
Table of Contents
ToggleDwarfism (Panhypopituitarism)
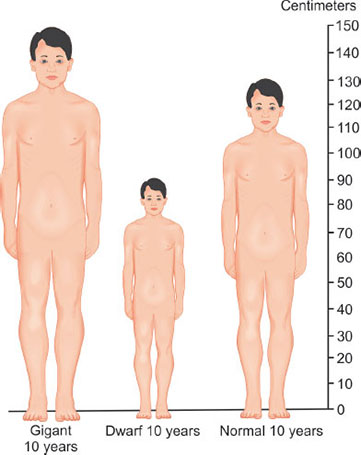
Dwarfism is a medical condition characterized by short stature.
It is defined as an adult height of 4 feet 10 inches (147 centimeters) or shorter. There are different types of dwarfism, which can be caused by various underlying factors.
It is a condition characterized by the underproduction or deficiency of several hormones produced by the pituitary gland. The primary hormones affected in panhypopituitarism include:
- Growth hormone (GH): GH plays a key role in stimulating growth and development in children. Its deficiency can result in impaired growth and short stature.
- Thyroid-stimulating hormone (TSH): TSH regulates the function of the thyroid gland, which affects metabolism, energy levels, and growth. Deficiency of TSH can lead to thyroid hormone deficiency.
- Adrenocorticotropic hormone (ACTH): ACTH stimulates the production of cortisol by the adrenal glands. Its deficiency can result in adrenal insufficiency.
- Gonadotropins (Luteinizing hormone [LH] and Follicle-stimulating hormone [FSH]): These hormones regulate the function of the gonads (testes in males, ovaries in females) and play a crucial role in reproductive function. Deficiency of gonadotropins can lead to infertility and sexual dysfunction.
- Prolactin: Prolactin is involved in milk production in females. Its deficiency may result in decreased lactation in breastfeeding women.
Types of Dwarfism
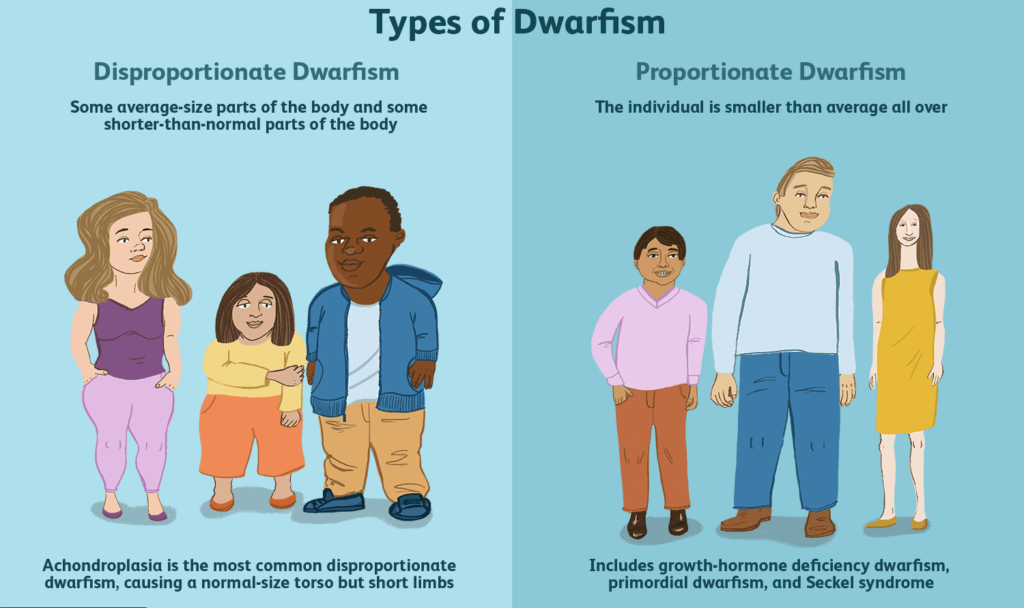
There are two main types of dwarfism — disproportionate and proportionate.
Disproportionate dwarfism: Disproportionate dwarfism is characterized by an average-size torso and shorter arms and legs or a shortened trunk with longer limbs. The most common types of dwarfism, known as skeletal dysplasia’s, are genetic. Skeletal dysplasia’s are conditions of abnormal bone growth that cause disproportionate dwarfism.
Skeletal dysplasia’s include:
1. Achondroplasia: The most common cause of dwarfism which causes disproportionately short stature. This is the most common form of dwarfism, occurs in about one out of 26,000 to 40,000 babies and is evident at birth. People with achondroplasia have a relatively long trunk and shortened upper parts of their arms and legs.
- This disorder usually results in the following:
- An average-size trunk
- Short arms and legs, with particularly short upper arms and upper legs
- Short fingers, often with a wide separation between the middle and ring fingers
- Limited mobility at the elbows
- An adult height around 4 feet (122 cm)
- a large head with a prominent forehead and a flattened bridge of the nose
- protruding jaw
- crowded and misaligned teeth
- forward curvature of the lower spine
- Progressive development of bowed legs
2. Spondyloepiphyseal dysplasia Congenita (SEDC): Another rare cause of disproportionate dwarfism that affects approximately one in 95,000 babies. It refers to a group of conditions characterized by a shortened trunk, which may not become apparent until a child is between ages 5 and 10.
- A very short trunk
- A short neck
- Shortened arms and legs
- Average-size hands and feet
- Slightly flattened cheekbones
- Hip deformities that result in thighbones turning inward
- Instability of the neck bones.
- Progressive hunching curvature of the upper spine.
- Progressive development of swayed lower back
- Vision and hearing problems.
- Arthritis and problems with joint movement.
- Adult height ranging from 3 feet (91 cm) to just over 4 feet (122 cm).
- club feet (A foot that’s twisted or out of shape).
- Opening in the roof of the mouth (cleft palate).
- severe osteoarthritis in the hips
- weak hands and feet.
- barrel-chested appearance (Broad, rounded chest)
3. Diastrophic dysplasia: A rare form of dwarfism, diastrophic dysplasia occurs in about one in 100,000 births. People who have it tend to have shortened forearms and calves (calf muscles-this is known as mesomelic shortening).

Achondroplasia

Spondyoepipheseal

Diastrophic
Proportionate dwarfism: In Proportionate dwarfism, the body parts are in proportion but shortened. It usually results from medical conditions present at birth or appearing in early childhood that limit overall growth and development. So the head, trunk and limbs are all small, but they’re proportionate to each other. Because these disorders affect overall growth, many of them result in poor development of one or more body systems. Growth hormone deficiency is a relatively common cause of proportionate dwarfism. It occurs when the pituitary gland fails to produce an adequate supply of growth hormone, which is essential for normal childhood growth.
Signs include:
- Height below the third percentile on standard pediatric growth charts
- Growth rate slower than expected for age
- Delayed or no sexual development during the teen years.

Causes of Dwarfism
- Most dwarfism-related conditions are genetic disorders, but the causes of some disorders are unknown. Most occurrences of dwarfism result from a random genetic mutation in either the father’s sperm or the mother’s Ovum rather than from either parent’s complete genetic makeup.
- Dwarfism can be caused by any of more than 200 conditions. Causes of proportionate dwarfism include metabolic and hormonal disorders such as growth hormone deficiency.
- The most common types of dwarfism, known as skeletal dysplasias, are genetic. Skeletal dysplasias are conditions of abnormal bone growth that cause disproportionate dwarfism.
Other causes include;
- Deficiency of growth hormone
- Malnutrition
- Inherited defect i.e. turners syndrome(Turner syndrome, a condition that affects only girls and women, results when a sex chromosome (the X chromosome) is missing or partially missing. A female inherits an X chromosome from each parent. A girl with Turner syndrome has only one fully functioning copy of the female sex chromosome rather than two)
- Renal disorders
- Congenital heart disease
- Chronic infection in childhood
Diagnosis of Dwarfism
- Some forms of dwarfism are evident at birth or during infancy and can be diagnosed through X-rays and a physical exam.
- A diagnosis of achondroplasia, diastrophic dysplasia, or spondyloepiphyseal dysplasia can be confirmed through genetic testing. In some cases, prenatal testing is done if there is concern for specific conditions.
- Sometimes dwarfism doesn’t become evident until later in a child’s life, when dwarfism signs lead parents to seek a diagnosis. Here are signs and symptoms to look for in children that indicate a potential for dwarfism:
- Late development of certain motor skills, such as sitting up or walking.
- Breathing problems
- Curvature of the spine
- bowed legs
- Joint stiffness and arthritis
- Lower back pain or numbness in the legs
- Crowding of teeth.
- Measurements. A regular part of a well-baby medical exam is the measurement of height, weight and head circumference. At each visit, they will be plotted on a chart to show the child’s current percentile ranking for each one. This is important for identifying abnormal growth, such as delayed growth or a disproportionately large head. If any trends in these charts are a concern, the health worker may make more-frequent measurements.
- Appearance. A child’s appearance may also help to make a diagnosis. Many distinct facial and skeletal features are associated with each of several dwarfism disorders.
- Imaging technology. Imaging studies, such as X-rays, may be ordered because certain abnormalities of the skull and skeleton can indicate which disorder a child may have. Various imaging devices may also reveal delayed maturation of bones, as is the case in growth hormone deficiency.
- A magnetic resonance imaging (MRI) scan may reveal abnormalities of the pituitary gland or hypothalamus, both of which play a role in hormone function.
- Genetic tests. Genetic tests are available for many of the known causal genes of dwarfism-related disorders, but these tests often aren’t necessary to make an accurate diagnosis. If the pediatrician believes the daughter may have Turner syndrome, then a special lab test may be done that assesses the X chromosomes extracted from blood cells.
- Family history. The pediatrician may take a history of stature in siblings, parents, grandparents or other relatives to help determine whether the average range of height in the family includes short stature.
- Hormone tests. Tests that assess levels of growth hormone or other hormones that are critical for childhood growth and development may be ordered.
Management of Dwarfism
Treatment for Underlying Cause: Focus on addressing the specific cause of dwarfism, if possible.
Growth Hormone Therapy: GH injections can be administered to stimulate growth in children and adolescents.
Physical Therapy:
- Improve Mobility: Develop strategies to compensate for mobility limitations.
- Strengthen Muscles: Improve overall strength and endurance.
Psychological Support:
- Counseling: Address any emotional issues related to self-esteem, body image, and social integration.
- Support Groups: Connect with others who have dwarfism to share experiences and build support networks.
Nursing Care:
Education and Support:
- Provide comprehensive information about dwarfism, its causes, and treatment options.
- Encourage open communication and emotional support for the individual and their family.
Medication Administration:
- Administer GH injections accurately and monitor for side effects.
- Educate patients and families about proper injection techniques and storage.
Physical Care:
- Assess mobility, and provide assistive devices and adaptive techniques as needed.
- Promote healthy weight management and encourage regular exercise.
Emotional Support:
- Empathize with the challenges of living with dwarfism and provide emotional support.
- Facilitate access to counseling and support groups for the individual and their family.
Advocacy:
- Advocate for the individual’s needs and rights.
- Connect them with resources and support services for people with dwarfism.
Nursing Concerns:
- Growth Hormone Therapy: Monitor for side effects of GH treatment, such as fluid retention, joint pain, and increased risk of diabetes.
- Mobility and Safety: Assess for potential falls and injuries related to mobility limitations. Provide modifications and adaptations to improve safety in the home and community.
- Psychological Well-being: Monitor for signs of depression, anxiety, and social isolation. Promote self-esteem and body image through counseling and support groups.
- Accessibility: Advocate for accessible environments and accommodations for individuals with dwarfism.
- Long-Term Management: Educate individuals and families about the lifelong implications of dwarfism and the need for ongoing care and support.
Surgical Management
- Surgical procedures that may correct problems in people with disproportionate dwarfism include:
- Correcting the direction in which bones are growing
- Stabilizing and correcting the shape of the spine
- Increasing the size of the opening in bones of the spine (vertebrae) to alleviate pressure on the spinal cord
- Placing a shunt to remove excess fluid around the brain (hydrocephalus), if it occurs to drain excess fluid and relieve pressure on the brain.
Limb lengthening
- Some people with dwarfism choose to undergo surgery called extended limb lengthening. This procedure is controversial for many people with dwarfism because, as with all surgeries, there are risks.
- Because of the emotional and physical stress of multiple procedures, waiting until the person with dwarfism is old enough to participate in the decision to have the surgery is recommended.
Ongoing health care
- Regular checkups and ongoing care by a doctor familiar with dwarfism can improve quality of life.
- Because of the range of symptoms and complications, treatments are tailored to address problems as they occur, such as assessment and treatment for ear infections, spinal stenosis or sleep apnea.
- Adults with dwarfism should continue to be monitored and treated for problems that occur throughout life.
In many cases, people with dwarfism have orthopaedic or medical complications. Treatment of those can include:
- A tracheotomy to improve breathing through small airways.
- Corrective surgeries for deformities such as cleft palate, club foot, or bowed legs
- Surgery to remove tonsils or adenoids to improve breathing problems related to large tonsils, small facial structures, and/or a small chest.
- Surgery to widen the spinal canal to relieve spinal cord compression.
Other treatments may include:
- Physical therapy to strengthen muscles and increase joint range of motion.
- Back braces to improve curvature of the spine
- Placement of draining tubes in the middle ear to help prevent hearing loss due to repeated ear infections.
- Orthodontic treatment to relieve crowding of teeth caused by a small jaw.
- Nutritional guidance and exercise to help prevent obesity, which can aggravate skeletal problems.
Life style and home remedies
- Talk with the pediatrician or a specialist about home care. Issues particularly critical for children with disproportionate dwarfism include:
- Car seats. Use an infant car seat with firm back and neck supports. Continue using a car seat in the rear-facing direction to the highest weight and height possible (and beyond the recommended age limit).
- Infant carriers and play equipment. Avoid infant devices such as swings, umbrella strollers, carrying slings, jumper seats and backpack carriers that don’t support the neck or that curve the back into a C shape.
- Adequate support. Support the child’s head and neck when he or she is seated.
- Complications. Monitor the child for signs of complications, such as ear infection or sleep apnea.
- Posture. Promote good posture by providing a pillow for the lower back and a footstool when the child is sitting.
- Healthy diet. Begin healthy eating habits early to avoid later problems with weight gain.
- Healthy activities. Encourage participation in appropriate recreational activities, such as swimming or bicycling, but avoid sports that involve collision or impact, such as football, diving or gymnastics.
- Coping and support. If a child has dwarfism, a number of steps to help him or her cope with challenges and function independently:
- Seek help. Organizations provides social support, information about disorders, advocacy opportunities and resources. Many people with dwarfism stay actively involved in this organization throughout their lives.
- Modify the home. Make changes in the home, such as putting specially designed extensions on light switches, installing lower handrails in stairways and replacing doorknobs with levers.
- Provide personal adaptive tools. Everyday activities and self-care can be a problem with limited arm reach and problems with dexterity. An occupational therapist also may be able to recommend appropriate tools for home and school use.
- Talk to educators. Talk to school personnel about what dwarfism is, how it affects the child, what needs the child may have in the classroom and how the school can help meet those needs.
- Talk about teasing. Encourage the child to talk to you about his or her feelings, and practice responses to insensitive questions and teasing.
- If the child tells you that bullying occurs in school, seek help from the child’s teacher, principal or the school guidance counselor and ask for a copy of the school’s policy on bullying.
Complications of Dwarfism
Complications of dwarfism-related disorders can vary greatly, but some complications are common to a number of conditions.
Disproportionate dwarfism
- The characteristic features of the skull, spine and limbs shared by most forms of disproportionate dwarfism result in some common problems.
- Delays in motor skills development, such as sitting up, crawling and walking.
- Frequent ear infections and risk of hearing loss.
- Bowing of the legs.
- Difficulty breathing during sleep (sleep apnea).
- Pressure on the spinal cord at the base of the skull.
- Excess fluid around the brain (hydrocephalus).
- Crowded teeth
- Progressive severe hunching or swaying of the back with back pain or problems breathing
- Narrowing of the channel in the lower spine (spinal stenosis), resulting in pressure on the spinal cord and subsequent pain or numbness in the legs
- Arthritis
- Weight gain that can further complicate problems with joints and the spine and place pressure on nerves
Proportionate dwarfism
- With proportionate dwarfism, problems in growth and development often result in complications with poorly developed organs. For example, heart problems often present in Turner syndrome can have a significant effect on health.
- An absence of sexual maturation associated with growth hormone deficiency
- Turner syndrome affects both physical development and social functioning.
- Pregnancy: Women with disproportionate dwarfism may develop respiratory problems during pregnancy. A C-section (cesarean delivery) is almost always necessary because the size and shape of the pelvis doesn’t allow for successful vaginal delivery.
- Public perceptions
- Most people with dwarfism prefer not to be labeled by a condition. However, some people may refer to themselves as dwarfs or little people.
- People of average height may have misconceptions about people with dwarfism. And the portrayal of people with dwarfism in modern movies often includes stereotypes.
- Misconceptions can impact a person’s self-esteem and limit opportunities for success in school or employment.
- Children with dwarfism are particularly vulnerable to teasing and ridicule from classmates. Because dwarfism is relatively uncommon, children may feel isolated from their peers.
Quick Quiz
Dwarfism Quiz
Medical Nursing - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
Dwarfism Quiz
Medical Nursing
Preparing questions...
Choose your answer and keep your streak alive.
Great effort.
Here is your quick performance summary.

Well compilation thanks