

Immunization is a process of deliberate inoculation of live attenuated or dead vaccines and toxoids to induce immunity against a specific disease. Immunization against a specific disease provides artificially acquired active immunity. The principle of immunization is to increase specific immunity to infection by administration of either immune serum (passive immunization) or by administration of an antigen (active immunization).
Artificially acquired immunity against some diseases may require periodic booster injections to keep an adequate antibody level (or antibody titer) circulating in the blood. A booster injection is the administration of an additional dose of the vaccine to boost the production of antibodies to a level that will maintain the desired immunity. The booster is given months or years after the initial vaccine and may be needed because the life of some antibodies is short.
- Toxoids: is a toxin that is attenuated (or weakened) but still capable of stimulating the formation of antitoxins.
- Vaccines: Special preparations of antigenic materials that can be used to stimulate the development of antibodies.
- Immune Globulins: Preparations containing antibodies against infectious micro-organisms, usually prepared from human plasma or serum.
- Antisera: Sterile preparations containing immunoglobulins obtained from the serum of immunized animals by purification. They have the power of neutralizing venoms or bacterial toxins.
The principal goal of immunization is to increase specific immunity to infection. This can be achieved through two main strategies: active immunization and passive immunization.
Passive immunization is the administration of already active antibodies to prevent or ameliorate infection. It gives immediate protection but immunity lasts for a short period of time. Passive immunisation is used in post-exposure prophylaxis in immunocompetent hosts when immediate protection is required following exposure to the infection e.g. tetanus.
- Hepatitis B
- Rabies
- Tetanus
- Diphtheria
- Passive immunisation can be lifesaving if toxin is already circulating.
- Prompt availability of large amount of antibodies.
- Protection is short-lived (up to 6 months) as the borrowed antibodies are eventually degraded and cleared.
- Use of human antisera has dangers of transmitting infections like HIV or Hepatitis.
- Antisera are expensive compared to vaccines.
- They need to be kept cool and have limited life span.
Active immunization is a process of increasing resistance to infection whereby micro-organisms or products of their activity act as antigens and stimulate certain body cells to produce antibodies with a specific productive capacity. It may be a natural process following recovery from an infection, or an artificial process induced by the administration of vaccines.
Active immunization is a process where the individual's own immune system is stimulated to produce antibodies and memory cells against a specific pathogen. This is achieved by administering an antigen, usually in the form of a vaccine. It may be a natural process following recovery from an infection, or an artificial process induced by vaccination.
- To protect susceptible individuals against specific infections.
- To reduce the incidence of infection in the community, leading to herd immunity.
- To eliminate an infection in a particular country or worldwide (e.g., the successful eradication of smallpox and the ongoing effort to eradicate polio).
Artificially acquired immunity against some diseases may require periodic booster injections to keep the antibody level (titer) adequate for protection. A booster is an additional dose given months or years after the primary vaccination series to "boost" the immunological memory and production of antibodies.
- Offers long-term, often lifelong, immunity due to the formation of memory cells.
- Has a slow onset of action, as it takes time (days to weeks) for the body to mount a primary immune response and become fully protected.
Vaccines are special preparations of antigenic materials designed to stimulate the development of antibodies and confer active immunity. Vaccination refers to the administration of a vaccine.
These vaccines use live microorganisms that have been weakened (attenuated) so they can still replicate but do not cause disease in healthy individuals. They typically provide long-lasting immunity with a single dose (with some exceptions like OPV).
Examples: BCG, Measles, Mumps, Rubella, Oral Polio (OPV), Yellow Fever.
- Live vaccines give longer protection than killed vaccines.
- One dose of the vaccine is usually sufficient with exception of oral polio vaccines.
- Live vaccines are often unstable e.g. measles and polio need to be stored at -20°C.
- Live vaccines may not work in the presence of circulating antibodies e.g. measles vaccine has to be given around 9 months of age when maternal antibodies have gone.
- Live vaccines may cause disease if the host is immuno deficient as in HIV infection.
- Live vaccines occasionally interfere with each other so that the immune response is not so great if given together.
These vaccines use whole bacteria or viruses that have been killed and can no longer replicate. They are very safe but usually require a series of injections and booster doses to produce an adequate response.
Examples: Inactivated Polio Vaccine (IPV), Rabies vaccine, Hepatitis A vaccine, whole-cell Pertussis vaccine.
These vaccines use bacterial toxins that have been chemically inactivated to become harmless toxoids. They stimulate the production of antitoxins.
Examples: Tetanus toxoid, Diphtheria toxoid.
Disadvantages: Immunity can be short-lived, requiring booster doses.
- Routine immunization of infants and children.
- Immunization of adults against tetanus.
- Immunization of adults at high risk for certain diseases (e.g., pneumococcal and influenza vaccines).
- Immunization of children or adults at risk for exposure to a particular disease (e.g., hepatitis A for those going to endemic areas).
- Immunization of pre-pubertal girls or non-pregnant women of childbearing age against rubella and cervical cancer.
Adverse reactions from the administration of vaccines or toxoids are usually mild.
- Chills, Fever, muscular aches and pains, rash, and lethargy may be present.
- Pain and tenderness at the injection site may also occur.
- Although rare, a hypersensitivity reaction may occur.
- Hypersensitivity: Individuals with known severe allergic reactions to vaccine components or previous doses should not receive the vaccine.
- Vaccines and toxoids are generally contraindicated during acute febrile illnesses, leukemia, lymphoma, immunosuppressive illness or drug therapy, and non-localized cancer.
- The measles, mumps, rubella, and varicella vaccines are contraindicated in patients who have had an allergic reaction to gelatin, neomycin, or a previous dose of one of the vaccines.
- The measles, mumps, rubella, and varicella vaccines are generally contraindicated during pregnancy, especially during the first trimester, because of the theoretical danger of birth defects. Women are instructed to avoid becoming pregnant for at least 3 months after receiving these vaccines.
- Antisera: Sterile preparations containing immunoglobulins obtained from the serum of immunized animals (e.g., horses). They are used to neutralize venoms or bacterial toxins.
- Immunoglobulins: Preparations containing specific antibodies, usually prepared from pooled human plasma. They are used for passive immunization.
- Should be able to induce an adequate and appropriate immune response without causing active infection.
- The vaccine should be safe with minimal side effects.
- The vaccine should be stable and remain potent during storage and transportation.
- The vaccine should be cheap if it is to be used on a large scale.
- It should be easy to administer.
- It should be highly purified so that it consists of one or only a few antigens.
Autoimmune diseases occur when the immune system loses its ability to distinguish "self" from "non-self" and mistakenly begins to attack the body's own cells and tissues. This failure of self-tolerance can be triggered by a combination of genetic susceptibility, environmental factors, and infections.
It is thought that female hormones like estrogen may enhance the inflammatory response, which could be one reason why autoimmune diseases are often more common or severe in women than in men.
| Disease | Part of the Body Primarily Affected |
|---|---|
| Rheumatoid Arthritis | Cartilage and linings of the joints. |
| Graves' Disease | Thyroid gland (causes hyperthyroidism). |
| Insulin-Dependent Diabetes Mellitus (Type 1) | Insulin-producing beta cells of the pancreas. |
| Multiple Sclerosis (MS) | Myelin sheath of nerves in the brain and spinal cord. |
| Psoriasis | Skin cells. |
| Ankylosing Spondylitis | Joints of the spine. |
This section provides a detailed breakdown of the key vaccines used in immunization programs, including their type, indications, dose, side effects, contraindications, and special precautions.
- Type: Live attenuated bacterial vaccine.
- Indications: Active immunization against severe forms of tuberculosis (TB) in children, such as TB meningitis and miliary TB. Protection against leprosy (in some contexts where leprosy is endemic and BCG is used for this purpose).
- Dose:
- Infants less than 12 months: 0.05ml administered intradermally in the right upper arm.
- Adults and children over 12 months: 0.1ml administered intradermally in the right upper arm.
- Side Effects: A localized papule, sore, and then ulceration at the injection site is a normal, expected reaction that heals to form a permanent scar. Lymphadenitis (swelling of local lymph nodes). Keloid formation at the scar site. Abscess formation at the injection site (rare, more severe). Osteitis/Osteomyelitis (inflammation of bone, very rare systemic complication). Disseminated BCG infection: A rare but severe complication that can occur in severely immunosuppressed patients.
- Contraindications: Severely immunocompromised patients (e.g., advanced HIV/AIDS, congenital immunodeficiency, individuals on immunosuppressive therapy). Generalized skin conditions like eczema or scabies at the intended injection site. Patients undergoing antibacterial treatment for tuberculosis. Known allergy to any component of the vaccine. Infants weighing less than 2 kg. Individuals with a positive tuberculin skin test (PPD) or IGRA (Interferon Gamma Release Assay), as this may indicate latent TB infection. Acute severe febrile illness (generally a temporary contraindication).
- Precautions: Pregnancy (though it may be given if the risk of TB exposure is high and benefits outweigh risks, especially in high-endemic areas). Infants born to HIV-positive mothers (careful risk-benefit assessment; may be given if the infant is asymptomatic for HIV and the risk of TB exposure is high, but generally avoided if HIV status is confirmed and symptomatic). Concomitant use with other live vaccines (spacing may be recommended by national guidelines, though many routine schedules allow co-administration).
- Type: A combination vaccine containing Diphtheria and Tetanus toxoids and an inactivated (killed) whole-cell Pertussis bacteria component. Note: Modern DPT vaccines often use acellular pertussis (aP) components (DTaP) which have fewer side effects, but the provided text specifies whole-cell. Pentavalent typically contains DPT-HepB-Hib.
- Indications: Active immunization against Diphtheria, Tetanus, and Pertussis (whooping cough) in infants and young children. Primary vaccination series for infants as part of routine immunization programs.
- Dose: Given as part of the Pentavalent vaccine series: 0.5ml intramuscularly at 6, 10, and 14 weeks of age. Specific schedules may vary by national immunization guidelines.
- Side Effects:
- Common: Pain, redness, and swelling at the injection site; fever; irritability; restlessness; loss of appetite; drowsiness.
- Less common: Persistent, inconsolable crying (lasting 3 hours or more); high fever (>=40.5°C); febrile seizures (very rare).
- Rare: Anaphylaxis (severe allergic reaction); hypotonic-hyporesponsive episodes (HHE); peripheral neuropathy; severe neurological reactions (especially associated with the whole-cell pertussis component, e.g., encephalopathy). Injection site nodule/lump which can persist for weeks.
- Contraindications: Known hypersensitivity to any of the ingredients of the vaccine or a severe allergic reaction to a previous dose. A history of a severe neurological reaction (e.g., encephalopathy not attributable to another identifiable cause) within 7 days of a previous dose of pertussis-containing vaccine. Progressive neurological disorder, including infantile spasms, uncontrolled epilepsy, or progressive encephalopathy (vaccination should be deferred until the condition has stabilized). Acute severe febrile illness (vaccination should be deferred until recovery).
- Precautions: Minor illnesses (e.g., mild upper respiratory infection, low-grade fever) are generally NOT contraindications. Family history of seizures or other neurological disorders (not a contraindication but requires observation after vaccination). History of a reaction following a previous dose that is considered a precaution (e.g., temperature ≥40.5°C within 48 hours not due to another cause, collapse/shock-like state within 48 hours, persistent crying lasting ≥3 hours within 48 hours, seizures with or without fever within 3 days). In such cases, benefits versus risks of subsequent doses should be carefully considered, and acellular pertussis vaccines (DTaP) might be preferred if available.
- Type: Toxoid vaccine. Td contains tetanus toxoid and a reduced dose of diphtheria toxoid.
- Indications: Active immunization against tetanus. Prevention of neonatal tetanus through the immunization of pregnant women and women of childbearing age. Boostering immunity against tetanus and diphtheria in adolescents and adults. Post-exposure prophylaxis for tetanus following wounds (often in combination with Tetanus Immunoglobulin if indicated).
- Dose (for Women of Childbearing Age and General Adult Boosters):
- Primary Series: Varies, but often 2-3 doses given at intervals (e.g., 0 and 4-8 weeks).
- TT1 (for Pregnant Women/WOCBA): 0.5ml deep IM or SC at first contact/early in pregnancy.
- TT2: 0.5ml at least 4 weeks after TT1 (preferably before 36 weeks of pregnancy).
- TT3: 0.5ml at least 6 months after TT2.
- TT4: 0.5ml at least 1 year after TT3.
- TT5: 0.5ml at least 1 year after TT4. (5 doses provide long-lasting protection, often considered lifelong for practical purposes if fully completed).
- Booster Doses: Recommended every 10 years for adolescents and adults.
- Side Effects: Common: Local reactions like pain, tenderness, redness, swelling, and a lump at the injection site. These are usually mild and resolve within a few days. Less common: Low-grade fever, headache, body aches, tiredness. Rare: Anaphylaxis (severe allergic reaction); brachial neuritis (inflammation of nerves in the arm, very rare); peripheral neuropathy. Arthus-type reactions (severe local reaction with swelling and pain) can occur, particularly in adults who receive frequent booster doses.
- Contraindications: Known hypersensitivity to any component of the vaccine or a severe allergic reaction to a previous dose. A history of a severe Arthus-type hypersensitivity reaction following a previous dose of tetanus or diphtheria toxoid-containing vaccine (usually not given again for at least 10 years). Acute severe febrile illness (defer vaccination until recovery).
- Precautions: Minor illnesses (e.g., mild upper respiratory infection, low-grade fever) are generally NOT contraindications. History of Guillain-Barré Syndrome (GBS) within 6 weeks of a previous dose of tetanus toxoid-containing vaccine (decision to vaccinate should weigh benefits against potential risks).
- Type: Live attenuated virus vaccine.
- Indications: Active immunization against Measles, Mumps, and Rubella. Recommended for all children as part of routine immunization schedules. Prevention of congenital rubella syndrome in women of childbearing age (ensure non-pregnant at vaccination and avoid pregnancy for recommended period). Outbreak control measures in susceptible populations.
- Dose: 0.5ml administered by deep subcutaneous or intramuscular injection. First dose: Typically at 12-15 months of age (some regions, like Uganda, may give first measles dose earlier at 9 months, and then MMR later). Second dose: Recommended for sustained immunity, often at 4-6 years of age (e.g., prior to school entry) or later, depending on national schedules.
- Side Effects: Common (5-12 days after dose 1): Fever (up to 15%), malaise, and a non-infectious, non-contagious maculopapular rash (measles-like) (5%). Common (3-4 weeks after dose 1): Parotid swelling (mild, mumps-like symptoms, <1%). Common (2-4 weeks after dose 1, particularly in post-pubertal females): Transient arthralgia or arthritis (joint pain/inflammation) related to the rubella component. Rare: Thrombocytopenia (transient low platelets, 1 in 30,000 to 40,000 doses). Very Rare: Febrile seizures (usually benign, related to the fever, not the vaccine itself causing epilepsy); anaphylaxis (severe allergic reaction, approx. 1 in 1,000,000 doses).
- Contraindications: Pregnancy (known or suspected). Women should be advised to avoid pregnancy for at least 1 month after vaccination. Severe immunosuppression (e.g., congenital immunodeficiency, HIV with severe immunosuppression, leukemia, lymphoma, generalized malignancy, high-dose corticosteroids, chemotherapy, radiation therapy). Known hypersensitivity to vaccine components (e.g., neomycin, gelatin). A history of a severe allergic reaction (anaphylaxis) to a previous dose of MMR vaccine. Receipt of blood products (e.g., transfusions, immunoglobulin) containing antibodies within a certain period (typically 3-11 months, depending on the product), as these antibodies can interfere with vaccine efficacy. Acute severe febrile illness (defer vaccination until recovery).
- Precautions: History of convulsions or epilepsy in the patient or family (parents should be advised on managing fever and monitoring for seizures, but vaccination is generally safe). Individuals with mild illness (e.g., low-grade fever, upper respiratory infection) can generally be vaccinated. The vaccine should be cautiously administered to individuals with a history of thrombocytopenia or thrombocytopenic purpura, as a recurrence is possible (risk vs. benefit should be assessed). Recent receipt of another live injected vaccine within the last 4 weeks (some guidelines prefer spacing by 4 weeks if not co-administered, but often co-administration is acceptable).
- Type: Recombinant subunit vaccine (contains inactivated Hepatitis B surface antigen, HBsAg), produced in yeast.
- Indications: Active immunization against Hepatitis B infection. Universal vaccination of all infants and children as part of routine immunization programs. Crucial for high-risk groups: infants born to HBsAg-positive mothers (should receive birth dose and Hepatitis B Immunoglobulin - HBIG); healthcare personnel; public safety workers; hemodialysis patients; patients with chronic liver disease; individuals with multiple sexual partners; injecting drug users; close contacts and sexual partners of HBsAg carriers; international travelers to endemic areas.
- Dose:
- Infants: First dose given within 24 hours of birth (birth dose), then typically as part of the Pentavalent vaccine at 6, 10, and 14 weeks (some schedules use a 0, 1, 6 month pattern if given as stand-alone).
- Children and Adolescents: Typically a 2- or 3-dose series depending on the specific vaccine and age.
- Adults: Typically a 3-dose series (e.g., 0, 1, and 6 months) or a rapid 4-dose series for specific needs.
- Administered intramuscularly, usually in the anterolateral thigh for infants/young children and deltoid muscle for older children/adults.
- Side Effects: Common: Pain, tenderness, redness, and swelling at the injection site (up to 29%). Less common: Low-grade fever, headache, myalgia (muscle aches), arthralgia (joint pain), fatigue, gastrointestinal disturbances (nausea, diarrhea). These are usually mild and transient. Rare: Anaphylaxis (severe allergic reaction, extremely rare).
- Contraindications: Known hypersensitivity to yeast or any other component of the vaccine. A history of a severe allergic reaction (anaphylaxis) to a previous dose of Hepatitis B vaccine. Acute severe febrile illness (defer vaccination until recovery).
- Precautions: Immunocompromised patients (e.g., those on dialysis, HIV-infected individuals, transplant recipients) may have a diminished immune response and may require higher doses, additional doses, or post-vaccination serologic testing to ensure adequate protection. Mild illness (e.g., low-grade fever, common cold) is generally not a contraindication. Use with caution in pregnancy and lactation (no evidence of harm, but generally recommended if risk of exposure is high). The benefits of vaccinating pregnant women at high risk for HBV infection outweigh potential risks to the fetus.
- Type: Live attenuated virus vaccine (17D strain).
- Indications: Active immunization against yellow fever, especially for residents of and travelers to endemic areas. Required for entry into certain countries where yellow fever is endemic or where there's a risk of transmission. Mass vaccination campaigns in areas with ongoing outbreaks or high risk.
- Dose: A single 0.5ml dose administered by subcutaneous injection (preferred) or intramuscular injection. Typically given at 9 months of age in endemic regions. Provides lifelong immunity for most people after a single dose, according to WHO. Some countries may still require revaccination certificates every 10 years for entry, so checking international health regulations is crucial for travelers.
- Side Effects: Mild (common, 5-10 days after vaccination): Headache, myalgia, low-grade fever, flu-like symptoms, injection site reactions (pain, redness, swelling). These usually resolve within a few days. Rare but serious: Anaphylaxis (severe allergic reaction, approx. 1 in 130,000 doses). Very Rare but severe: Yellow Fever Vaccine-Associated Neurologic Disease (YEL-AND), typically neurological symptoms like encephalitis or meningitis (occurs in approx. 0.8 in 100,000 doses). Very Rare and most severe: Yellow Fever Vaccine-Associated Viscerotropic Disease (YEL-AVD), a multi-organ failure resembling severe yellow fever (occurs in approx. 0.3 in 100,000 doses, higher risk in older individuals).
- Contraindications: Infants under 6 months of age (and used with caution between 6-8 months due to higher risk of YEL-AND). Severe immunosuppression (e.g., congenital immunodeficiency, HIV with CD4 count <200 cells/mm3, leukemia, lymphoma, generalized malignancy, high-dose corticosteroids, chemotherapy, radiation therapy). Known hypersensitivity to eggs, egg proteins, or any other component of the vaccine (e.g., gelatin, chicken protein). Individuals with a history of thymus disorders (e.g., thymoma, thymectomy, myasthenia gravis, DiGeorge syndrome) due to increased risk of YEL-AVD. Acute severe febrile illness (defer vaccination until recovery).
- Precautions: Age 60 years or older: Increased risk of YEL-AND and YEL-AVD. Benefits and risks should be carefully weighed, especially for first-time vaccine recipients. Pregnancy: Generally not recommended unless travel to an endemic area with high risk of exposure cannot be avoided. Risk vs. benefit assessment is crucial. Breastfeeding: Generally not recommended if the infant is under 9 months due to theoretical risk of transmission through breast milk, unless the risk of maternal infection is high. Mild illness is generally not a contraindication. As a live vaccine, it should ideally be given simultaneously with other live vaccines or spaced by at least 4 weeks.
- Type: There are two main types, which are not interchangeable:
- Pneumococcal Conjugate Vaccine (PCV): Such as PCV10 (used in Uganda) or PCV13, PCV15, PCV20. The polysaccharide capsule antigens are "conjugated" (joined) to a protein carrier, which creates a strong and lasting immune response, especially in infants and young children, and induces T-cell dependent memory.
- Pneumococcal Polysaccharide Vaccine (PPSV23): Contains antigens from 23 different serotypes. It provides broader serotype coverage but elicits a T-cell independent immune response, which is weaker and shorter-lived, and not effective in children under 2 years old. It is primarily used for adults and high-risk older children.
- Indications: Active immunization against diseases caused by Streptococcus pneumoniae, including pneumonia, meningitis, bacteremia (invasive pneumococcal disease), and otitis media. Crucial for high-risk populations: all infants and young children (PCV); adults over 65 years (PCV and/or PPSV23); and individuals with underlying medical conditions such as sickle cell disease, functional or anatomic asplenia, chronic heart, lung, or kidney disease, diabetes mellitus, and immunosuppression (PCV and/or PPSV23).
- Dose:
- PCV (Routine for infants): 0.5ml IM at 6, 10, and 14 weeks (Uganda schedule). Other common schedules include 2, 4, 6 months with a booster at 12-15 months, or 2, 4 months with a booster.
- PPSV23 (for adults/high-risk): 0.5ml IM or deep SC as a single dose. Revaccination with PPSV23 may be considered for those at highest risk after 5 years. Sequential vaccination with PCV followed by PPSV23 is often recommended for certain adult risk groups.
- Side Effects: Common: Fever, irritability, drowsiness, and local reactions at the injection site (pain, redness, swelling, tenderness). These are generally mild and resolve within 1-2 days. Less common: Decreased appetite, vomiting, diarrhea. Rare: Anaphylaxis (severe allergic reaction).
- Contraindications: A severe allergic reaction (anaphylaxis) to a previous dose of the specific pneumococcal vaccine or to any component of the vaccine. Acute severe febrile illness (defer vaccination until recovery).
- Precautions: Mild illness or low-grade fever is generally not a contraindication. In individuals with compromised immune systems (e.g., due to HIV infection, immunosuppressive therapy), the immune response to the vaccine may be diminished. For PPSV23, administer with caution to individuals with a history of severe local reactions to previous doses.
- Type: Can be a polysaccharide vaccine (e.g., MPSV4) or, more effectively, a conjugate vaccine (e.g., MCV4 or MenACWY). They are formulated against the most common disease-causing serogroups of Neisseria meningitidis: A, C, Y, and W-135 (quadrivalent vaccines). Monovalent (e.g., Men C) and bivalent (e.g., Men A+C) preparations are also available. Separate vaccines exist for serogroup B (MenB vaccines).
- Indications: Active immunization against meningococcal meningitis and septicemia caused by vaccine-preventable serogroups. Essential for individuals residing in or traveling to the "meningitis belt" of sub-Saharan Africa, particularly during epidemic seasons. Recommended for travelers to high-risk areas, military recruits, university students living in dormitories, and individuals with certain medical conditions (e.g., asplenia, persistent complement component deficiencies, those on eculizumab). Outbreak control in specific populations.
- Dose: 0.5ml by deep subcutaneous (polysaccharide) or intramuscular (conjugate) injection as a single dose or multi-dose series depending on the vaccine type, age, and schedule. For conjugate vaccines, routine vaccination for adolescents is common, with a booster dose.
- Side Effects: Common: Local pain, redness, and swelling at the injection site; headache; fatigue; malaise; muscle aches; low-grade fever. These are usually mild and transient. Rare: Allergic reactions, including anaphylaxis.
- Contraindications: Known severe allergy to any ingredient in the vaccine or a severe allergic reaction to a previous dose. Acute severe febrile condition (postpone vaccination until recovery).
- Precautions: Use with caution during pregnancy: Generally recommended only if the benefit of vaccination outweighs the potential risk to the fetus, such as in high-risk travel or outbreak situations. The immune response from polysaccharide vaccines in children under 2 years may be short-lived and does not induce herd immunity or memory, making conjugate vaccines preferred for this age group and for broader public health impact. Individuals with mild illness are generally not a contraindication.
- Type: An oral vaccine. There are two main types:
- Live attenuated preparation: (e.g., Vaxchora) - single dose.
- Inactivated whole-cell preparations: (e.g., Dukoral, Shanchol, Euvichol) - usually multi-dose. These contain killed whole cells of Vibrio cholerae, often combined with B subunit of cholera toxin (Dukoral).
- Indications: Prophylactic immunization for travelers over 2 years of age (or younger depending on the specific vaccine) going to areas with high risk of cholera infection, particularly those who will be in areas with poor sanitation and hygiene. Used in outbreak control and humanitarian settings to reduce transmission, but is not a substitute for providing safe water, sanitation, and hygiene (WASH) interventions. Not typically part of a routine national immunization schedule in most non-endemic countries.
- Dose: Varies significantly by vaccine type and manufacturer:
- Inactivated (Dukoral): Requires a multi-dose schedule. Children 2-6 years: 3 doses, with 1-6 weeks between doses. Adults and children >6 years: 2 doses, with 1-6 weeks between doses. A booster dose is typically recommended after 2 years for continued protection.
- Live attenuated (Vaxchora): Single dose for individuals aged 2 to 64 years.
- Side Effects: Common: Abdominal discomfort, mild diarrhea, nausea, vomiting, headache, loss of appetite. These are usually mild and transient. Rare: Hypersensitivity reactions.
- Contraindications: History of hypersensitivity or severe allergic reaction to any of the ingredients of the specific vaccine or a previous dose. Should be postponed during an acute moderate to severe gastrointestinal illness (e.g., acute diarrhea, vomiting) or acute moderate to severe febrile illness. For live attenuated vaccines: severe immunocompromise (similar to other live vaccines).
- Precautions: Efficacy may be reduced if taken concurrently with certain medications (e.g., antacids, antibiotics). Check specific product information. Not a substitute for practicing safe food and water hygiene. Protection is not 100%, and duration of protection varies by vaccine. Pregnancy and breastfeeding: Consult with a healthcare provider; generally, only given if the risk of exposure is high and benefits outweigh potential risks.
- Type: An inactivated (killed) virus vaccine. Prepared from purified chick embryo cell culture (PCEC), human diploid cell culture (HDCV), or Vero cell culture.
- Indications:
- Post-Exposure Prophylaxis (PEP): To prevent the development of rabies after a person has been bitten, scratched, or had mucous membrane exposure to a potentially rabid animal. This is a medical emergency, as rabies is nearly 100% fatal once symptoms begin. PEP includes immediate wound cleansing, vaccine administration, and in severe cases, Rabies Immunoglobulin (RIG).
- Pre-Exposure Prophylaxis (PrEP): For persons at high and continuous risk of exposure, such as veterinarians, animal handlers, laboratory workers handling the rabies virus, speleologists, and travelers to rabies-endemic areas who may not have immediate access to medical care.
- Dose:
- Pre-exposure (PrEP): Standard: 1ml (or 0.5ml for intradermal) IM injection on days 0, 7, and 21 or 28. Newer schedules (e.g., 2 doses for some vaccines) are being explored.
- Post-exposure (PEP): For unvaccinated individuals: 1ml IM injection on days 0, 3, 7, and 14 (4-dose regimen). In some settings, a 5-dose regimen (days 0, 3, 7, 14, 28) or 2-site intradermal regimens are used. For previously vaccinated individuals (PrEP complete): 1ml IM injection on days 0 and 3 (2-dose regimen), no RIG needed.
- For severe exposures, especially in unvaccinated individuals, Rabies Immunoglobulin (RIG) should also be infiltrated around the wound and into the wound on day 0, as much as anatomically feasible.
- Route: Intramuscular (IM) injection, usually in the deltoid muscle for adults and anterolateral thigh for young children. Intradermal (ID) routes are also approved for certain schedules in some regions, which can save vaccine.
- Side Effects: Common: Pain, redness, swelling, and itching at the injection site (up to 30-70%). Systemic: Fever, headache, dizziness, myalgia (muscle aches), malaise (general discomfort), nausea, abdominal pain. These are usually mild. Rare: Hypersensitivity reactions (e.g., urticaria, rash, anaphylaxis). Neurological complications are extremely rare.
- Contraindications: There are generally no contraindications to PEP once exposure to rabies is suspected or confirmed, given the fatal nature of the disease. For PrEP, contraindications are similar to other inactivated vaccines: severe allergic reaction to a previous dose or component of the vaccine, or acute moderate to severe febrile illness (defer until recovery).
- Precautions: Administer with caution to individuals with a history of hypersensitivity reactions to previous doses. Pregnancy and breastfeeding: Not a contraindication for PEP; for PrEP, it should be given if the risk of exposure is substantial. Immunocompromised individuals: May require additional doses or serologic testing to confirm adequate immune response after PrEP, and for PEP, the full recommended series with RIG is crucial.
- Type: An inactivated (killed) virus vaccine. Whole virus particles are grown in cell culture, purified, and inactivated with formalin.
- Indications: Active immunization against Hepatitis A infection, a common cause of acute viral hepatitis transmitted via the fecal-oral route. Recommended for: Travelers to high-risk areas, children as part of routine immunization schedules, laboratory workers, patients with chronic liver disease, individuals who use parenteral or illicit drugs, homosexual and bisexual men, individuals who work with nonhuman primates, people with clotting factor disorders, close contacts of adoptees from endemic countries, and individuals who change partners frequently.
- Dose: Typically a two-dose series given by intramuscular injection. An initial dose (e.g., 0.5ml or 1.0ml depending on age and specific vaccine) is followed by a booster dose 6-12 months later (or up to 18 months for some vaccines). For combined Hepatitis A and B vaccine (Twinrix), the schedule is typically 3 doses over 6 months (0, 1, 6 months) or a rapid 4-dose schedule.
- Side Effects: Common: Pain, tenderness, redness, and swelling at the injection site. Systemic: Headache, fever (low-grade), fatigue, malaise (general discomfort), myalgia (muscle aches). Less common: Nausea, loss of appetite, irritability, skin rash. Rare: Allergic reactions, including anaphylaxis.
- Contraindications: Known hypersensitivity or severe allergic reaction to any component of the vaccine or a previous dose. Acute moderate to severe febrile illness (defer vaccination until recovery).
- Precautions: Use with caution in patients with altered immunity; while generally safe, the immune response may be diminished. Pregnancy and lactation: Data on safety are limited, but the vaccine is considered safe, and vaccination should be considered if the risk of exposure to HAV is high.
- Type: This is a form of passive immunization, not a vaccine. It is a preparation of purified human immunoglobulin G (IgG) antibodies directed against the Rhesus D (RhD) antigen found on the surface of red blood cells. It works by destroying any Rh-positive fetal red blood cells that enter the Rh-negative mother's circulation before her immune system can produce its own antibodies.
- Indications: To prevent a Rhesus-negative (Rh-negative) mother from forming her own anti-RhD antibodies when exposed to Rhesus-positive (Rh-positive) fetal red blood cells. This prevents Rh isoimmunization, which can cause severe Hemolytic Disease of the Newborn (HDN) or erythroblastosis fetalis in subsequent Rh-positive pregnancies. It is administered in Routine Antenatal Prophylaxis (RAP), Postnatal Prophylaxis, and following any potential sensitizing event (Abortion, Miscarriage, Ectopic pregnancy, Hydatidiform mole, Stillbirth, Amniocentesis, Chorionic villus sampling, Cordocentesis, External cephalic version, Abdominal trauma, Antepartum hemorrhage, or Transfusion of Rh-positive blood products).
- Dose:
- Antenatal Prophylaxis: Typically 300 mcg (1500 IU) IM around 28 weeks of gestation.
- Postnatal Prophylaxis: Typically 300 mcg (1500 IU) IM within 72 hours of delivering an Rh-positive infant.
- For sensitizing events earlier in pregnancy or with smaller potential bleeds, a lower dose (e.g., 50-120 mcg) may be used. For suspected or quantified large feto-maternal hemorrhage, additional doses may be required. One 300 mcg dose typically neutralizes 15 mL of Rh-positive red blood cells.
- Side Effects: Common: Local tenderness, pain, swelling, and redness/stiffness at the injection site. Less common systemic effects: Low-grade fever, headache, malaise, nausea, vomiting, myalgia. Rare: Allergic reactions, including urticaria, rash, and very rarely, severe anaphylactic reactions. Extremely rare: Hemolysis (in the recipient).
- Contraindications: Should NEVER be given to an Rh-positive individual. Should NEVER be given to the Rh-positive newborn infant. Contraindicated in individuals with a known severe allergy or hypersensitivity to human immunoglobulins or any component of the preparation. Contraindicated in individuals with isolated IgA deficiency with known anti-IgA antibodies. It is NOT indicated for an Rh-negative woman who has already been sensitized and has produced anti-RhD antibodies.
- Drug Interactions: As Anti-D immunoglobulin is a preparation of antibodies, it can interfere with the immune response to live virus vaccines (e.g., MMR, Varicella, Oral Polio, Yellow Fever). Live attenuated vaccinations should generally be postponed for at least 3 months (and up to 6 months depending on the dose of immunoglobulin). Concomitant administration with other passive antibodies should be avoided unless specifically indicated.
- Storage: Typically stored refrigerated at 2°C to 8°C (36°F to 46°F). Do not freeze. Protect from light.
| Vaccine | Details |
|---|---|
| Measles–Rubella Vaccine | Available preparations: Injection powder for solution (live attenuated). Indications: Active immunization against measles and rubella. Dose: 0.5ml SC at 9 months and 18 months (left upper arm). Side effects: Fever, Headache and Malaise, Rashes and Thrombocytopenia. Contraindications: Hypersensitivity to any antibiotic present in the vaccine, Pregnancy, Immunosuppression. |
| Measles, Mumps and Rubella Vaccine (MMR vaccine) | Available brands: Trimovax®, Priovix®. Dose: By deep SC or by intramuscular injection 0.5ml (usually at 12-15 months). Indications: Active immunization against measles, mumps and rubella. Contraindications: Pregnancy, Hypersensitivity to components like neomycin, Immunosuppressed patients, Children who have received another live vaccine by injection within 4 weeks. Side effects: Fever and Malaise, Parotid swelling and Rashes. Precautions: History of convulsions. |
| BCG Vaccine | Available preparations: Powder for solution of live bacteria of strain derived from the bacillus of calmette and Guerin. Indications: Active immunization against tuberculosis. Dose: 0.05ml intradermal in the right upper arm to neonates; 0.1ml intradermal on the upper arm (children > 12 months). Side effects: Keloid, Lymphadenitis, Localized necrotic ulceration, Disseminated BCG infection in immunosuppressed patients, Anaphylaxis. Contraindications: Generalized oedema, Immunosuppressed patients, Antibacterial treatment. Precautions: Pregnancy, Eczema, Scabies. Vaccine site must be lesion free. |
| Diphtheria, Pertussis and Tetanus (DPT) Vaccine | Available brand: Tripacel®, Infantrix®. Indications: Active immunization against diphtheria, tetanus and pertussis. Dose: Infant: 0.5ml by intramuscular or deep SC injection at 6, 10 and 14 weeks. Side effects: Irritability and Limb swelling, Peripheral neuropathy, Urticaria, Fever, Restlessness and Malaise, Myalgia, Headache and Loss of appetite. Contraindications: Known hypersensitivity to any of the ingredients. |
| Tetanus Toxoid Vaccine | Available brand: Tetavax®. Indications: Active immunization against tetanus and neonatal tetanus. Dose: Women 15-49 years of age. 0.5ml deep SC or intramuscular injection. 5 doses (TT1-TT5) are required for lifelong protection. Side effects: Peripheral neuropathy. |
| Anti-tetanus Immunoglobulin | Available brand: Tetanea®. Indications: Passive immunization against tetanus as part of the management of tetanus prone wounds. Dose: Adult and Children: 1ml by IM injection. Side effects: Local reactions, Fever, Pain and tenderness at site of injection, Headache. |
| Yellow Fever Vaccine | Available brand: Stamaril®. Indications: Active immunization against yellow fever. Dose: Infant at 9 months: 0.5ml by SC injection. Side effects: Headache, Myalgia, Fever, Influenza like symptoms. Contraindications: Immunosuppressed patients, Hypersensitivity to any ingredient (including eggs), Infant under 4 months of age. |
| Typhoid Vaccine | Available brands: Typhim VI®, Typherix PFS®. Indications: Active immunization against typhoid. Dose: Adult and Children > 2 years: By deep SC or intramuscular 0.5ml with booster doses every 3 years for those at continued risk. Side effects: Headache, Nausea, Myalgia, Malaise. Contraindications: Immunosuppressed patients, Febrile illness, Hypersensitivity. |
| Pneumococcal Vaccine | Available brand: Pneumo 23® (Polysaccharide version). Indications: Immunization against pneumococcal infections in Sickle cell disease Children > 2 years of age, and immunocompromised patients > 5 years. Dose: Adults and Children > 2 years: 0.5ml deep SC or IM as a single dose. Side effects: Fever, Myalgia. Contraindication: Severe allergic reaction to any ingredients. |
| Meningococcal Vaccine | Available brand: Meningo A + C®, Mencevax ACWY®. Indications: Active immunization against Neisseria meningitidis infections. Dose: Adult and Children > 2 years of age. 0.5ml deep SC or IM injection as a single dose. Side effects: Allergic reaction, Anaphylaxis, Erythema. Contraindications: Known allergy, Febrile conditions. |
| Cholera Vaccine | Available brand: Dukoral® (Oral). Indications: Immunization for travellers > 2 years of age at high risk. Dose: Multiple oral doses given at intervals of at least 1-6 weeks. Side effects: Abdominal discomfort, Diarrhoea, Headache, Fever, Vomiting, Nausea, Loss of appetite. Contraindications: Hypersensitivity, Acute GIT or febrile illness. |
| Rabies Vaccine | Available brand: Verorab®. Indications: Pre-exposure prophylaxis and post-exposure treatment to prevent rabies. Dose: Pre-exposure: 1ml on days 0, 7 and 28. Post-exposure: 1ml on days 0, 3, 7, 14 and 30. Side effects: Pain/erythema at injection site, Nausea, Fever, Headache, Myalgia, Malaise. |
| Hepatitis B Vaccine | Available brand: Euvax B®, Engerix B®. Indications: Active immunization against Hepatitis B infection for all infants and high-risk persons. Dose: Infants: 0.5ml IM at 6, 10, 14 weeks. Adults: 1ml IM, 3 doses. Side effects: Abdominal pain, GIT disturbance, Peripheral neuropathy, Myalgia, Lymphadenopathy. Precautions: Immunocompromised patients may need further dose, Pregnancy, Lactation. |
| Hepatitis A Vaccine | Available brand: Avaxim®, Havrix®. Indications: Active immunization against Hepatitis A for high-risk groups. Dose: By IM injection, 0.5ml single dose with a booster 6-12 months later. Side effects: Headache, Fever, Malaise, Fatigue, Myalgia, Loss of appetite, Nausea. Contraindications: Severe febrile infections. |
| Anti-D (Rho) Immunoglobulin | Indications: Prevention of antibody formation to Rh-positive blood cells in Rh-negative mothers. Given following any sensitizing episode (birth of Rh+ infant, abortion, miscarriage). Dose: Varies by episode, typically 250-500mcg IM within 72 hours. Side effects: Fever, Nausea, Myalgia, Abdominal pain, Local tenderness and stiffness. Contraindications: Rhesus positive individuals, Isolated IgA deficiency. |
The Uganda National Expanded Programme on Immunization (UNEPI), officially launched in October 1993, was established to address critical challenges in immunization services. These included low immunization coverage, the use of non-potent vaccines, inadequate skills among health workers, limited community participation, and a lack of regular monitoring and evaluation. The re-launch of the program in 1997 marked a significant turning point, leading to great improvements in routine immunization coverage and a reduction in the incidence of Vaccine Preventable Diseases (VPDs) like measles.
The core objectives that guide UNEPI's work are:
- To formulate and update national immunization policy, standards, and guidelines.
- To ensure a consistent and reliable supply of potent and effective vaccines.
- To increase both access to and demand for immunization services from the community.
- To build technical and management capacity for the immunization program at all levels of the health system.
- To continuously monitor disease trends and program performance to guide actions.
To achieve its objectives, UNEPI employs a multi-faceted approach:
- Service Delivery: Providing routine immunization through the national health delivery system, including static (at the facility) and outreach services.
- Logistics: Providing and maintaining an effective cold chain and logistics system at all levels.
- Communication: Improving the communication skills of health workers to effectively engage with parents, leaders, and communities.
- Supervision: Strengthening technical and administrative support supervision to ensure quality.
- Training: Providing technical guidance for both pre-service training of health workers and continuous on-the-job training.
- Partnerships: Strengthening partnerships with other child health programs, NGOs, civil society, religious organizations, and the private sector.
- Advocacy & Social Mobilization: Enhancing public education and community involvement to increase vaccine uptake.
- Injection Safety: Promoting and ensuring safe injection practices and proper waste management.
- Surveillance: Maintaining a robust surveillance system for vaccine-preventable diseases using the Integrated Disease Surveillance and Response (IDSR) approach.
- AEFI Management: Promoting the monitoring, investigation, and management of Adverse Events Following Immunization (AEFI).
- Supplemental Activities: Carrying out mass vaccination campaigns (Supplemental Immunization Activities - SIAs) against targeted diseases as needed.
- Innovation: Adopting internationally recommended approaches like Reaching Every District/Reaching Every Child (RED/REC) and developing strategies to reach hard-to-reach populations.
- Disease Control Goals: Strengthening specific disease control measures, including for measles, maternal and neonatal tetanus elimination, and polio eradication.
- UNEPI: Policy and guideline formulation, strategic planning, resource mobilization, technical support and supervision, capacity building, and national monitoring and evaluation.
- National Medical Stores (NMS): Procurement, storage, and distribution of vaccines, injection materials, and other logistics to the district level.
- Implementation of national policies and plans.
- Forecasting, ordering, and storing vaccines and logistics.
- Distribution of supplies to lower-level health facilities.
- Cold chain maintenance and repair.
- Support supervision and on-the-job training for health facility staff.
- Monitoring performance data (e.g., coverage, dropout rates, vaccine wastage) for action.
- Conducting active surveillance for diseases like Acute Flaccid Paralysis (AFP), Neonatal Tetanus (NNT), and measles.
This is where nurses and midwives play their most direct role.
- Providing daily immunization services (static and outreach).
- Counseling and health-educating parents/caretakers.
- Screening every child visiting the facility for their immunization status to reduce missed opportunities.
- Estimating vaccine needs, ordering, and storing them correctly.
- Maintaining the vaccine refrigerator temperature between +2°C and +8°C and recording it twice daily.
- Monitoring and reporting performance data (coverage, wastage, dropouts).
- Tracking defaulters through home visiting and community engagement.
- Working with community mobilizers like Village Health Teams (VHTs).
- Ensuring safe injection practices and proper disposal of sharps in a safety box.
- Taking children for all scheduled immunizations and ensuring completion.
- Participating in planning for outreach services.
- Mobilizing other parents and community members for immunization.
- Keeping the child's health card safe and presenting it at every health facility visit.
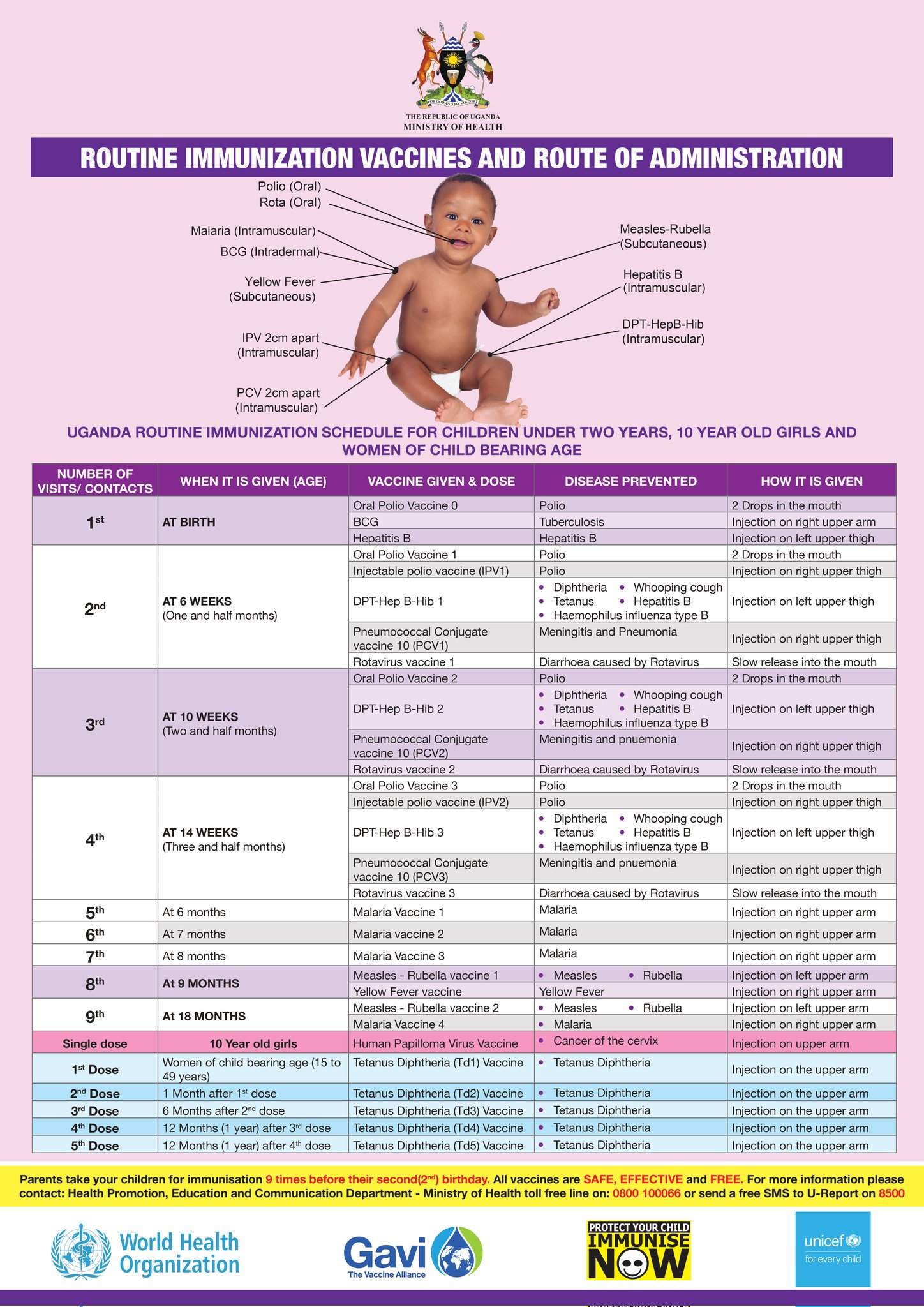
| Visit/Contact | When it is Given (Age) | Vaccine Given & Dose | Disease(s) Prevented | How it is Given (Route and Site) |
|---|---|---|---|---|
| 1st | AT BIRTH (Within 24 hours is best) |
Oral Polio Vaccine 0 (OPV0) | Polio | 2 Drops in the mouth (Oral) |
| BCG | Tuberculosis (severe forms like TB meningitis) | 0.05ml Injection on right upper arm (Intradermal) | ||
| Hepatitis B (Birth Dose) | Hepatitis B (prevents mother-to-child transmission) | Injection on left upper thigh (Intramuscular) | ||
| Injectable Polio Vaccine (IPV1) | Polio | Injection on right upper thigh (Intramuscular) | ||
| 2nd | AT 6 WEEKS (One and a half months) |
Pentavalent 1 (DPT-HepB-Hib 1) | Diphtheria, Pertussis (Whooping cough), Tetanus, Hepatitis B, Haemophilus influenzae type B | Injection on left upper thigh (Intramuscular) |
| Pneumococcal Conjugate Vaccine (PCV1) | Meningitis and Pneumonia (caused by S. pneumoniae) | Injection on right upper thigh (Intramuscular) | ||
| Rotavirus vaccine 1 | Diarrhoea caused by Rotavirus | Slow release into the mouth (Oral) | ||
| Oral Polio Vaccine 2 (OPV2) | Polio | 2 Drops in the mouth (Oral) | ||
| 3rd | AT 10 WEEKS (Two and a half months) |
Pentavalent 2 (DPT-HepB-Hib 2) | Diphtheria, Pertussis, Tetanus, Hepatitis B, Haemophilus influenzae type B | Injection on left upper thigh (Intramuscular) |
| Pneumococcal Conjugate Vaccine (PCV2) | Meningitis and Pneumonia | Injection on right upper thigh (Intramuscular) | ||
| Rotavirus vaccine 2 | Diarrhoea caused by Rotavirus | Slow release into the mouth (Oral) | ||
| Injectable Polio Vaccine (IPV2) | Polio | Injection on right upper thigh (Intramuscular) | ||
| 4th | AT 14 WEEKS (Three and a half months) |
Pentavalent 3 (DPT-HepB-Hib 3) | Diphtheria, Pertussis, Tetanus, Hepatitis B, Haemophilus influenzae type B | Injection on left upper thigh (Intramuscular) |
| Pneumococcal Conjugate Vaccine (PCV3) | Meningitis and Pneumonia | Injection on right upper thigh (Intramuscular) | ||
| Rotavirus vaccine 3 | Diarrhoea caused by Rotavirus | Slow release into the mouth (Oral) | ||
| 5th | At 6 months | Malaria Vaccine 1 | Malaria | Injection on right upper arm (Intramuscular) |
| 6th | At 7 months | Malaria Vaccine 2 | Malaria | Injection on right upper arm (Intramuscular) |
| 7th | At 8 months | Malaria Vaccine 3 | Malaria | Injection on right upper arm (Intramuscular) |
| 8th | AT 9 MONTHS | Measles-Rubella vaccine 1 | Measles, Rubella | Injection on left upper arm (Subcutaneous) |
| Yellow Fever vaccine | Yellow Fever | Injection on right upper arm (Subcutaneous) | ||
| 9th | AT 18 MONTHS | Measles-Rubella vaccine 2 | Measles, Rubella | Injection on left upper arm (Subcutaneous) |
| Malaria Vaccine 4 | Malaria | Injection on right upper arm (Intramuscular) | ||
| Single dose | 10 Year old girls | Human Papilloma Virus (HPV) Vaccine | Cancer of the cervix | Injection on the upper arm (Intramuscular) |
| Dose | When to Give | Vaccine | Disease Prevented | Route and Site |
|---|---|---|---|---|
| Td1 | At first contact or as early as possible in pregnancy | Tetanus Diphtheria (Td) Vaccine | Tetanus, Diphtheria in the mother; Prevents Neonatal Tetanus in the baby | Injection on the upper arm (Intramuscular) |
| Td2 | At least 1 month after Td1 | |||
| Td3 | At least 6 months after Td2 | |||
| Td4 | At least 1 year after Td3 | |||
| Td5 | At least 1 year after Td4 |
BCG (Bacillus Calmette-Guérin) Vaccine: This is a live attenuated (weakened) bacterial vaccine. It is used in the immunization program to protect the child against tuberculosis. BCG is given in a single dose at birth or first contact. The vaccine is very sensitive to light and loses much of its potency when exposed to light. It is given by injecting the child in the skin (intradermally) at the right upper arm. The amount of 0.05 ml is recommended for children up to eleven (11) months of age, and 0.1 ml for children after eleven years.
Polio Vaccine: Polio vaccine is a live attenuated virus vaccine used in the immunization program to protect the child against poliomyelitis. The Sabin type is given orally (by mouth) in Uganda. Some countries use another type called Salk vaccine, which is given by injection. Oral polio vaccine is given four times beginning: at birth (polio 0); at 6 weeks polio 1; at 10 weeks polio 2, and at 14 weeks polio 3 respectively. 2 drops in the mouth are recommended for each dose. It should be noted that booster doses are sometimes given to all children below five years of age in the entire country regardless of immunization status. This is done during national immunization days (NIDs), whose primary objective is to eradicate poliomyelitis. It is nice to remember that polio vaccine is made up of three polio viruses, and the oral polio vaccine is given four times to enable each of three viruses to stimulate the production of antibodies.
Pentavalent Vaccine: Pentavalent vaccine has 5 vaccines which include DPT and Hep.b & Hib. The DPT vaccine is commonly referred to as a triple vaccine because it is used to prevent three diseases, namely diphtheria, pertussis, and tetanus. The diphtheria and tetanus parts of the vaccine are made from the respective toxins, while the pertussis vaccine is made of killed bacterial antigen. It has become necessary to add hepatitis B and haemophylus influenza type b vaccines to DPT to form what is now known as the Pentavalent vaccine (five vaccines). These are given three times because they do not stimulate the body to produce antibodies as well as the live attenuated vaccines. When the second and the third dose are given, the body’s memory of the earlier dose quickly leads to the production of more antibodies. The Pentavalent vaccine is given by injecting the child intramuscularly (in the muscle) at the left upper thigh. It is given three times beginning: at 6 weeks, at 10 weeks, and at 14 weeks, respectively. A dose of 0.5 ml is recommended each time given.
Tetanus Toxoid Vaccine: This is a toxoid vaccine used in the immunization program to prevent children against neonatal tetanus. UNEPI targets all women of childbearing age (15-49 years) and pregnant mothers for tetanus toxoid (TT) vaccination. It is better and safe to give two doses of TT vaccine to any pregnant woman if you are not sure she has had TT in a previous pregnancy. The aim is to use the TT vaccine to provide passive immunity for unborn babies, through the transfer of the mother’s antibodies. This type of immunity reduces with time and is normally boosted by giving the child Pentavalent vaccines at 6 weeks after birth.
Pneumococcal Conjugate Vaccine (PCV 10): PCV 10 consists of sugars (polysaccharides) from the capsule of the bacterium streptococcus pneumonia, which are conjugated to a carrier protein. The PCV 10 contains serotypes 1, 4, 5, 6B, 7F, 9V, 14, 18C, 19F, and 23F. It is highly effective and protects children younger than 2 years of age against severe forms of pneumococcal disease, such as meningitis, pneumonia, and bacteremia. It will not protect against these conditions if they are caused by agents other than pneumococcus or pneumococcal serotypes not present in the vaccine. The World Health Organization and Ministry of Health recommend that infants be given three doses of PCV vaccine, at 6 weeks, 10 weeks, and 14 weeks. PCV should be integrated with DPT-HepB-Hib vaccination.
Rotavirus Vaccine: Rotavirus vaccine is a vaccine used to protect against rotavirus infections. These viruses are the leading cause of severe diarrhea among young children. The vaccines are safe. This includes their use in people with HIV/AIDS. The vaccines are made from weakened rotavirus. The World Health Organization recommends the first dose of vaccine be given right after 6 weeks of age. Two or three doses more than a month apart should be given, depending on the vaccine administered. The vaccine is not recommended for use in children over two years of age.
Malaria Vaccine (RTS,S/AS01): The malaria vaccine, known by its brand name Mosquirix™, is a landmark achievement in public health. It is a recombinant protein-based vaccine that targets the Plasmodium falciparum parasite, the most deadly species causing malaria in Africa. It works by preventing the parasite from infecting the liver and maturing, thus stopping the disease before it can cause symptoms. It is given in a four-dose schedule starting at 6 months of age, with subsequent doses at 7, 8, and 18 months. It is administered as an intramuscular injection in the upper arm.
Human Papillomavirus (HPV) Vaccine: The HPV vaccine is a crucial tool for cancer prevention. It is a recombinant vaccine that protects against specific high-risk types of HPV that are responsible for the vast majority of cervical cancer cases. In Uganda, it is targeted at 10-year-old girls before they are likely to be exposed to the virus through sexual activity. Providing the vaccine at this age ensures the strongest possible immune response. It is administered as an injection in the upper arm.
Immunization coverage should be high to reduce disease transmission. As health workers, we should aim to achieve immunization coverage of over 80%. All children should be immunized at every opportunity. There is no contraindication for immunization. If immunization is done daily, this improves immunization coverage.
Children with minor illnesses should be immunized. The misconception that sick children should not be immunized should be discarded. Very sick children admitted to the hospital should be immunized on discharge. Malnourished children should also be immunized. The danger of vaccine of any given type to the malnourished child is much less than the infection itself.
For children with HIV/AIDS, BCG can spread rapidly and thus should be treated as an opportunistic infection.
Vaccines used in the immunization program are in different forms. Some vaccines are in powder form and must be dissolved in the diluent supplied with them, while others come in liquid form and will not need a diluent. There is a need to prepare the vaccine before immunization.
- Preparing Polio Vaccine: To prepare this vaccine the following should be done: If a dropper is separate, attach it securely to the vial (bottle). Keep polio vaccine shaded from sunlight during the immunization session. Place the vial on a frozen icepack or place it in the sponge hole placed at the mouth of the vaccine carrier, which is provided for this purpose to maintain the temperature.
- Preparing BCG and Measles Vaccines: The following should be done: Use the diluent provided for each vaccine. The diluent should be cold, +4°C – +8°C. Use different 9 ml syringes for mixing measles and BCG vaccines. Draw up the full required amount of the diluent provided as per instruction on the vial. Draw and expel mixture back into the bottle three times or until the vaccine is mixed. Do not shake the vial. BCG and measles vaccines should be placed on a frozen icepack or use the sponge in the vaccine carrier for maintaining the correct temperature. Draw 0.5 ml of measles vaccine (recommended dosage). Draw 0.05 ml of BCG vaccine for babies up to 11 months old and 0.1 ml for babies above 11 months of age (recommended dose).
- Preparing DPT and TT: DPT and TT come in liquid form. You will not need to dissolve or mix them. Remove the metal top from the vial. Draw 0.5 ml into the sterile syringe. Remove bubbles. Keep the vaccine shaded from the light.
- Preparing PCV 10: Ensure availability of a clean vaccine carrier and a sponge. The vaccine carrier should be able to close tightly. Condition icepacks prior to packing vaccines in a vaccine carrier to prevent freezing of PCV, TT, and DPT-Hep B-Hib. On a table with a plastic sheet: – Vaccines, diluent, and droppers – Thermometer – Cotton swab in a clean container – Clean water in a clean container for cleaning injection sites – A tin of vitamin A and a pair of scissors – AD syringe and needles – Child health cards – Child register.
- Never take two vials of the same vaccine out of the vaccine carrier at the same time.
- Do not mix vaccines until mothers and children are present.
- Mix one vial of a particular vaccine at a time.
- Keep opened vials of polio, measles, and BCG vaccines on a frozen icepack or use the sponge in the vaccine carrier. Their temperature must be carefully maintained.
- Do not keep vials of DPT and TT vaccines directly on the frozen icepack.
- Open the vaccine carrier when necessary.
- NEVER SHAKE VACCINE VIALS!!!
After preparing vaccines, the next step is to administer them. Before administering vaccines, you should always remember the following important points:
- Use one sterile syringe and needle per vaccine (antigen) per child or mother.
- Avoid holding loaded syringes in your hand for long to avoid exposing the vaccine to heat or direct sunlight.
- Inform each parent what type of vaccine you are giving the child, the possible reactions to it, what to do about the reactions, and when to bring the child back for more immunization.
- Listen to parents and encourage questions.
- Remove any child’s clothes that are in your way when vaccinating.
- During immunization, ask the mother to hold the child firmly to restrict their movement during immunization.
- Administer the vaccine.
- Give specific health information about each vaccine.
- Clean the skin with cotton wool soaked in clean water and let it dry.
- Hold the middle of the child’s upper right arm firmly with your left hand.
- Hold the syringe by the barrel with the millimeter scale upward and the needle pointing in the direction of the child’s shoulder. Do not touch the plunger.
- Point the needle against the skin, barrel turned up about 3 cm above the thumb. Gently insert its tip into the upper layer of the skin (intradermally).
- Make sure that the needle is in the skin (intradermally) and not under the skin. If the needle goes under the skin, take it out and insert it again. If you bend the needle, replace it with another sterile one.
- Holding the barrel with your index and middle finger, put your thumb on the plunger.
- Holding the syringe flat (parallel to the surface of the skin), inject the vaccine intradermally.
- If the vaccine is injected correctly into the skin, a wheal, with the surface pitted like an orange peel, will appear at the injection site. An indication that the vaccine has been injected incorrectly is that the plunger will move much more easily when the needle is injected under the skin than when it is injected in the skin. If there is no local reaction, re-immunize the child.
- Give the mother health information about BCG, i.e., in 7-9 days, a small sore will appear at the site where the injection was given. The sore might ooze a bit and will last for 6-8 weeks. Keep the baby’s arm clean with soap and water. Do not put dressing or medicine on the sore. The sore will not hurt and it will heal by itself.
- Change the syringe and needle after each vaccine and each child.
- Fill in the immunization tally sheet in the BCG section.
- Administer the next vaccine.
- Ask the mother to hold the child across her laps so that the front of the child’s thigh is facing upwards. Then ask her to hold the child’s legs from moving.
- Clean the site to be injected with a cotton swab moistened in clean water and let it dry.
- Place your thumb and index finger on each side of the place you intend to inject. Stretch the skin slightly.
- Quickly push the needle deeply into the muscle (intramuscular). Pull the plunger back; if there is blood in the syringe, withdraw the needle and discard the vaccine. Obtain a sterile syringe with a needle and new vaccine.
- If no blood appears in the syringe, inject 0.5 ml of vaccine.
- Withdraw the needle.
- Rub the injection spot quickly with a clean piece of cotton swab.
- Give health advice about DPT. Tell the mother that: DPT may cause some tenderness at the site which will go away after a few days, and may cause fever but it will subside in 24 hours.
- Fill the immunization tally sheet appropriately.
- Use another needle and syringe to vaccinate another child.
- Explain to the mother that the child is going to be given two types of vaccines in the form of injections. One will be given in the right and the other in the left thigh.
- Explain to the parent the disease prevented by the vaccine, the number of doses in order to achieve the protection, and reassure her that there is no danger in giving two injections in one visit.
- Explain to the mother the likely side effects and how to manage them, then wash hands with soap and water, drip dry.
- Open the vaccine carrier and pick one vial of PCV and quickly check the expiry date and status of the vial.
- Observe the vial content for unusual appearance and particles. If either is observed, the vial must be discarded.
- Shake the vaccine vial gently to obtain a uniform solution.
- Draw 0.5 ml of the vaccine from the vial using an AD syringe and return the partially used vial in a sponge in a vaccine carrier.
- Instruct the mother on how to hold the child for vaccine administration.
- Clean the right upper outer thigh with a swab soaked in water and administer the vaccine intramuscularly.
- Press the injection site firmly for a few seconds. Do not massage.
- Dispose of the used syringe and needle immediately into the safety box. Do not put swabs in the safety box. Do not recap the needle.
- If a vial is opened for one child and another child is not immediately available to be vaccinated with the remaining vaccine dose in the vial, write on the vial the time it was opened and ensure that the vial is kept cool in the sponge pad and away from any potential contamination for 6 hours.
- Ask the child’s mother whether the child has diarrhea. If yes, note this on the child’s card and tell the mother that this dose of polio needs to be repeated after one month. This child with diarrhea should have a total of 4-9 doses of polio vaccine depending on whether the child got polio 0 or not.
- Use the dropper or device supplied with the vaccine.
- If the child will not open the mouth, gently squeeze his/her cheeks to open his mouth.
- Put 2 drops of vaccine on the child’s tongue.
- Fill in the immunization tally sheet appropriately.
- Note that every child below 5 years of age should receive an extra 2 doses of oral polio vaccine (OPV) each year during national immunization days (NIDs), whether she/he was immunized before or not.
- Use a sterile syringe and needle for each injection. Draw 0.5 ml dose of mixed measles vaccine.
- Ask the mother to expose the child’s left outer upper arm and hold the child firmly to restrict their movement.
- Clean the injection site with a cotton swab soaked in clean water and let it dry.
- With the fingers of one hand, pinch the skin on the outer side of the upper arm.
- Hold the syringe at an acute angle to the child’s arm. Inject the vaccine subcutaneously.
- To avoid injecting the vaccine into a vein, withdraw the plunger slightly before injecting the vaccine. Never give the vaccine if blood is seen in the syringe.
- Press the plunger gently, inject 0.5 ml of vaccine.
- Withdraw the needle. If a drop of blood appears at the injection site, ask the mother to wipe it away with a piece of cotton wool.
- If blood is drawn back in the syringe, the vaccine should not be given. Use another needle and syringe to obtain new vaccine.
- Record the immunization in the immunization tally sheet.
- Pregnant mothers should be given two doses of TT vaccine (0.5 ml) a month apart. However, if it is not possible to establish whether the mother had previously been immunized with TT or whether the mother was a default from a previous dose, two doses should be given a month apart.
- Use a sterile syringe and needle for each injection.
- Clean the thigh with cotton wool moistened in clean water.
- Hold the thigh muscle between your thumb and forefinger.
- With your other hand, inject the vaccine intramuscularly.
- Withdraw the needle.
- Discard the needle and syringe into a safety box. Ensure you do not put swabs in the safety box. Safety boxes are collected and burned.
- Fill the immunization tally sheet.
A well-prepared immunization session requires specific equipment to ensure vaccines are kept potent and administered safely.
- Vaccine Carrier with Conditioned Ice Packs: A portable, insulated container to maintain the cold chain during an immunization session.
- Foam Pad/Sponge: A slotted sponge placed in the top of the vaccine carrier to hold opened multi-dose vials and protect them from heat and direct sunlight.
- Vaccines and their specific Diluents: The correct vaccines and diluents for the session.
- Syringes and Needles: Including single-use Auto-Disable (AD) syringes and separate mixing syringes.
- Safety Box (Sharps Container): A puncture-proof container for the immediate and safe disposal of used needles and syringes.
- Cleaning Supplies: Cotton swabs and a bottle of clean water for cleaning injection sites.
- Documentation Tools: Child health cards, immunization register, and tally sheets.
- Supplemental Supplies: Vitamin A capsules and a pair of scissors to open the blister packs.
- Cold Boxes and Ice Packs: Larger insulated containers used for transporting vaccines from a district store to a health facility.
Communication with the parent or caregiver after vaccination is a critical nursing role. It builds trust and ensures proper follow-up care.
- Reassure parents of the vaccine's safety and explain the common, minor side effects, such as swelling and redness at the injection site, slight fever, or soreness.
- Advise parents on how to manage these side effects (e.g., giving paracetamol for fever).
- Offer integrated health education on topics like nutrition, hygiene, and the importance of breastfeeding.
- Always ask mothers if they have any concerns and take the time to answer their questions respectfully.
- Clearly inform the mother about the date of the next visit required for immunization.
- Administer Vitamin A supplementation to children according to the national schedule (e.g., at 6 months and 12-59 months). If a child receives their first measles dose at 6 months, inform the mother the second dose is due at 18 months.
Accurate record keeping is mandatory for the immunization program. All vaccines administered must be recorded in tally sheets and registers to monitor performance, check a child's immunization status, calculate coverage rates, and plan for future needs.
- The register must be clearly labeled with the name of the health facility.
- It should include the names of the children (not parents), their date of birth, and their medical file/card number.
- For each vaccine (BCG, Polio, Pentavalent, Measles, etc.), enter the date the dose was given. If a dose was missed or not given, it should be clearly indicated, often with a zero (0).
- Note: Supplemental doses like extra OPV or Vitamin A given during campaigns are typically recorded on the child's health card, not in the main immunization register.
- Each child must have their own health card.
- The card must contain essential identifying information: child’s name, mother’s name, date of birth, village, and the primary health unit.
- It serves as the child's personal record of all vaccines received, including dates. Other health information, like Vitamin A administration, is also recorded here.
- Always ensure the child’s card is up-to-date before administering any vaccine.
The refrigerator is the most critical piece of equipment for storing vaccines at the health facility. It must be properly maintained and kept in good working condition at all times. All refrigerators must be maintained at a temperature between +2°C and +8°C.
- Solar direct drive (SDD) vaccine refrigerator.
- Gas refrigerators (using Kerosene or paraffin).
- Electric vaccine refrigerator.
The refrigerator should also be able to freeze ice packs. These ice packs are used to keep vaccines cool in vaccine carriers during outreach sessions. Ice packs inside a vaccine carrier are referred to as Conditioned Icepacks.
All refrigerators should be serviced and maintained regularly (e.g., every 3 months). During maintenance, the following activities are done:
- The refrigerator is cleaned thoroughly.
- The thermostat setting is checked for accuracy.
- The defrosting system is checked.
- The cooling system and compressor are checked and cleaned.
- The electrical connection or gas/kerosene system is checked.
An AEFI is any untoward medical occurrence which follows immunization and does not necessarily have a causal relationship with the use of the vaccine. It is important to respond appropriately to any AEFI.
- Fever: Advise parents to give the child paracetamol (acetaminophen) in the correct dose for their weight. Do not give aspirin to children. Encourage plenty of fluids.
- Swelling or Redness at the Site of Injection: This is usually a normal, mild reaction. Reassure the parent it will go away on its own. Do not give any drug or apply any substance to the site.
- Swelling of the Limbs or Face, or Difficulty in Breathing: This is a sign of a potential severe allergic reaction and is a medical emergency. Do not give any drug. Advise the parent to seek medical attention at the nearest health facility immediately.
- Loss of Weight, Generalized Body Swelling, Poor Feeding, or Coughing: These are unlikely to be side effects of vaccination and are more likely symptoms of an underlying condition like malnutrition or another illness. Refer the child to the health facility for assessment and treatment.
- Diarrhea: This is most likely not related to vaccination. Ensure the child receives oral rehydration solution (ORS) or other appropriate fluids to prevent dehydration.
Mass vaccination campaigns, such as National Immunization Days (NIDs) or outbreak responses, require careful planning and execution.
- Planning and Training: Plan the campaign, identify target populations, and train healthcare workers on all procedures.
- Community Mobilization: Inform communities well in advance about the campaign's purpose, date, and location.
- Logistics: Ensure all necessary equipment (vaccines, syringes, safety boxes, cold chain equipment) is in place.
- Safety Measures: Implement infection control, safe waste disposal, and crowd control measures at vaccination sites.
- Vaccination Site Setup: Organize sites for an efficient flow of people from registration to vaccination to a post-vaccination observation area.
- Vaccine Administration: Follow standard procedures, ensuring one sterile syringe and needle per injection.
- Monitoring and Reporting: Monitor the campaign’s progress, track doses administered, and ensure AEFIs are reported and managed promptly.
- Documentation: Maintain detailed records of all vaccines administered, including tallies and vaccine wastage.
- Post-Campaign Evaluation: Evaluate the campaign’s success and identify areas for improvement.
- Follow-Up: After the campaign, ensure routine immunization services continue and that children receive follow-up doses as needed.
Very informative
Enjoyable
Polio is divided into two, OPV and IPV
so OPV is a live attenuated vaccine while IPV is inactivated polio vaccine.
And both are given together at 14weeks.
Where does polio vaccine fall
Live attenuated or dead