.
- Infections: Post-viral syndromes.
The key here is that the mood disturbance is judged to be a direct physiological consequence of another medical condition.
- Substance-Induced Mood Disorder: Symptoms of depression due to drug use, the effects of a medication, or exposure to toxins.
Consideration for Children/Adolescents: Highly relevant for adolescents. Substance use (alcohol, cannabis, stimulants, opioids, hallucinogens, etc.) can both induce mood symptoms (depressive or manic-like) and exacerbate pre-existing mood disorders. Certain prescribed medications (e.g., corticosteroids, some acne medications like isotretinoin, certain antihypertensives) can also cause mood side effects. Exposure to environmental toxins is less common but possible. A thorough substance use history and medication review are essential during assessment. The mood disturbance must develop during or soon after substance intoxication or withdrawal, or after exposure to a medication/toxin, and the involved substance must be capable of producing the symptoms.
Differentiating Primary Mood Disorders from Mood Dysregulation:
This distinction is particularly important with the introduction of a new diagnosis in DSM-5.
1. Disruptive Mood Dysregulation Disorder (DMDD):
DMDD was introduced in DSM-5 to address concerns about the overdiagnosis of Bipolar Disorder in children, especially those with chronic, severe irritability and temper outbursts, who did not experience distinct, episodic mania/hypomania.
- Core Features:
- Severe Recurrent Temper Outbursts: Outbursts are grossly out of proportion in intensity or duration to the situation or provocation, occur frequently (three or more times per week), and are inconsistent with developmental level.
- Persistent Irritable or Angry Mood: Present most of the day, nearly every day, between temper outbursts.
- Duration: Symptoms must be present for at least 12 months, without a period of 3 or more consecutive months without all symptoms.
- Onset: Onset before age 10, with diagnosis not made before age 6 or after age 18.
- Exclusivity: The diagnosis cannot coexist with Bipolar Disorder or Oppositional Defiant Disorder (ODD), though it can coexist with MDD, anxiety disorders, and ADHD.
- Key Differentiation from Bipolar Disorder: DMDD is characterized by chronic, inter-episode irritability and non-episodic temper outbursts, not distinct periods of mania or hypomania. Children with DMDD do not have the classic "mood cycling" of bipolar disorder, nor do they typically experience the same degree of grandiosity, decreased need for sleep, or racing thoughts that characterize mania/hypomania. The mood is persistently negative, not episodically elevated.
- Key Differentiation from ODD: While both involve irritability and defiance, DMDD's temper outbursts are more severe, more frequent, and more pervasive, with persistent severe irritability between outbursts that is not seen in ODD.
Manifestations of Depressive Disorders and Bipolar Disorders as they present in children and adolescents.
The symptoms of mood disorders in children and adolescents are often age-dependent and can be masked by developmental stage, making them difficult to recognize. Unlike adults who might articulate feelings of sadness or euphoria, youth often express their distress through behavioral changes, irritability, or physical complaints.
Depressive disorders (Major Depressive Disorder, Persistent Depressive Disorder/Dysthymia) in youth are characterized by a pervasive low mood and/or loss of pleasure, accompanied by a range of emotional, cognitive, behavioral, and physical symptoms.
A. Emotional Manifestations:
- Irritability/Anger (Most Common in Youth): This is perhaps the most significant difference from adult depression. Instead of sadness, children and adolescents often present with persistent crankiness, short temper, rage outbursts, or an inability to tolerate minor frustrations. They might seem constantly annoyed or easily provoked.
- Persistent Sadness/Unhappiness: While often masked by irritability, children may express feelings of sadness, being down, or tearfulness. They might report feeling "empty" or "nothing matters."
- Loss of Interest or Pleasure (Anhedonia): A decrease in enjoyment from activities previously found pleasurable (e.g., hobbies, sports, playing with friends, video games). They might seem bored, withdrawn, or uninterested in anything.
- Feelings of Hopelessness/Worthlessness/Guilt: Children may express negative self-perception, feeling like a failure, blaming themselves for problems, or believing things will never get better.
- Anxiety Symptoms: Increased worry, nervousness, or fearfulness often co-occurs with depression.
B. Behavioral Manifestations:
- Social Withdrawal/Isolation: Avoiding friends, family activities, or social events. Spending more time alone in their room.
- Changes in Activity Level: Can be either psychomotor retardation (slowing down, lack of energy, lethargy) or psychomotor agitation (restlessness, inability to sit still, fidgeting).
- Academic Decline: Decreased concentration, difficulty focusing, forgetfulness, lower grades, missing assignments, or school refusal.
- Behavioral Problems/Acting Out: Increased defiance, aggression, oppositional behavior, or substance use (especially in adolescents) can sometimes be a manifestation of underlying depression.
- Increased Sensitivity/Tearfulness: Crying easily or becoming upset over minor issues.
- Self-Harm/Suicidal Behavior: Non-suicidal self-injury (e.g., cutting, burning) or suicidal ideation, threats, gestures, or attempts are serious manifestations and require immediate attention.
C. Cognitive Manifestations:
- Difficulty Concentrating/Indecisiveness: Problems paying attention in class, reading, or making simple decisions.
- Memory Problems: Forgetfulness, difficulty retaining new information.
- Negative Thinking: Pervasive pessimistic outlook, catastrophic thinking, focusing on failures.
- Preoccupation with Death/Dying: Thoughts about death, their own mortality, or wishing they weren't alive.
D. Physical (Somatic) Manifestations:
- Changes in Appetite/Weight: Can be either decreased appetite leading to weight loss (or failure to gain weight as expected) or increased appetite leading to weight gain.
- Sleep Disturbances: Insomnia (difficulty falling or staying asleep, early morning waking) or hypersomnia (sleeping excessively, difficulty waking up).
- Fatigue/Low Energy: Persistent tiredness, lack of motivation, feeling physically drained even after rest.
- Unexplained Physical Complaints: Frequent headaches, stomachaches, or other body aches without a clear medical cause.
II. Core Manifestations of Bipolar Disorders in Children and Adolescents:
Bipolar disorders involve distinct periods of elevated mood (mania or hypomania) and often periods of depression. The manifestation of mania/hypomania in youth is particularly challenging to differentiate from severe ADHD or ODD.
A. Manic/Hypomanic Episodes (Often Present as Irritability/Explosiveness in Youth):
- Severe Irritability/Explosiveness (Most Common): Instead of classic euphoria, manic episodes in children and adolescents are often characterized by persistent, severe irritability, rage, violent outbursts, and extreme defiance. This can be episodic or more continuous during an episode.
- Elevated/Expansive Mood: Less common, but can include periods of excessive cheerfulness, giddiness, silliness, or inappropriate euphoria, sometimes out of context.
- Grandiosity/Inflated Self-Esteem: Exaggerated beliefs about one's abilities, talents, or importance. May make unrealistic plans, believe they have special powers, or feel invulnerable.
- Decreased Need for Sleep: Significant reduction in sleep duration (e.g., sleeping only 2-3 hours) without feeling tired, feeling rested after very little sleep. This is a classic and highly diagnostic symptom.
- Pressured Speech/Increased Talkativeness: Talking excessively, very rapidly, loudly, or about multiple topics simultaneously, difficult to interrupt.
- Flight of Ideas/Racing Thoughts: Subjective experience that thoughts are moving too quickly, jumping from one idea to another, difficulty staying on topic.
- Distractibility: Easily sidetracked by irrelevant stimuli, difficulty focusing attention.
- Increased Goal-Directed Activity/Psychomotor Agitation: Excessive involvement in multiple activities, starting many projects but not finishing them, restlessness, fidgeting, pacing, impulsively engaging in risky behaviors.
- Reckless/Risky Behavior: Engaging in actions with high potential for negative consequences without considering the risks (e.g., sexual promiscuity, substance use, shoplifting, driving recklessly, excessive spending).
- Rapid Mood Swings: Abrupt and frequent shifts between intense emotions (e.g., from rage to giddiness to sadness). This is often referred to as "affective lability."
- Psychotic Features (Severe Cases, Bipolar I): Hallucinations (seeing/hearing things that aren't there) or delusions (false, fixed beliefs, e.g., believing they have special powers or are being targeted).
B. Depressive Episodes:
- As described above for depressive disorders. Children and adolescents with bipolar disorder will experience periods that meet criteria for Major Depressive Episodes, which can be particularly debilitating. The cycling between these states (manic/hypomanic and depressive) is characteristic.
C. Cyclothymic Disorder:
- Persistent Mood Swings: Less severe but more chronic fluctuations between mild depressive symptoms and mild hypomanic symptoms. These do not meet full criteria for major depressive or hypomanic episodes but are noticeably different from the child's typical mood.
- Irritability and Dysphoria: Often present with chronic grumpiness, discontent, and fluctuating periods of increased energy and restlessness, interspersed with periods of low mood and fatigue.
Etiology and Risk Factors Associated with Mood Disorders
Mood disorders in children and adolescents are complex, multifactorial conditions resulting from an interplay of various biological, psychological, and social factors.
No single cause explains their development; rather, a vulnerability-stress model is often applied, suggesting that individuals with certain predisposing vulnerabilities are more likely to develop a disorder when exposed to specific stressors.
I. Genetic Contributors:
Genetics play a significant role in increasing susceptibility to mood disorders.
- Family History: A strong family history of depression, bipolar disorder, or other mood disorders significantly increases a child's risk.
- Children with a parent who has Major Depressive Disorder have a 2-4 times higher risk of developing depression themselves.
- The risk for bipolar disorder is even higher; children with one parent with bipolar disorder have a 15-30% chance of developing a mood disorder (often bipolar disorder), and the risk increases to 50-75% if both parents are affected.
- Heritability: Twin and adoption studies consistently demonstrate a substantial heritable component for both depressive and bipolar disorders. However, it's important to note that specific genes are not solely responsible; rather, polygenic inheritance (multiple genes acting together) is suspected, contributing to a predisposition rather than a deterministic outcome.
II. Neurobiological Contributors:
Advances in neuroimaging and neurochemistry have identified several brain-based factors associated with mood disorders.
- Neurotransmitter Dysregulation: Imbalances or dysregulation in key neurotransmitter systems are implicated.
- Serotonin: Involved in mood regulation, sleep, appetite, and impulse control. Lower levels or dysregulation are commonly linked to depression.
- Norepinephrine: Affects alertness, energy, and attention. Dysregulation can contribute to both depressive and manic symptoms.
- Dopamine: Associated with pleasure, reward, motivation, and motor control. Implicated in both depression (low levels leading to anhedonia, low energy) and mania (excessive activity leading to euphoria, grandiosity).
- Brain Structure and Function: Differences in certain brain regions and their connectivity have been observed.
- Limbic System: (e.g., Amygdala, Hippocampus) Involved in emotion processing and memory. Dysregulation can lead to altered emotional responses.
- Prefrontal Cortex: (PFC) Involved in executive functions (planning, decision-making, impulse control, emotional regulation). Reduced activity or altered connectivity in the PFC can impair these functions, contributing to symptoms of depression and the impulsivity seen in mania.
- Neural Circuitry: Alterations in neural circuits that regulate emotion, reward, and cognition are increasingly recognized as contributing factors.
- Hormonal Imbalances: Dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis, which controls the stress response, is often seen in mood disorders. Elevated cortisol levels can impact brain function and lead to depressive symptoms. Pubertal hormonal changes may also play a role, particularly in adolescent-onset mood disorders.
III. Psychosocial Contributors:
These factors relate to an individual's psychological makeup and their interactions within social environments.
- Temperament and Personality Traits:
- Negative Affectivity: A predisposition to experience negative emotions (anxiety, sadness, irritability).
- Behavioral Inhibition: A tendency to be shy, withdrawn, and fearful in novel situations.
- Neuroticism: A personality trait characterized by emotional instability, anxiety, and worry.
- Perfectionism: Can lead to excessive self-criticism and feelings of inadequacy.
- Cognitive Distortions: Maladaptive thought patterns, such as negative self-talk, catastrophic thinking, hopelessness, and learned helplessness, can perpetuate or exacerbate depressive symptoms.
- Poor Coping Skills: Inadequate strategies for managing stress, emotions, and challenges can increase vulnerability.
- Low Self-Esteem: A pervasive negative self-view can contribute to and be maintained by depressive episodes.
IV. Environmental Contributors (Stressors):
Exposure to adverse environmental experiences and stressors can precipitate mood disorders, especially in genetically vulnerable individuals.
- Adverse Childhood Experiences (ACEs):
- Trauma: Physical, emotional, or sexual abuse.
- Neglect: Physical or emotional neglect.
- Household Dysfunction: Exposure to domestic violence, parental substance abuse, parental mental illness, parental separation/divorce, or incarceration of a household member.
- High ACE scores are strongly linked to an increased risk of mood disorders.
- Family Environment:
- Parental Psychopathology: Parents with mental health disorders, especially mood disorders, can create a less supportive or more chaotic home environment.
- Parent-Child Conflict: High levels of conflict, lack of warmth, or critical parenting styles.
- Family Instability: Frequent moves, financial difficulties, or disruptions in family structure.
- Poor Attachment: Insecure attachment patterns with primary caregivers.
- Peer Relationships:
- Bullying/Victimization: Being subjected to physical, verbal, or social aggression by peers.
- Social Isolation/Rejection: Feeling lonely or excluded by peers.
- Peer Pressure: Pressure to engage in risky behaviors, especially when coupled with low self-esteem.
- Academic Stress: High academic demands, school-related failures, or learning difficulties.
- Life Stressors: Significant life changes (moving, changing schools), loss of a loved one, chronic illness (personal or family member), relationship breakups (in adolescence).
- Substance Use: As discussed in Objective 1, substance abuse can induce or exacerbate mood symptoms. Self-medication with substances is also common in youth struggling with underlying mood disorders.
Diagnostic Process for Mood Disorders in Children and Adolescents
There is no single "test" for mood disorders; instead, diagnosis relies on a comprehensive clinical assessment.
- Multimodal/Multi-informant Assessment: Information should be gathered from various sources:
- Child/Adolescent Interview: Direct assessment of symptoms, feelings, thoughts, and perception of functioning. Rapport building is key.
- Parent/Caregiver Interview: Crucial for developmental history, family history, home behavior, onset/duration of symptoms, and impact on family life.
- Teacher/School Reports: Essential for understanding behavior, mood, and academic functioning in the school setting, often providing objective observations.
- Other Relevant Informants: (e.g., coaches, therapists, previous providers) if applicable and with consent.
- Developmental Sensitivity: Symptoms must be evaluated in the context of the child's age and developmental stage. What is problematic for a 15-year-old might be normal for a 5-year-old.
- Longitudinal Perspective: Mood disorders are not static. Symptoms often fluctuate, and a comprehensive history helps understand the course of the illness, including onset, duration, severity, and previous episodes.
- Emphasis on Functional Impairment: Symptoms must cause clinically significant distress or impairment in social, academic, occupational, or other important areas of functioning.
- Rule-Out Approach (Differential Diagnosis): Before concluding a mood disorder, other conditions that could mimic or explain the symptoms must be systematically considered and ruled out.
Components of the Diagnostic Assessment:
A. Detailed History Taking:
- Presenting Problem: Detailed description of current symptoms, including onset, frequency, intensity, duration, triggers, and what makes them better or worse.
- Developmental History: Pregnancy and birth complications, developmental milestones, temperament, early childhood experiences, significant traumas.
- Psychiatric History: Previous episodes of mood disturbance, psychiatric diagnoses, hospitalizations, previous treatments (medications, therapy), response to treatment, self-harm or suicide attempts.
- Family Psychiatric History: History of mood disorders, anxiety disorders, substance use, suicide in first-degree relatives. This helps assess genetic risk.
- Medical History: Past and current medical illnesses, hospitalizations, surgeries, current medications (prescription, OTC, supplements), allergies. Rule out medical conditions that could cause mood symptoms.
- Substance Use History: For adolescents, inquire about alcohol, tobacco, illicit drug use, and prescription medication misuse.
- Social History: Peer relationships, bullying, social skills.
- Academic History: School performance, learning difficulties, disciplinary issues, school attendance, relationships with teachers.
- Trauma History: Exposure to abuse (physical, emotional, sexual), neglect, domestic violence, significant losses, natural disasters.
- Cultural and Spiritual Factors: Understanding the family's cultural background, beliefs about mental illness, and spiritual practices can influence how symptoms are expressed and perceived.
B. Mental Status Examination (MSE):
- Appearance: Grooming, hygiene, age appropriateness.
- Behavior: Psychomotor activity (agitation, retardation), eye contact, tics, mannerisms.
- Speech: Rate, rhythm, volume, clarity, spontaneity.
- Mood: Subjective report of emotional state (e.g., "sad," "angry," "upbeat").
- Affect: Objective observation of emotional expression (e.g., "flat," "constricted," "labile," "irritable," "appropriate to mood").
- Thought Process: Organization, logic, coherence (e.g., "linear," "flight of ideas," "loose associations").
- Thought Content: Presence of delusions, obsessions, suicidal/homicidal ideation, paranoia. Crucially, assess for suicidal ideation, intent, plan, and access to means.
- Perceptual Disturbances: Hallucinations (auditory, visual, etc.).
- Cognition: Orientation, attention, concentration, memory, general knowledge.
- Insight: Understanding of their condition.
- Judgment: Ability to make sound decisions.
C. Use of Standardized Rating Scales and Screening Tools:
- Depression Scales: Children's Depression Inventory (CDI), Beck Depression Inventory (BDI), PHQ-9 (modified for adolescents), Center for Epidemiologic Studies Depression Scale for Children (CES-DC).
- Mania/Bipolar Scales: Mood Disorder Questionnaire (MDQ), Child Mania Rating Scale (CMRS), Young Mania Rating Scale (YMRS).
- General Symptom Checklists: Child Behavior Checklist (CBCL), Strengths and Difficulties Questionnaire (SDQ).
- Suicide Risk Scales: Columbia-Suicide Severity Rating Scale (C-SSRS).
D. Physical Examination and Laboratory Tests:
- Complete Blood Count (CBC).
- Thyroid Function Tests (TFTs) to rule out hypo/hyperthyroidism.
- Electrolyte Panel.
- Vitamin D and B12 levels.
- Urine toxicology screen (especially for adolescents) to rule out substance-induced mood symptoms.
- Other tests as indicated by clinical presentation (e.g., EEG for seizure disorders, neuroimaging if neurological concerns).
Differential Diagnosis
This is the process of distinguishing a particular disease or condition from others that present with similar symptoms. For mood disorders in youth, this often involves differentiating from:
- Normal Developmental Fluctuations: Mood swings and irritability are common during adolescence. The key is the intensity, persistence, and impact on functioning.
- Anxiety Disorders: Can co-occur, but primary anxiety disorders might present with irritability, poor sleep, and concentration difficulties.
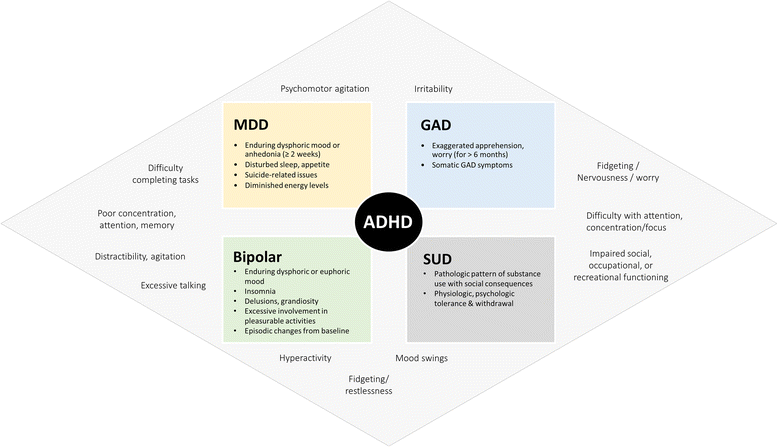
- Attention-Deficit/Hyperactivity Disorder (ADHD): Hyperactivity, impulsivity, and inattention can mimic manic/hypomanic symptoms, especially irritability and distractibility. Differentiation often lies in the episodic nature of bipolar symptoms versus the chronic presentation of ADHD.
- Oppositional Defiant Disorder (ODD)/Conduct Disorder (CD): Chronic irritability, defiance, and behavioral outbursts can resemble DMDD or symptoms within a depressive or manic episode.
- Substance Use Disorders: Can cause or exacerbate mood symptoms. A comprehensive toxicology screen and history are essential.
- Psychotic Disorders: Early stages of schizophrenia or other psychotic disorders can sometimes present with mood symptoms, especially with disorganized thought processes.
- Trauma-Related Disorders (PTSD, Adjustment Disorders): Symptoms of depression or anxiety can arise in response to traumatic events.
- Medical Conditions: As discussed in Objective 1 (e.g., thyroid disease, neurological conditions, anemia, chronic pain).
- Medication Side Effects: Some medications (e.g., corticosteroids, anticonvulsants) can induce mood symptoms.
Nursing Diagnoses for Children and Adolescents
- Risk for Suicide
- Related Factors: Depressed mood, feelings of hopelessness/worthlessness, previous suicide attempts, family history of suicide, access to means, substance abuse, chronic illness, social isolation, impulsive behavior (especially in adolescents).
- Defining Characteristics: (Not directly observed, as it's a risk diagnosis, but inferred from risk factors and verbal/behavioral cues) Verbalization of suicidal ideation, making plans, giving away possessions, sudden improvement in mood after prolonged depression, self-harm gestures.
- Priority: This is often the highest priority nursing diagnosis in depression.
- Hopelessness
- Related Factors: Chronic pain or illness, long-term stress, deteriorating physical condition, perceived loss of control, social isolation, feelings of worthlessness, lack of support system.
- Defining Characteristics: Verbal cues (e.g., "I give up," "What's the use?"), decreased affect, lack of initiative, passivity, sleep disturbance, decreased appetite, withdrawal, decreased problem-solving ability.
- Low Self-Esteem (Situational or Chronic)
- Related Factors: Lack of positive feedback, perceived failure (academic, social), dysfunctional family dynamics, negative self-talk, body image disturbance, social isolation, peer rejection/bullying.
- Defining Characteristics: Self-negating verbalizations (e.g., "I'm stupid," "I can't do anything right"), expressions of shame/guilt, social withdrawal, lack of eye contact, indecisiveness, excessive need for reassurance, aggressive behavior (as a compensatory mechanism).
- Social Isolation
- Related Factors: Depression, anxiety, perceived rejection, immature interests, developmental delay, inadequate social skills, withdrawal behaviors, family conflict.
- Defining Characteristics: Absence of supportive significant others, expressions of loneliness, withdrawal from social activities, preoccupation with own thoughts, sad/dull affect.
- Inadequate protein energy nutritional intake
- Related Factors: Depressed mood, loss of appetite, anhedonia, poor oral intake, inadequate knowledge of nutritional needs.
- Defining Characteristics: Weight loss (or failure to gain weight appropriate for age), aversion to eating, poor muscle tone, pale conjunctiva and mucous membranes, verbal report of inadequate food intake.
- Disrupted Sleep Pattern
- Related Factors: Psychological stress, internalizing behaviors (anxiety, depression), worry, environmental disturbances, medication side effects.
- Defining Characteristics: Verbal complaints of difficulty falling asleep, frequent awakenings, early morning awakening, not feeling rested, changes in mood/irritability, lethargy, dark circles under eyes.
- Ineffective Coping
- Related Factors: Inadequate coping skills, emotional distress, poor impulse control, trauma history, low self-esteem, lack of problem-solving skills, unsupportive environment.
- Defining Characteristics: Verbalization of inability to cope, inability to meet basic needs, destructive behavior towards self or others, use of maladaptive coping mechanisms (e.g., substance abuse, self-harm), changes in usual behavior patterns.
- Risk for Delayed Development (especially for younger children with chronic, severe depression)
- Related Factors: Chronic illness, poor social interaction, lack of environmental stimulation, impaired primary caregiver, physical/emotional neglect.
- Defining Characteristics: (Inferred from risk factors) Regression in developmental milestones, difficulty learning new skills, apathy, lack of initiative.
- Risk for Injury
- Related Factors: Extreme psychomotor agitation, poor judgment, impulsivity, grandiosity, decreased need for sleep, aggressive behavior, engagement in risky activities, environmental hazards.
- Defining Characteristics: (Inferred from risk factors) Restlessness, hyperactivity, inability to control impulses, engaging in high-risk behaviors without regard for consequences, self-neglect.
- Priority: Often the highest priority during acute manic phases.
Specific Nursing Interventions for Children and Adolescents with Mood Disorders
Nursing interventions for children and adolescents aiming to promote safety, stabilize mood, improve functioning, enhance coping skills, and support overall well-being.
Principles Guiding Nursing Interventions:
- Safety First: Prioritize interventions that address immediate risks, especially suicide, self-harm, and aggression.
- Therapeutic Relationship: Establish a trusting, empathetic, and non-judgmental relationship with the child/adolescent and their family.
- Individualized Care: Tailor interventions to the specific needs, developmental stage, and cultural background of the child/adolescent and family.
- Family-Centered Care: Involve parents/caregivers as active partners in the treatment plan, providing education and support.
- Interdisciplinary Collaboration: Work closely with psychiatrists, psychologists, social workers, teachers, and other healthcare professionals.
- Psychoeducation: Provide comprehensive information about the disorder, treatment options, symptom management, and relapse prevention.
- Skill Building: Help the child/adolescent develop coping mechanisms, problem-solving skills, emotional regulation strategies, and social skills.
- Least Restrictive Environment: Strive to provide care in the least restrictive setting possible while ensuring safety and effectiveness.
Nursing Interventions Across Settings:
A. Inpatient Setting (Acute Stabilization, High-Risk Situations):
- Suicide/Self-Harm Precautions: Implement constant observation (1:1 sitter) or frequent checks, remove all dangerous objects (sharps, ligatures), ensure tamper-proof environment.
- Aggression Management: Monitor for escalation, use de-escalation techniques, implement least restrictive restraints (verbal, chemical, physical) as per policy and only when absolutely necessary, followed by debriefing.
- Administration & Monitoring: Administer prescribed psychotropic medications (antidepressants, mood stabilizers, antipsychotics) accurately.
- Side Effect Monitoring: Closely observe and document side effects (e.g., akathisia, sedation, weight changes, suicidal ideation with SSRIs in some youth). Educate about side effects.
- Therapeutic Efficacy: Monitor for therapeutic effects and report to the prescriber.
- Routine and Predictability: Establish consistent daily schedules for activities, meals, and sleep to provide a sense of security and structure.
- Limit Setting: Consistently enforce clear, fair, and firm boundaries to manage behavior and provide a sense of control and safety.
- Active Listening & Validation: Listen to concerns, validate feelings, even if behavior is maladaptive.
- Individual & Group Therapy Participation: Encourage and facilitate participation in therapeutic activities (e.g., CBT, DBT, art therapy).
- Psychoeducation: Begin educating the patient and family about the diagnosis, medication, and coping skills.
- ADLs Assistance: Assist with activities of daily living (hygiene, grooming) if self-care deficits are present.
- Nutrition & Hydration: Monitor intake, offer nutritional supplements if needed, encourage regular meals.
- Sleep Promotion: Implement sleep hygiene practices (quiet environment, consistent bedtime, no electronics).
B. Outpatient Setting (Ongoing Management, Prevention, Skill Building):
- Adherence Education: Educate child/adolescent and family about medication purpose, dosage, administration, importance of adherence, and potential side effects.
- Side Effect Monitoring: Assess for and manage side effects in collaboration with the prescriber.
- Relapse Prevention: Emphasize the importance of continued medication use even when feeling better.
- Disease Education: Explain the specific mood disorder, its etiology, symptoms, and prognosis.
- Coping Strategies: Teach stress management, relaxation techniques (deep breathing, progressive muscle relaxation), problem-solving skills, and emotional regulation.
- Communication Skills: Improve assertive communication and conflict resolution.
- Relapse Recognition & Prevention: Help identify early warning signs of worsening mood and develop an action plan.
- Referrals: Facilitate referrals to individual, family, and group therapy (e.g., CBT, DBT, interpersonal therapy).
- Support Groups: Suggest age-appropriate peer support groups.
- Nutrition & Exercise: Promote a balanced diet and regular physical activity.
- Sleep Hygiene: Reinforce healthy sleep habits.
- Stress Reduction: Encourage hobbies, mindfulness, and healthy leisure activities.
- Symptom Tracking: Use symptom rating scales to monitor progress and adjust treatment.
- Safety Planning: Review and update safety plans (for suicide/self-harm risk).
- Appointment Adherence: Encourage attendance at all appointments.
C. School Setting (Support, Integration, Early Identification):
- IEP/504 Plans: Advocate for and participate in the development and implementation of individualized education plans (IEPs) or 504 plans to accommodate academic needs (e.g., reduced workload, extended time, preferential seating, quiet testing environment).
- Communication: Liaison between family, healthcare team, and school staff to ensure consistent support.
- Behavioral Plans: Help develop and implement classroom management strategies tailored to the student's needs.
- Social Skills Training: Facilitate opportunities for social skill development and positive peer interactions.
- Tutoring/Extra Help: Suggest academic accommodations or support services.
- Monitoring Attendance & Performance: Track school attendance and academic progress, noting changes that may indicate worsening symptoms.
- Emergency Protocols: Ensure school staff are aware of emergency protocols for mental health crises, including suicide risk.
- Referrals: Assist with referrals to school counselors or external mental health services.
- Staff Education: Educate teachers and school personnel on recognizing signs of mood disorders and appropriate responses.
- Peer Education: Promote anti-stigma initiatives and understanding among peers (age-appropriate).
D. Community Setting (Prevention, Advocacy, Resource Connection):
- Connecting Families to Resources: Provide information and referrals to community mental health services, support groups, advocacy organizations, and financial assistance programs.
- Advocacy: Advocate for policies that support mental health services for youth.
- Awareness Campaigns: Participate in or initiate community-wide campaigns to reduce stigma and increase awareness of mental health issues in youth.
- Early Identification: Educate community groups (e.g., youth sports coaches, scout leaders) on recognizing early signs of mood disorders.
- Emergency Planning: Inform families about local crisis hotlines, walk-in clinics, and emergency services.
- Youth Programs: Support and encourage participation in positive youth development programs that foster resilience, self-esteem, and social connections.
Evaluation of the Effectiveness of Nursing Interventions and Treatment Plan.
Evaluation is an ongoing and systematic process that determines the effectiveness of nursing interventions and the overall treatment plan.
I. Principles of Evaluation:
- Continuous Process: Evaluation is not a one-time event but an ongoing cycle that occurs throughout the entire care trajectory, from initial assessment to discharge and follow-up.
- Client-Centered: Outcomes should reflect improvements that are meaningful to the child/adolescent and their family.
- Objective and Subjective Data: Utilize both measurable data (e.g., symptom scores, school attendance) and the client's/family's subjective reports of well-being.
- Multimodal Approach: Gather evaluative data from multiple sources (child/adolescent, parents, teachers, other providers).
- Interdisciplinary Collaboration: Share evaluation findings and collaborate with the entire treatment team to make informed decisions.
- Documentation: Clearly document all evaluation findings, adjustments to the care plan, and the rationale behind those changes.
II. Key Areas for Evaluation:
A. Symptom Severity and Frequency:
- Tools: Re-administer standardized rating scales (e.g., PHQ-9, CDI for depression; CMRS, YMRS for mania) at regular intervals to track changes in symptom severity.
- Observation: Nurses' ongoing observation of behaviors, mood, and affect for improvement or worsening.
- Self-Report/Parent Report: Ask the child/adolescent and parents to rate symptom severity (e.g., on a 0-10 scale) and note any changes.
- Specific Symptoms: Monitor specific target symptoms identified during assessment (e.g., frequency of rage outbursts, duration of sleep, presence of anhedonia, suicidal ideation).
B. Functional Impairment:
- Academic Performance: Monitor grades, school attendance, completion of homework, participation in class, and reports from teachers.
- Social Functioning: Observe and inquire about peer interactions, participation in extracurricular activities, social withdrawal, and family relationships.
- Activities of Daily Living (ADLs): Assess for improvements in self-care, hygiene, and age-appropriate responsibilities.
- Behavioral Regulation: Note changes in impulsivity, aggression, defiance, and overall behavioral control.
C. Safety:
- Suicide Risk: Continuously assess for suicidal ideation, intent, plan, and behaviors. Any increase in risk necessitates immediate intervention and care plan adjustment.
- Self-Harm: Monitor for cessation or reduction of non-suicidal self-injury, and the use of healthy coping strategies instead.
- Aggression/Violence: Track the frequency and intensity of aggressive outbursts and the effectiveness of de-escalation strategies.
D. Medication Adherence and Side Effects:
- Adherence: Ask the child/adolescent and parents about consistent medication taking.
- Side Effects: Routinely assess for the presence and severity of medication side effects.
- Therapeutic Efficacy: Determine if the medication is achieving its intended therapeutic effect on mood and behavior.
E. Coping Skills and Resilience:
- Observed Use: Note whether the child/adolescent is actively using taught coping strategies (e.g., relaxation techniques, problem-solving, communication skills) in stressful situations.
- Self-Report: Ask the child/adolescent about their perceived ability to cope with challenges.
- Stress Management: Assess their ability to manage daily stressors without significant decompensation.
F. Family Functioning and Support:
- Family Communication: Observe and inquire about improvements in family communication patterns.
- Parental Coping: Assess parents' ability to cope with the child's illness and their engagement in the treatment plan.
- Support System: Evaluate the adequacy of the family's formal and informal support systems.
G. Client and Family Satisfaction:
- Feedback: Obtain feedback from the child/adolescent and family regarding their satisfaction with the care received, their perception of progress, and any unmet needs.
III. Adjusting the Care Plan:
Based on the evaluation findings, the nursing care plan, and the broader treatment plan, will be adjusted as follows:
- If Goals Are Met:
- Reinforce Success: Acknowledge and celebrate the child/adolescent's progress and efforts.
- Set New Goals: Establish new, more advanced goals to continue progress, focusing on relapse prevention and further skill development.
- Transition Care: Consider stepping down to a less intensive level of care if appropriate and safe.
- Discharge Planning: Prepare for discharge, ensuring adequate follow-up and community resources.
- If Goals Are Partially Met or Not Met:
- Reassessment: Conduct a thorough reassessment to identify new or persistent problems, changes in circumstances, or barriers to progress.
- Review Diagnoses: Re-evaluate the accuracy and relevance of existing nursing diagnoses.
- Modify Interventions: Adjust nursing interventions. This might involve:
- Increasing the intensity or frequency of an intervention.
- Introducing new interventions.
- Modifying the approach (e.g., trying a different teaching method).
- Addressing previously overlooked barriers.
- Collaborate with Team: Discuss findings with the interdisciplinary team to consider changes in medication, therapy type, or other aspects of the overall treatment plan.
- Family Engagement: Re-engage the family to ensure their understanding and participation in any revised plan.
- Problem-Solve Barriers: Identify and problem-solve any identified barriers to treatment (e.g., transportation issues, financial constraints, lack of motivation).
- Emergence of New Problems/Risks:
- Immediate Action: Address any new safety concerns (e.g., increased suicidal ideation) or significant symptom worsening with immediate, appropriate interventions.
- Re-prioritize: Adjust priorities in the care plan to reflect the most pressing needs.
- Escalate Care: Consider a higher level of care (e.g., inpatient hospitalization) if the current setting cannot adequately manage the new risks or symptoms.
Mood Disorders in Children and Adolescents Read More »