
Organophosphates Poisoning is a serious medical emergency that occurs when a person develops an illness as a result of exposure to organophosphates (OPs). Organophosphates are chemicals extensively used in agriculture as insecticides. When humans—particularly agricultural workers—are exposed to large quantities, these chemicals can be severely harmful or fatal.
- Other Uses: They are also used as nerve agents in chemical warfare (e.g., Sarin gas, Soman, Tabun, VX) and occasionally as therapeutic agents (e.g., ecothiopate for glaucoma).
- Global Impact: There are no rules and regulations governing the purchase of these products in many regions, making them readily available "over the counter." This leads to an estimated 3 million exposures and 300,000 mortalities globally each year.
- Exposure Context: Exposure in an attempt to commit suicide is a key problem, particularly in developing countries, and is a more common cause of severe poisoning than the chronic exposure experienced by farmers or sprayers.
- Poison: A foreign chemical that is capable of producing a harmful effect on a biologic system (xenobiotic).
- Poisoning: The development of harmful effects on normal body functions following exposure to chemicals after it is swallowed, inhaled, injected, or absorbed cutaneously.
There are more than a hundred organophosphorus compounds in common use, classified according to their toxicity and clinical use:
| Toxicity Level | Common Examples | Primary Use |
|---|---|---|
| 1. Highly Toxic | Tetra-ethyl pyrophosphates (TEPP), Parathion | Agricultural insecticides |
| 2. Intermediately Toxic | Coumaphos, Chlorpyrifos, Trichlorfon | Animal insecticides, antihelminthic agents |
| 3. Low Toxicity | Diazinon, Malathion, Dichlorvos | Household applications and field sprays |
- Parathion
- Fenthion
- Malathion
- Diazinon
- Dursban
- Quinalphos
- Prothoate
- Nearly 25 million cases of unintentional pesticide poisoning occur in the agricultural industry across the world each year.
- Globally, it is reported that 3 million or more people are exposed to OPs every year, accounting for approximately 300,000 mortalities.
- In the United States, there are around 8,000 exposures per year, with fewer deaths.
- Poisoning leads to significant morbidity and mortality each year in India. According to the National Crime Records Bureau of India, there were 27,657 deaths and suicides by poisoning in 2015.
- Cases are most common in regions where workers do not use or do not have access to protective gear, such as specialized suits or masks.
- Symptoms and complications vary wildly but can quickly escalate to death.
Organophosphates exert their acute toxic effects by causing massive overstimulation at cholinergic nerve terminals.
- Normal Function: Acetylcholine (ACh) is a vital neurotransmitter found in the central and peripheral nervous systems, neuromuscular junctions, and red blood cells (RBCs). Normally, the enzyme acetylcholinesterase (AChE) catalyzes the rapid degradation of ACh into choline and acetic acid in the nerve synapse, ending the nerve signal.
- The Toxic Mechanism: OP pesticides act by binding irreversibly to the AChE enzyme.
- The Consequence: This binding severely reduces the ability of the enzyme to break down the neurotransmitter. This produces a massive, uncontrolled accumulation of ACh in the central and peripheral nervous systems.
- The Result: This accumulation results in an acute cholinergic syndrome via continuous, unrelenting neurotransmission.
The clinical onset of cholinergic overstimulation can vary from almost instantaneous to several hours after exposure. Although most patients rapidly become symptomatic, the onset and severity of symptoms depend heavily on the specific compound, the amount, the route of exposure, and the rate of metabolic degradation in the patient's body.
- Ingestion: Through the Gastrointestinal (GI) tract (can be accidental or deliberate/suicidal).
- Cutaneous: Absorption directly through the skin (common in occupational exposure).
- Inhalation: Absorption through the lungs.

The length and strength of the exposure will determine the nature of the symptoms, which can range from mild to severe emergency-level toxicity.
- Blurry or impaired vision, watery/stinging eyes, narrowed pupils
- Nausea
- Runny nose, extra saliva
- Headache
- Muscle fatigue, weakness, or minor twitching
- Agitation and glassy eyes
- Dizziness, disorientation
- Very narrow pupils (miosis)
- Muscle tremors, pronounced twitching, and weakness
- Drooling, excessive phlegm
- Wheezing, coughing, and difficulty breathing
- Severe vomiting and severe diarrhea
- Sneezing and uncontrolled urination or bowel movements
- Extreme confusion or Coma
- Pinpoint narrow pupils
- Convulsions / Seizures
- Agitation
- Massive, excessive secretions (saliva, sweat, tears, mucus)
- Irregular or slow heartbeat (bradycardia)
- Collapsing
- Breathing that becomes ineffective or stops completely (respiratory arrest)
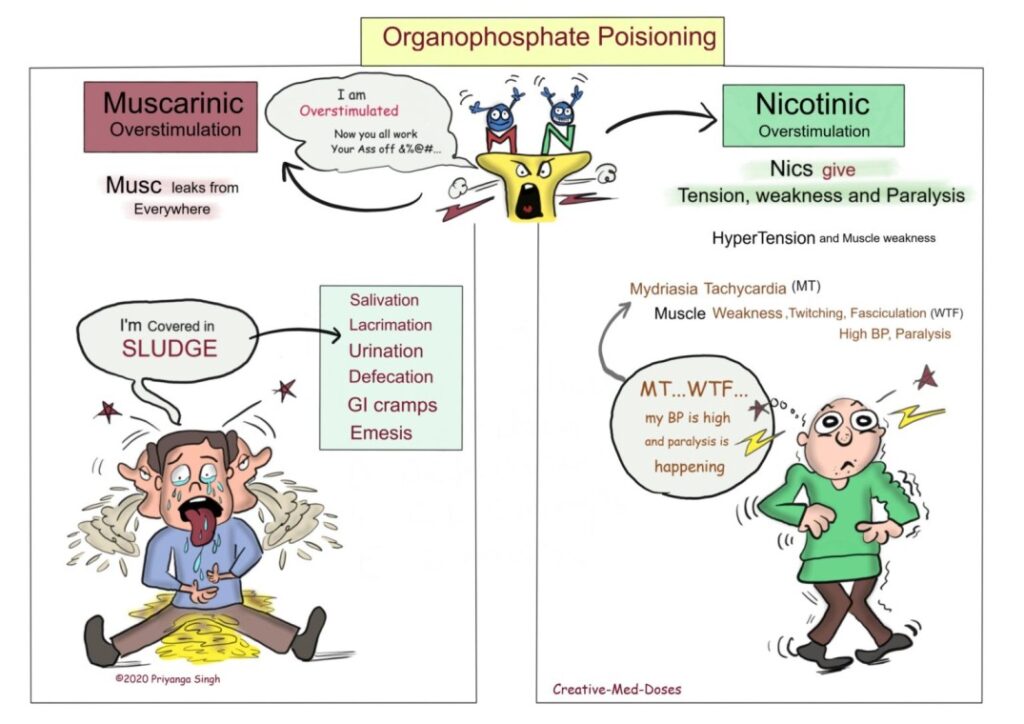
The accumulation of acetylcholine overstimulates two main types of receptors: Muscarinic and Nicotinic.
Muscarinic Signs and Symptoms
"Musc leaks from everywhere" - There are excessive secretions from everywhere in muscarinic overstimulation. Remember the mnemonic SLUDGE:
- S - Salivation
- L - Lacrimation (tears)
- U - Urination
- D - Defecation
- G - GI cramps
- E - Emesis (vomiting)
Nicotinic Signs and Symptoms
"Nics give tension, weakness, and paralysis" - Remember the mnemonic MT WTF:
- M - Mydriasis (Note: while miosis is the classic muscarinic sign, sympathetic override can occasionally cause mydriasis)
- T - Tachycardia
- W - Muscle Weakness
- T - Muscle Twitching
- F - Muscle Fasciculation
- BP is high - Hypertension
- Paralysis is happening - Muscle paralysis
In addition to immediate symptoms, OP exposure can cause long-term complications depending on the extent of exposure:
- Paralysis
- Fertility issues
- Cancer
- Metabolic disorders (e.g., high blood sugar levels)
- Inflammation of the pancreas (Pancreatitis)
- Excess acid in the blood (Acidosis)
- Brain and nerve problems (Organophosphate-induced delayed polyneuropathy - OPIDN)
- History: Determine the type of exposure (occupational, accidental, deliberate ingestion), time of exposure, and specific chemical if known.
- Physical Examination: Look for classic signs (SLUDGE, miosis, garlic-like odor on breath).
- Vital Signs: Depressed respirations, bradycardia, and hypotension are common, life-threatening findings.
- Laboratory Investigations:
- Plasma pseudocholinesterase levels: Normal is 3000–8000 U/L. In poisoning, serum levels may drop to < 1000 U/L.
- RBC AChE level: A more accurate marker of nervous system AChE inhibition.
- White blood cells (WBC): Leucocytosis is frequently seen.
- ABG values: To rule out or confirm metabolic and/or respiratory acidosis.
- Electrolytes: Potassium and magnesium levels are often decreased.
- Imaging Studies:
- Chest X-ray for aspiration pneumonia or pulmonary edema.
- Electrocardiogram (ECG) for ventricular arrhythmias, prolonged QTc, or heart block.
Identify the specific nature of the poison (e.g., OP, carbamate, chloride, pyrethroid) to guide specific antidote therapy.
- Staff Safety: Staff must put on protective equipment before commencing treatment, including masks, gowns, eye protection, and specialized gloves (usually nitrile/rubber, as OPs penetrate latex). Staff involved in direct contact with the patient’s bodily secretions should immediately and thoroughly wash affected areas with soap and water.
- Physical Decontamination: Remove all clothing. Wash the patient thoroughly with soap and copious amounts of water.
- Gastric Decontamination: Gastric lavage should be done only after stabilizing the airway. It is generally given within 1 hour of ingestion. Activated charcoal (0.5–1 g/kg) can be given within 1 hour of ingestion to bind remaining poison in the gut, though some studies show limited benefit. Do not induce emesis.
- Airway: Maintain a clear airway via frequent suctioning of excessive secretions. Check the gag reflex. If absent, intubate before any stomach wash is performed to prevent aspiration.
- Breathing: Administer oxygen at 6 L/min. Intubation and mechanical ventilation are required if breathing is inadequate, oximetry is <90%, or the Glasgow Coma Scale (GCS) is <8.
- Circulation: Administer adequate intravenous (IV) fluids through a wide bore cannula to replace volume loss from severe vomiting and diarrhea.
Continuously monitor for fatal arrhythmias (e.g., ventricular tachycardia, Torsades de pointes) using an ECG.
- Protocol for Atropinisation: Atropinisation must be initiated as soon as the diagnosis is suspected. The aim is to keep the patient's airway dry. Administer Injection Atropine 2 mg IV bolus (or 0.05 mg/kg). The dose is then doubled every 5 minutes until adequate atropinisation is achieved.
- Signs of Atropinisation (Target End-Points):
- Heart rate about 100/min
- Pupils return to mid-position
- Bowel sounds just heard (not hyperactive)
- Clear lung sounds (secretions dry up)
- Dry skin
- Signs of Atropine Toxicity (Anticholinergic Toxidrome): Care must be taken not to over-atropinise. Signs include: Dry mucus membranes ("dry as a bone"), mental status changes/delirium ("mad as a hatter"), flushed skin ("red as a beet"), severe mydriasis ("blind as a bat"), fever ("hot as hell"), severe tachycardia, hypertension, decreased bowel sounds, and urinary retention.
- Treatment for Toxicity: Atropine toxicity is treated with injection haloperidol (5 mg IM or IV) for agitation, and by immediately reducing or pausing the dose of atropine.
- Oximes (e.g., Pralidoxime/PAM): Given to reactivate the AChE enzyme and reverse nicotinic effects (muscle weakness/paralysis). Must be given early before the enzyme "ages."
- Antibiotics: Not usually indicated for OP poisoning itself. However, gastric lavage with an unprotected airway and/or a low GCS creates a massive risk for aspiration. If aspiration pneumonia is suspected (fever, leucocytosis, pulmonary infiltrates), broad-spectrum antibiotics (e.g., Ceftriaxone, Piperacillin/Tazobactam [Piptaz]) are indicated.
- Sedation: Agitation may indicate over-atropinisation, hypoxaemia, or distress. Intubated patients need a combination of an analgesic and a sedative (e.g., morphine + lorazepam infusion). Haloperidol may increase the seizure threshold and is not recommended unless patients are unresponsive to other drugs.
- Diuretics: Lasix (Furosemide) is the drug of choice if pulmonary edema persists even after full atropinisation has been achieved.
| No. | Nursing Responsibility | Clinical Rationale |
|---|---|---|
| A. Airway & Respiratory Management | ||
| 1 | Assess the airway for bilateral equal air entry, respiratory rate, and breath sounds. Check for bronchospasms. | Respiratory failure is the primary cause of death; continuous assessment is vital. |
| 2 | Position the patient in semi-Fowler’s at 45° and change position every 2 hours. | Promotes diaphragmatic descent, maximal lung expansion, mobilizes secretions, and actively prevents aspiration of vomit. |
| 3 | Perform frequent, aggressive airway suctioning whenever necessary. | Bronchorrhea (massive lung secretions) can rapidly occlude the airway. |
| 4 | Assess for cough and gag reflex; assist immediately with intubation if absent. | An absent gag reflex means the patient cannot protect their airway from massive secretions or vomit. |
| 5 | Provide humidification to airways and check ventilator settings closely if mechanically ventilated. | Thins out thick secretions and ensures optimal mechanical oxygenation. |
| B. Hemodynamic & Systemic Monitoring | ||
| 6 | Assess heart rate, rhythm (via ECG) for arrhythmias, BP, capillary refill time, skin turgor, and vital signs every hour. | OP poisoning and Atropine therapy both cause massive, rapidly shifting hemodynamic instability. |
| 7 | Administer IV fluids and Atropine infusions accurately as prescribed. | Fluids combat hypovolemia from GI losses; Atropine must be titrated meticulously to maintain the heart rate above 90/min without causing severe toxicity. |
| 8 | Monitor urine output every hour via a Foley catheter. | Assesses renal perfusion and checks for urinary retention (a sign of atropine toxicity). |
| 9 | Check for neck muscle weakness and the use of accessory muscles for breathing. Assess "single breath count." | These are critical early warning signs of impending nicotinic respiratory muscle paralysis. |
| C. Infection Control & Supportive Care | ||
| 10 | Follow strict aseptic technique while handling invasive lines and performing suctioning. | Prevents secondary healthcare-associated infections in a critically ill patient. |
| 11 | Provide rigorous oral care with chlorhexidine solution. | Prevents Ventilator-Associated Pneumonia (VAP) and manages excessive oral secretions. |
| 12 | Administer prophylactic or therapeutic antibiotics (e.g., Injection Piptaz 4.5 g IV q 8 hourly) as per order. | Treats suspected or confirmed aspiration pneumonia. |
| 13 | Monitor ABG values, WBC counts, culture and sensitivity results, and chest X-rays. | Provides objective data on respiratory acidosis, infection status, and pulmonary edema. |
| 14 | Evaluate the patient's feelings and perception of their lack of power; involve them in care when conscious. | Addresses the severe psychological trauma of a suicide attempt or a terrifying accidental poisoning, promoting mental recovery. |
Good notes I like them