

Role of Ophthalmic Nurses
- Provide first aid treatment in cases of eye injuries and emergencies.
- Perform preliminary physical examinations, such as blood tests, to detect possible underlying illnesses that could contribute to eye problems (e.g., hypertension).
- Conduct initial screenings on patients.
- Collect medical histories.
- Assist in eye examinations.
- Offer tips and advice to help patients manage eye pain and other symptoms.
- Demonstrate how to administer medication.
- Educate patients on the treatment of ocular conditions.
- Prepare patients for surgery and assist during operations.
- Provide after-surgery care for patients.
- Conduct various eye tests and procedures.

Ophthalmic Emergencies and Urgent Cases
Emergencies requiring immediate medical attention include:
Sudden vision loss:
- Central retinal artery occlusion: Blockage of the artery supplying the central retina.
- Central retinal vein occlusion: Blockage of the vein draining blood from the retina.
- Giant cell arteritis: Inflammation of the arteries in the head, including those supplying the eye.
- Retinal detachment: Separation of the retina from the back of the eye, especially if the macula (central part of the retina) is still attached.
Primary acute glaucoma: Rapid increase in pressure within the eye, causing pain, blurred vision, and halos around lights.
Trauma:
- Penetrating or perforating injuries: Objects entering the eye.
- Chemical burns: Exposure of the eye to chemicals.
Orbital cellulitis: Infection of the tissues surrounding the eye.
Urgent cases requiring prompt medical attention, but not considered true emergencies:
- Corneal ulcer: Open sore on the cornea, causing pain, redness, and blurred vision.
- Vitreous hemorrhage: Bleeding into the vitreous humor (jelly-like substance filling the back of the eye), causing blurred vision or floaters.
- Acute dacryocystitis: Inflammation of the lacrimal sac (tear sac), causing pain, swelling, and redness.
- Optic nerve disorders: Conditions affecting the optic nerve, causing vision loss or other visual disturbances.
- Ocular tumors: Growths within the eye, which may affect vision or require treatment.
- Acute uveitis: Inflammation of the middle layer of the eye, causing pain, redness, and blurred vision.




Common charts used in the measurement of distance visual acuity
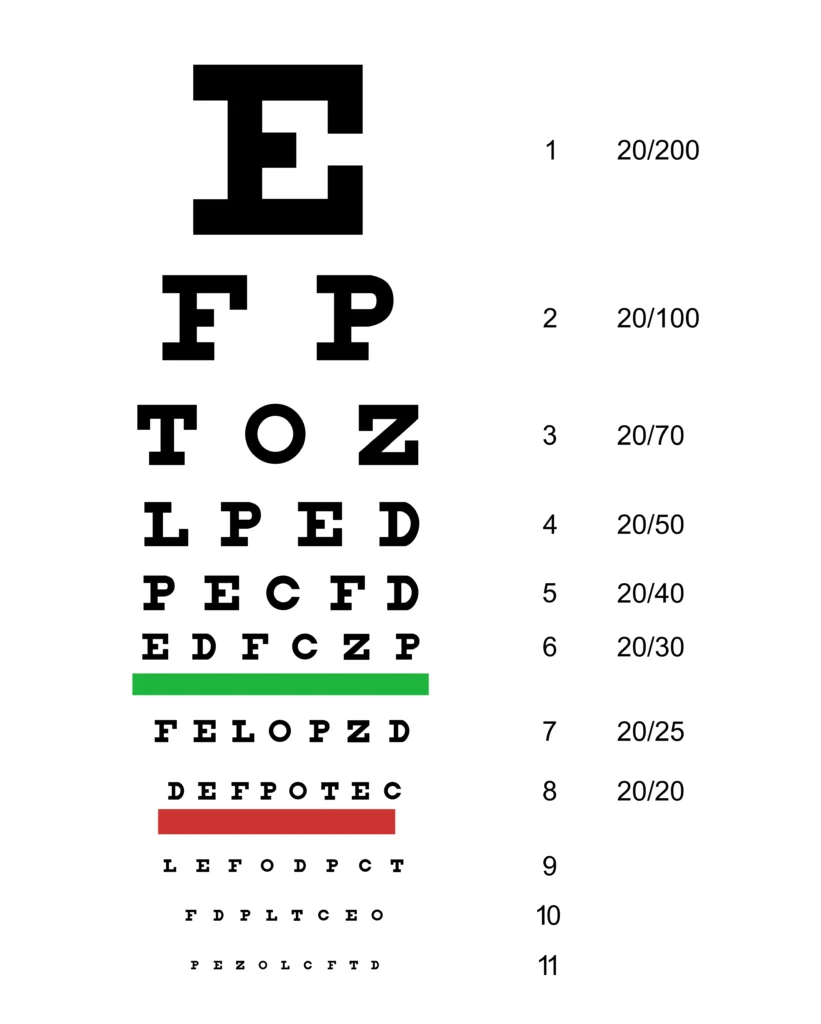
The most common chart for measuring distance visual acuity in a literate adult is the Snellen chart. Distance vision is tested at 6 meters, as rays of light from this distance are nearly parallel. If the patient wears glasses constantly, vision may be recorded with and without glasses, but this must be noted on the record. Each eye is tested and recorded separately, the other being covered with a card held by the examiner.
Snellen’s Chart
Heavy block letters, numbers, or symbols printed in black on a white background are arranged on a chart in nine rows of graded size, diminishing from the top downwards. The top letter can be read by the normal eye at a distance of 60 meters, and the following rows should be read at 36, 24, 18, 12, 9, 6, 5, and 4 meters, respectively.
Procedure:
- One eye is tested at a time, with the other eye covered.
- The patient reads lines of letters, starting from the top and working down.
- The smallest line the patient can read correctly indicates their visual acuity.
Recording: Visual acuity is recorded as a fraction (e.g., 20/20, 6/6), where the numerator represents the distance at which the patient can read the line and the denominator represents the distance at which a person with normal vision can read that same line.
Using the pinhole in the measurement of visual acuity
Occasionally, a patient’s visual acuity may be below average, which could be a result of a refractive error not corrected by glasses, or due to the patient wearing an old pair of prescription glasses. One effective, but very simple, way to see if distance visual acuity can be improved through spectacles or a change of prescription is a pinhole. A pinhole disc only allows central rays of light to fall onto the macula and does not need to be refracted by the cornea or lens. A ‘pinhole disc’ is used if the VA is less than 6/6 or 6/9, which may improve VA. If a considerable increase in vision is obtained, it may usually be assumed that there is no gross abnormality, but rather a refractive error.

- Purpose: Used when visual acuity is below average, to determine if the problem is refractive error (uncorrected by glasses) or another condition.
- Method: A pinhole disc restricts light to pass through a small opening, improving focus and reducing blur caused by refractive errors.
- Interpretation:
- If visual acuity significantly improves with the pinhole, it suggests a refractive error.
- If visual acuity does not improve, it may indicate another underlying eye condition.
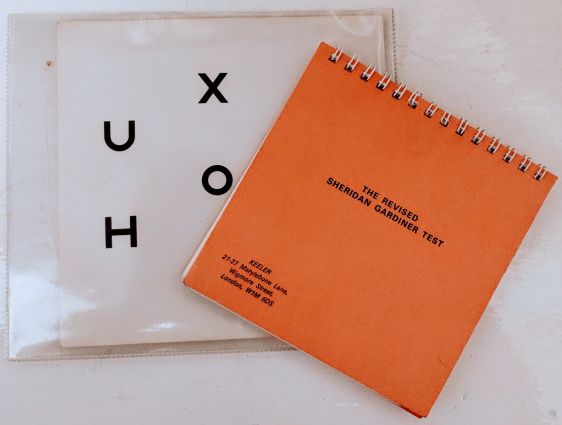
Sheridan Gardner Test Chart
The Sheridan Gardner test chart can be used for children and patients who are illiterate. This test type has a single reversible letter on each line. For example, A, V, N. The child holds the card with these letters printed on and is asked to point to the letter on his card which corresponds to the letter on the test type. This test can also be used for very young children as they do not have to name a letter.
Procedure:
- The patient holds a card with the same letters printed on it.
- The examiner points to a letter on the chart.
- The patient points to the corresponding letter on their card.
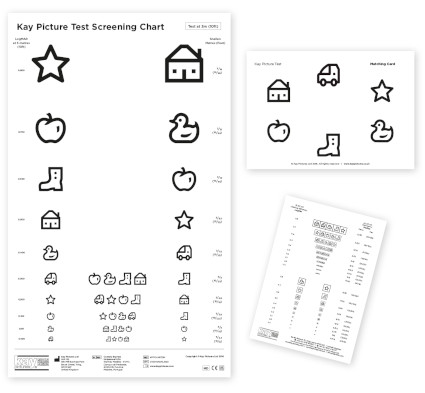
Kay Picture Chart
The Kay picture chart is again used with patients who are illiterate or with children. Instead of letters, the book contains pictures, which are also of varying sizes. The patient is asked what the picture represents. In order to avoid any misunderstanding amongst patients with language difficulties, it is good practice to ask the hospital’s official interpreter to translate for patients.
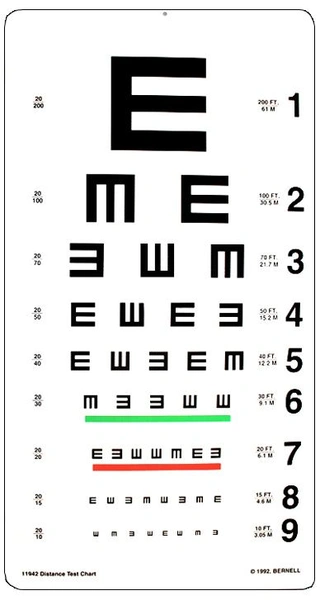
Tumbling E chart
The tumbling E chart is mainly used for patients who are illiterate. In the chart, the Es face in different directions. The patient is asked to hold a wooden E in his hand and to turn it the same way as the one the examiner is pointing to on the test chart.
Procedure:
- The patient holds a wooden “E”.
- The examiner points to an “E” on the chart.
- The patient rotates their wooden “E” to match the orientation of the “E” on the chart.

The content adds knowledge
Appreciate your efforts
Thanks.
Well elaborated keep it up
This is a very helpful Note, thanks so much.. however, different surgeries have their different nursing care, I feel would be good if explained according to a specific surgery
A great Job…. thanks