
Structure of a neuron
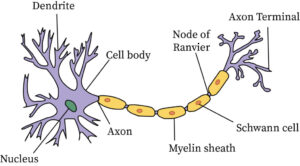
FUNCTIONS OF NEURON STRUCTURES
- Nucleus – controls the entire neuron.
- Dendrite – receives stimulus and carries its impulses toward the cell body.
- Cell Body (soma) – has a nucleus & cytoplasm. It acts as a factory of the neuron. It produces all protein for the dendrites and neurotransmitters.
- Axon – fiber which carries impulses away from the cell body i.e it forms a conduction region for the neuron.
- Schwann Cells/ neurolemmocyte – cells which produce myelin or fat layer in the Peripheral Nervous System (axon maintenance and regeneration) It’s a glial cell that wraps the nerve fibre in PNS.
- Myelin sheath – dense lipid layer which insulates the axon ( makes the axon look gray) It speeds-up nerve transmission.
- Node of Ranvier – gaps or nodes in the myelin sheath. They speed up nerve transmission.
- Axon terminals – form junctions with other cells.
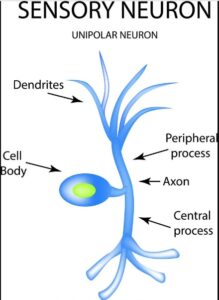
There are three types of Neurons
- Sensory neurons – bring messages to CNS.
- Motor neurons – carry messages from CNS.
- Interneurons – between sensory & motor neurons in the CNS.


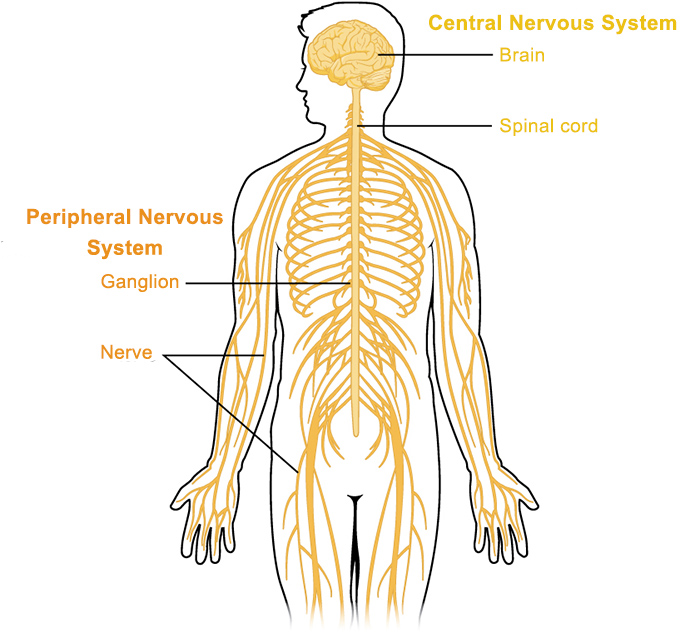
I. Introduction to Cerebrospinal Fluid (CSF)
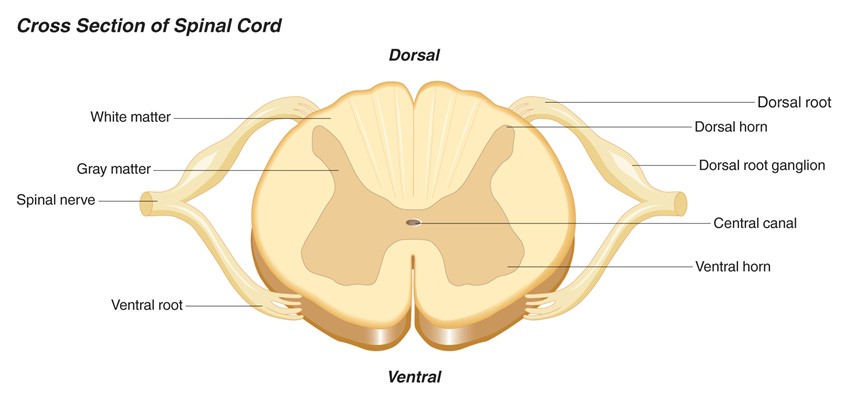
The Cerebrospinal Fluid (CSF) is a clear, colorless, ultrafiltrate of blood plasma that fills the ventricles of the brain, the central canal of the spinal cord, and the subarachnoid space surrounding the entire Central Nervous System (CNS). It serves as the vital “lifeblood” and shock absorber for the brain and spinal cord.
Volume and Production Rate:
- Total Volume: The average adult CNS contains about 130 to 150 mL of CSF at any given time.
- Rate of Production: It is produced at a rate of roughly 20 mL per hour (or about 500 mL per day).
- Physiological Implication: Because 500 mL is produced daily but the system only holds 150 mL, the entire volume of CSF is completely flushed and turned over 3 to 4 times a day! If absorption is blocked, this rapid production quickly leads to hydrocephalus.
Formation of CSF:
- The Choroid Plexus: Approximately 70-80% of CSF is actively secreted by the choroid plexuses (networks of blood capillaries lined by highly specialized ependymal cells) located in the roofs of the lateral, third, and fourth ventricles.
- Blood-CSF Barrier: Unlike normal leaky capillaries, the ependymal cells of the choroid plexus are joined by tight junctions. This forms the Blood-CSF barrier, strictly controlling what substances from the blood are allowed to be actively transported into the CSF.
- The remaining 20-30% of CSF is produced by the ependymal lining of the ventricles and cerebral capillaries.
II. Functions of the CSF
The CSF is not just “water in the brain.” It has four highly specific, life-sustaining functions:
Mechanical Protection (Buoyancy):
- The brain is essentially “floating” in a bath of CSF. According to Archimedes’ principle, this buoyancy reduces the effective weight of the human brain from ~1,400 grams to a mere 50 grams.
- Without CSF, the heavy brain would sink and crush the vital centers in the lower brainstem against the base of the skull, cutting off its own blood supply.
Shock Absorption:
- It acts as a liquid hydraulic cushion. When the head takes a blow, the CSF dissipates the physical force, preventing the delicate brain tissue from violently smashing against the hard inner skull.
Chemical Protection & Homeostasis:
- Optimal neuronal signaling (action potentials) requires a highly stable ionic environment. The CSF provides a strictly regulated, optimized chemical bath for the neurons, free from the wild hormonal and chemical fluctuations of normal blood plasma.
Circulation & Waste Removal (The “Glymphatic” System):
- Because the brain lacks a traditional lymphatic system, the CSF acts as the brain’s waste clearance pathway. It washes away toxic metabolic byproducts (like amyloid-beta plaques) that accumulate during the day. (Interestingly, this flushing mechanism is highly active while we sleep!)
III. The Circulation Pathway of CSF
CSF flows in a strict, one-way path driven by its own continuous production, the pulsating of nearby blood vessels, and the beating of cilia on ependymal cells.
 Mnemonic: The CSF Flow Pathway
Mnemonic: The CSF Flow Pathway
“Love In The Air, For Lovers & Maidens, So Sweet”
- Lateral ventricles
- Interventricular foramina (of Monro)
- Third ventricle
- Aqueduct (Cerebral Aqueduct of Sylvius)
- Fourth ventricle
- Luschka (Lateral foramina) & Magendie (Median foramen)
- Subarachnoid space
- Superior sagittal sinus (Absorption)
Absorption of CSF:
- After circulating through the subarachnoid space, the CSF must be returned to the venous blood to prevent pressure buildup.
- This occurs at the Arachnoid Villi (which clump together to form Arachnoid Granulations).
- These granulations protrude into the dural venous sinuses (primarily the Superior Sagittal Sinus). They act as one-way pressure valves: when CSF pressure is higher than venous pressure, CSF empties into the blood. If venous pressure rises, the valves snap shut to prevent blood from flowing backward into the brain.
IV. Composition of CSF vs. Blood Plasma
A crucial topic for board exams and clinical practice. Normal CSF is crystal clear and looks like water. Because of the Blood-CSF barrier, its composition is very different from blood plasma.
 Points for Attention: Lumbar Puncture (Spinal Tap)
Points for Attention: Lumbar Puncture (Spinal Tap)
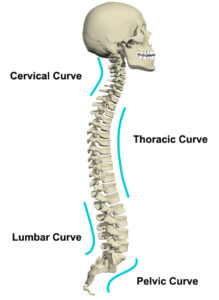
To analyze the composition of CSF, doctors perform a Lumbar Puncture. Because the solid spinal cord ends at the L1/L2 vertebral level in adults, the needle is safely inserted between L3 and L4 (or L4 and L5) into the subarachnoid space (the lumbar cistern). This area contains floating nerve roots (cauda equina) that easily move out of the needle’s way, making it the safest place to draw CSF.
 Applied Clinical Question: Meningitis
Applied Clinical Question: Meningitis
Case: A 19-year-old student presents with a stiff neck, severe headache, high fever, and photophobia (light sensitivity). A lumbar puncture is performed. The CSF drawn is cloudy and turbid. Laboratory analysis reveals a heavily elevated WBC count (mostly neutrophils), massively elevated protein (250 mg/dL), and drastically reduced glucose (15 mg/dL). What is the diagnosis?
Answer: Acute Bacterial Meningitis.
Why? The bacteria are literally “eating” the glucose for energy (causing low CSF glucose). The immune system sends neutrophils to fight the infection (high WBCs), and the inflammation destroys the Blood-Brain Barrier, allowing large blood proteins to leak into the CSF (high protein), turning the fluid cloudy.



Thank you for great work towards our excellence 🤝🤝🤝
You are welcome
Thanks for the great work being to up lift our performance.
Thanks for the good work.
I asking whether unmeb sets questions and review of anatomy and physiology or we just need to remind our selves so that we can understand the medical conditions under the system?
I mean questions on not and
Thanks 👍👍👍😊 pat
Quite interesting but kinder tasky to digest
Thanks so much for the great work of making tasky information easier
I am enjoying my diploma study with a lot of peace
Greatly simplified notes for i in certificate