

The World Health Organization (WHO) states that freedom from cancer pain and pain caused by other diseases like HIV/AIDS should be a basic human right. No person should suffer unnecessarily from pain that can be treated.
In Uganda, where cancer and HIV/AIDS are major causes of illness and death, pain management is one of the most important services nurses can provide. Yet pain remains one of the most undertreated symptoms in our health facilities.
Pain cannot be managed properly without first being assessed. Assessment tells us:
- Where the pain is
- What type of pain it is
- How severe it is
- What is causing it
- What the patient has already tried
Without assessment, treatment is only guessing — and guessing causes suffering.
Pain Assessment CLICK HERE if you haven't read it yet
The WHO has established five fundamental principles that guide all pain management in palliative care. Every nurse must know these by heart.
Pain pathways in the central nervous system (CNS) undergo "wind-up" or central sensitization. If pain is left untreated or allowed to fluctuate wildly, the spinal cord receptors (NMDA receptors) become hyper-reactive. This means it takes exponentially MORE medication to treat pain once it has "broken through" than it takes to prevent it in the first place.
Always give treatment orally when possible.
- The oral route is the safest, most convenient, and most acceptable route for patients.
- Oral medicines can be taken at home without a nurse present.
- Oral morphine is cost-effective compared to injections or tablets.
- Patients prefer oral medicines because they avoid the pain and fear of injections.
- If the patient is vomiting severely.
- If the patient is unconscious and cannot swallow.
- If the patient has a bowel obstruction.
- In these cases, use rectal, subcutaneous, buccal (inside the cheek), or intravenous routes.
Nursing tip: Even unconscious patients can absorb small amounts of oral morphine through the mucosa of the mouth (buccal) or rectum. (Physiology: Buccal and rectal routes bypass the hepatic first-pass metabolism, allowing the drug to enter the systemic circulation directly via the capillary beds).
Persistent pain requires regular, round-the-clock dosing.
- Give analgesics at fixed, regular intervals — not just when the patient asks.
- Give the next dose before the previous one has worn off.
- For oral morphine, this means every 4 hours (6 doses per day).
- Do not wait for the patient to complain of pain. By the time they complain, the pain has already returned and is harder to control.
- Pain that is allowed to return causes fear, anxiety, and suffering.
- It takes more medicine to relieve pain that has "broken through" than to prevent it.
- Regular dosing keeps a steady level of medicine in the blood. (Maintaining therapeutic plasma concentration).
Nursing tip: Write a clear schedule for the patient and family. For example: "Take morphine at 6am, 10am, 2pm, 6pm, 10pm, and 2am."
Use the WHO analgesic ladder as a guide to management. You can move stepwise up or down the ladder.
The WHO analgesic ladder is a step-by-step system for choosing pain medicines based on pain severity.
- Start at the step that matches the patient's pain level.
- If pain is not controlled, move up to the next step.
- If pain improves, you can move down to a lower step.
- Step 1 drugs can be used with Step 2 and Step 3 drugs.
- BUT: Weak opioids (Step 2) must NEVER be given with strong opioids (Step 3) because they work on the same receptors and do not add benefit. (Physiological reason: They compete for the exact same Mu-opioid receptors. Giving Codeine with Morphine just wastes the Codeine and can even antagonize/block the stronger Morphine's effect!).
Dosage is determined on an individual basis. No two patients are the same.
- The "right dose" is the dose that relieves the patient's pain without causing intolerable side effects.
- There is no standard dose of morphine that fits everyone.
- Factors that affect the dose include:
- Age (elderly need lower starting doses).
- Weight (very thin/cachexic patients need lower doses).
- Kidney function (impaired kidneys cause morphine to build up).
- Previous use of opioids (patients already on codeine may need higher starting doses of morphine).
- Severity and type of pain.
- Psychological and social factors.
Pay attention to the details of care, including side effects and adjuvant medicines.
- Regular laxatives are needed in ALL patients who receive opiates — except those with persistent diarrhea.
- Antiemetics are usually required with initial morphine use, especially in African patients who seem more prone to nausea.
- Not all pain responds to opiates and the ladder.
- Bone pain → NSAIDs +/− opiates
- Nerve compression → steroids
- Increased intracranial pressure (ICP) → steroids
- Inflammation → steroids
- Muscle pain/spasm → muscle relaxants
- Neuropathic pain → tricyclic antidepressants (amitriptyline) and anticonvulsants
| Principle | What It Means | Nursing Action |
|---|---|---|
| Avoid unnecessary delay | Do not make a patient in severe pain wait for hours. | Give pain relief immediately. Do not delay for "doctor's rounds." |
| Give adequate dosages | Do not under-dose out of fear. | Follow the WHO ladder. Titrate up if pain persists. |
| Schedule according to pharmacology | Know how long each medicine lasts. | Morphine lasts 4 hours. Paracetamol lasts 4-6 hours. Plan doses accordingly. |
| Titrate the dose for each patient | Increase gradually until pain is controlled. | Increase morphine by 30-50% every 24-48 hours if needed. |
| Give written instructions | Patients and families need clear guidance. | Write the schedule in simple language or local language. |
| Prescribe a breakthrough dose | Extra medicine for sudden flares of pain. | Give 1/6 to 1/10 of the total daily morphine dose every 1 hour as needed. |
| Prevent and treat side effects | Side effects can stop patients from taking medicine. | Give laxatives with every opioid. Give antiemetics if nausea occurs. |
| Treat other symptoms aggressively | Constipation and muscle spasms make pain worse. | Treat constipation before it becomes severe. Treat spasms with muscle relaxants. |
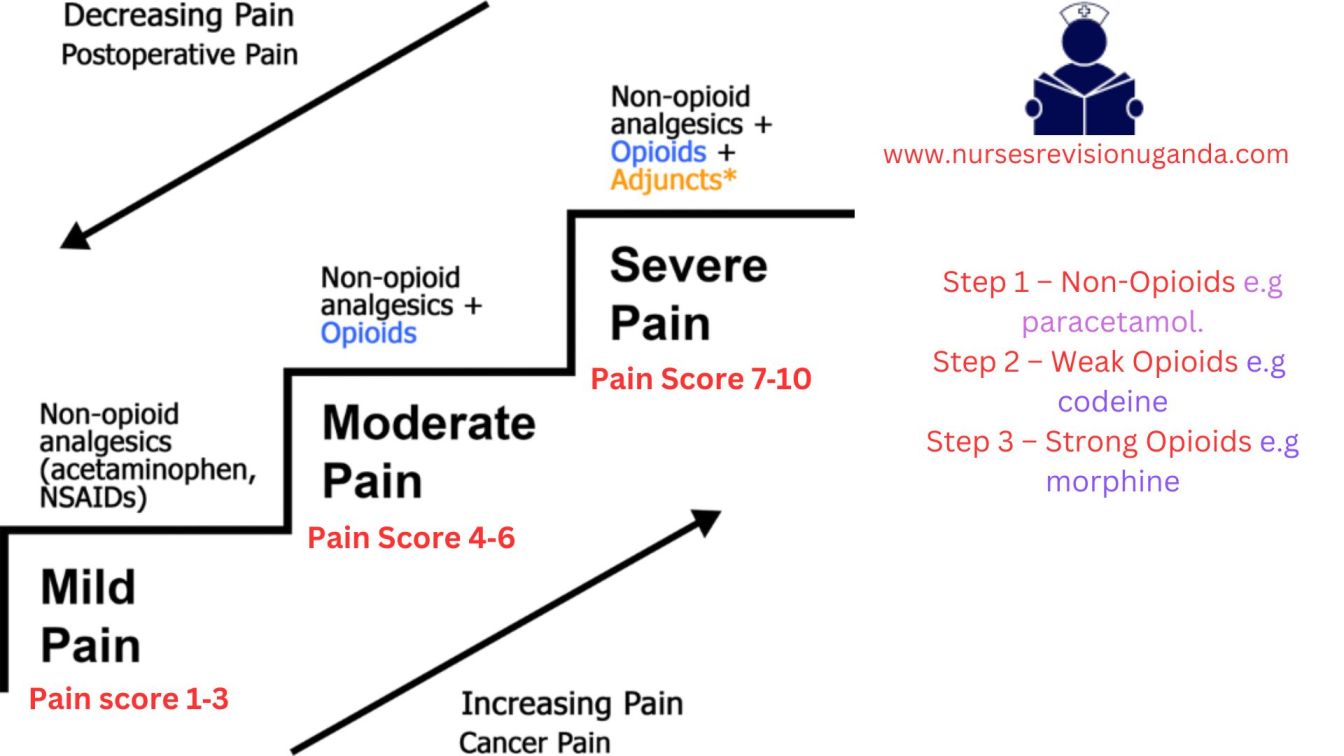
The WHO analgesic ladder was created as a method for effectively managing pain in cancer patients. It has proven successful in providing pain relief to approximately 90% of cancer patients when used correctly.
The ladder has three steps. You move up the ladder as pain severity increases.
Used for pain scores of 1-3 out of 10 (or 1-2 out of 5).
| Paracetamol (Acetaminophen) | |
|---|---|
| Adult dose | 500mg–1g orally every 6 hours |
| Maximum daily dose | 4g (4000mg) per day |
| How it works | Acts centrally in the brain to reduce pain and fever. |
| Notes |
|
| Ibuprofen (NSAID — Non-Steroidal Anti-Inflammatory Drug) | |
|---|---|
| Adult dose | 400mg orally every 6–8 hours |
| Maximum daily dose | 1.2g (1200mg) per day |
| How it works | Acts peripherally to reduce inflammation, pain, and fever. Blocks prostaglandins. (Physiology: Inhibits the Cyclooxygenase (COX) enzymes, stopping the conversion of arachidonic acid to inflammatory prostaglandins). |
| Notes |
|
| Diclofenac (NSAID) | |
|---|---|
| Adult dose | 50mg orally every 8 hours |
| Maximum daily dose | 150mg per day |
| Notes |
|
Paracetamol and NSAIDs can be given together because they work in different ways (paracetamol centrally in the brain, NSAIDs peripherally at the site of injury). This combination often provides far better relief than either drug alone without requiring an opioid.
Used for pain scores of 4-6 out of 10 (or 3-4 out of 5). Used when Step 1 drugs do not control the pain.
| Codeine | |
|---|---|
| Adult dose | 30–60mg orally every 4 hours |
| Maximum daily dose | 240mg per day (this is the "ceiling dose") |
| How it works | A weak opioid that blocks pain signals in the brain and spinal cord. (It is a prodrug; the liver enzyme CYP2D6 converts about 10% of codeine into active morphine). |
| Notes |
|
| Tramadol | |
|---|---|
| Adult dose | 50–100mg orally every 4–6 hours |
| Maximum daily dose | 400mg per day |
| How it works | Weak opioid with additional effects on serotonin and norepinephrine (also helps mood). |
| Notes |
|
Used for pain scores of 7-10 out of 10 (or 5 out of 5). Used when Step 1 and Step 2 drugs do not control the pain.
Morphine is the "gold standard" against which all other opioid analgesics are measured. When used correctly:
- Patients do not become addicted.
- Tolerance is uncommon in the way people fear.
- Respiratory depression does not usually occur when started carefully and titrated properly.
Key principle: The correct morphine dose is the one that gives pain relief. There is no ceiling or maximum dose — the right dose is the one that controls the patient's pain without intolerable side effects. However, you must increase the dose gradually.
| Patient Type | Starting Dose | Frequency | Notes |
|---|---|---|---|
| Standard adult | 5–10mg | Every 4 hours | For patients new to strong opioids |
| Patient changing from Step 2 (e.g., codeine 30mg q4h) | 10mg | Every 4 hours | Already has some opioid tolerance |
| Cachexic patient (very thin/weak) or no prior opioids | 5mg | Every 4 hours | Start low to avoid side effects |
| Frail/elderly patient | 2.5mg | Every 6–8 hours | Due to likelihood of impaired renal function reducing excretion. |
In Uganda, the most common dose is 30mg per 24 hours (e.g., 5mg every 4 hours).
Oral morphine solution comes in different strengths (identified by cap color):
| Strength | Color | Concentration | Typical Use |
|---|---|---|---|
| Weak | Green | 5mg per 5ml | Starting dose for most patients |
| Strong | Red | 50mg per 5ml | Patients on higher doses |
| Very strong | Blue | 100mg per 5ml | Patients on very high doses |
Nursing tip: Always double-check the concentration before giving morphine. Giving 5ml of the red bottle (50mg) instead of the green bottle (5mg) is a 10-fold overdose!
Black Box Warning:
- When morphine is administered as an epidural drug, patients must be closely monitored in a fully equipped and staffed environment for at least 24 hours due to the risk of adverse effects.
- Extended-release tablets of morphine have a potential for abuse similar to other opioid analgesics.
- Morphine is classified as a Schedule II controlled substance and should be used strictly according to dispensing instructions. Tablets or capsules should be taken whole and should not be broken, chewed, dissolved, or crushed.
- Alcohol consumption should be avoided when taking morphine products.
- Failure to adhere to these warnings could result in fatal respiratory depression.
"Titrating" means adjusting the dose until pain is controlled.
How to titrate:- Start with the initial dose (e.g., 5mg every 4 hours).
- Assess pain regularly.
- If pain is still severe after 24-48 hours: Add the total daily dose + total breakthrough doses given in 24 hours. Divide by 6 to get the new 4-hourly dose.
- OR: Increase by 30–50% increments (e.g., 5mg → 7.5mg → 10mg → 15mg). Increments of less than 30% are ineffective. Do not increase by tiny amounts.
- Patient takes 5mg every 4 hours = 30mg per day.
- Needs 3 breakthrough doses of 5mg each = 15mg extra.
- Total in 24 hours = 45mg.
- New regular dose = 45mg ÷ 6 = 7.5mg every 4 hours.
Even patients on regular morphine may have breakthrough pain — sudden flares of pain that "break through" the regular control.
Management:- Give an additional dose of oral morphine.
- The breakthrough dose is usually 1/6 to 1/10 of the total daily dose.
- If using 30mg per day, breakthrough dose = 5mg.
- If breakthrough doses are needed more than 2-3 times per day, the regular 4-hourly dose needs to be increased.
Once pain is stable on regular immediate-release morphine for 2-3 days:
- Calculate the total daily dose of immediate-release morphine.
- Divide by 2 to get the twice-daily (every 12 hours) slow-release dose.
- Continue to give immediate-release morphine for breakthrough pain.
- Patient takes 10mg every 4 hours = 60mg per day.
- Slow-release morphine = 30mg every 12 hours.
- Continue immediate-release 10mg every 1 hour as needed for breakthrough.
| Route | When to Use | Conversion Ratio |
|---|---|---|
| Rectal | Patient cannot swallow but rectum is functional | Same as oral dose (1:1) |
| Subcutaneous (SC) | Patient cannot swallow, needs continuous infusion | PO:SC = 2:1 (e.g., 10mg oral = 5mg SC) |
| Intravenous (IV) | Rapid relief needed, patient in hospital | PO:IV = 2–3:1 (e.g., 30mg oral = 10mg IV) |
| Buccal (inside cheek) | Small amounts for unconscious patients | Absorbed directly through mouth mucosa |
Pethidine is sometimes used for severe pain, but it is NOT recommended in palliative care because:
| Problem | Explanation |
|---|---|
| Short duration of action | Only lasts 3 hours — too short for chronic pain control. |
| Toxic metabolite | Metabolite norpethidine accumulates and causes CNS excitation and convulsions (seizures), especially in renal impairment. |
| Needs injection | Must be given by IM injection, meaning the patient must be near medical help and endure more pain from the needle. |
| Addiction risk | Higher risk of euphoria and addiction compared to morphine. |
Use pethidine ONLY for: Short-term control of severe pain after an operation — not for long-term palliative care.
Case: A 70-year-old palliative cancer patient is currently on Step 2 of the WHO ladder (Codeine 60mg every 4 hours), but reports his pain is still an 8/10. The doctor suggests adding a low dose of Morphine (5mg) on top of the Codeine. As the nurse, what is your intervention?
Answer: You must intervene and stop this order. Principle 3 (By the Ladder) states that Weak Opioids (Codeine) must NEVER be combined with Strong Opioids (Morphine). They compete for the exact same Mu receptors, so there is no added benefit. The correct action is to stop the Codeine entirely and transition the patient completely onto Step 3 (Morphine).
Understanding how morphine works helps nurses explain it to patients, monitor for side effects, and advocate for proper use.
Morphine exerts its action by:
- Binding to opioid receptors in the brain and spinal cord (specifically mu and kappa receptors), resulting in profound pain relief (analgesia).
(Physiology Expansion: Opioid receptors are G-protein coupled. When morphine binds, it opens Potassium (K+) channels to hyperpolarize the cell, and closes Calcium (Ca2+) channels on the presynaptic nerve. This strictly halts the release of pain neurotransmitters like Substance P and Glutamate!) - Acting on the spinal cord to modify the transmission of pain signals from the periphery to the brain.
- Activating inhibitory pathways from the brain stem and basal ganglia — these are the body's natural "pain control systems." (Specifically, the descending inhibitory pathways from the Periaqueductal Gray - PAG).
- Acting on the limbic system and higher brain centers to modify the emotional response to pain. This is why morphine not only reduces the sensation of pain but also reduces the fear and distress associated with it.
- Affecting the gastrointestinal and respiratory systems partly through the autonomic nervous system and partly through direct interaction with opioid receptors in peripheral tissues.
| Feature | Detail & Physiological Context |
|---|---|
| Plasma half-life | 2–3 hours (unaffected by constant usage) |
| Effective duration of action | Approximately 4 hours (This is the exact pharmacological reason why we dose oral immediate-release morphine every 4 hours!) |
| Metabolism | Mainly in the liver via glucuronidation. |
| Metabolites (CRITICAL) |
|
| Excretion | Glucuronide metabolites are excreted in the urine. |
| Renal impairment | Including normal age-related decline, can lead to accumulation of M3G and M6G, causing adverse effects: cognitive impairment, nausea, vomiting, myoclonus (muscle jerking). |
| Liver disease | Not reported to alter morphine pharmacokinetics significantly, but care must be taken with severe hepatic dysfunction. |
Morphine is indicated for:
| Use | Explanation & Pathophysiology |
|---|---|
| Moderate to severe pain | The primary indication in palliative care. |
| Acute myocardial infarction (heart attack) | Alleviates chest pain and reduces anxiety. (It also causes venodilation, reducing preload on the damaged heart, which decreases cardiac workload). |
| Severe acute and chronic pain | When non-narcotic analgesics have proven ineffective. |
| Pre-anesthetic medication | To calm the patient before surgery. |
| Shortness of breath (dyspnea) | From heart failure and pulmonary edema. (Morphine decreases the brainstem's sensitivity to CO2 build-up, reducing the terrifying sensation of air hunger). |
| Diarrhea | Morphine slows gut movement by binding to Mu receptors in the GI tract. |
| Cough | Morphine heavily suppresses the cough reflex in the medullary cough center. |
| Side Effect | Explanation | Nursing Management |
|---|---|---|
| Constipation | Morphine slows down the gut. This happens to EVERY patient on opioids. Tolerance to constipation NEVER develops. | Always give a laxative alongside morphine (unless the patient has diarrhea). Example: Bisacodyl 5mg at night, increase to 15mg if needed. |
| Nausea and vomiting | Morphine stimulates the Chemoreceptor Trigger Zone (CTZ) in the brain. Common in the first few days. | Give anti-emetics: Metoclopramide (Plasil) 10mg every 8 hours OR Haloperidol 0.5–1.5mg once a day. |
| Drowsiness | Common in the first few days as the body adjusts. | Reassure the patient. If it persists beyond 3 days, reduce the morphine dose slightly. |
| Itching (Pruritus) | Not very common, but can occur. (Due to morphine directly causing mast cells to release histamine—this is a side effect, NOT a true allergic reaction). | Reduce the dose of morphine if needed. Give antihistamines. |
- Acute or severe asthma: Morphine can worsen respiratory symptoms (depresses respiratory drive and releases histamine causing bronchoconstriction).
- Gallbladder disease: May intensify or mask pain from biliary tract spasms. (Morphine specifically causes spasms of the Sphincter of Oddi).
- GI obstruction: Morphine slows gut movement and can worsen a mechanical obstruction.
- Severe hepatic / renal impairment: Metabolism altered or toxic metabolites accumulate.
- Elderly, debilitated, or cachectic patients: Start with reduced doses (e.g., 2.5mg) due to decreased organ function and body mass.
- Adverse Effects: Dysphoria (restlessness/depression), Hallucinations, Dizziness, Overdose (severe respiratory depression or cardiac arrest).
- Interactions:
- CNS Depressants (alcohol, sedatives) potentiate respiratory depression.
- MAO Inhibitors (antidepressants) increase risk of Serotonin Syndrome (agitation, hallucinations, rapid heartbeat, high temp).
- Tricyclic Antidepressants enhance analgesia but increase sedation.
- Epidural morphine: Monitor closely for 24 hrs due to delayed respiratory depression.
- Extended-release tablets: Do not break, chew, dissolve, or crush! Breaking them destroys the slow-release matrix, causing a massive, fatal dose dumping.
- Avoid alcohol: Synergistic respiratory depression.
| Date: | 25/3/2014 |
| Patient: | Baluku John |
| IP No: | 123/14 |
| Age / Sex: | 68 years / Male |
| Diagnosis: | Cancer of the penis (Ca penis) |
| Medication: | Liquid morphine 5mg in 5ml (Green cap) |
| Instructions: | Take 5ml every 4 hours AND 10ml at night (Double dose at night helps patient sleep through without waking up for a dose) |
| Supply: | 250ml |
Morphine overdose is rare when used correctly, but nurses must know how to respond.
- Naloxone: A pure opioid receptor antagonist. It rips morphine off both mu and kappa receptors to reverse effects. Given IV. Restores normal breathing and consciousness.
- Administration Alert: Administer if respiratory rate is fewer than 10 breaths per minute.
- Adverse effects: Sudden rapid loss of analgesia (severe pain returns instantly!), increased BP, tremors, hyperventilation.
- Clinical Caution: The half-life of Naloxone is very short (30-60 mins). The half-life of Morphine is longer. The patient can slip back into an overdose state once the Naloxone wears off. Continuous monitoring and multiple doses are often needed!
- Activated charcoal / Laxatives: Used if oral overdose just occurred, to bind morphine in gut and promote elimination.
These three concepts are often confused. Nurses must understand the difference to educate patients and families.
- Opioid Dependence: Means the patient cannot function without the drug.
- Psychological dependence (addiction): Cravings and compulsive drug-seeking behavior. Very rare in patients using morphine for real pain.
- Physiological dependence: The body physically adapts. If the drug is stopped abruptly, the patient gets withdrawal symptoms (sweating, tremors, diarrhea). Prevented by tapering gradually over 2-3 days.
- Therapeutic dependence: The underlying cause of pain is not resolved, so the patient needs ongoing morphine. This is normal and appropriate.
- Tolerance: The body gets used to the drug, and higher doses may be needed over time to achieve the same effect.
- Myth: "If we increase the dose, the patient is becoming addicted."
- Truth: Needing more morphine usually means the disease is progressing (the tumor is growing/pain is getting worse), not addiction.
- Addiction: Very rare in medical settings when used for real pain. Driven by psychological craving for a "high," not pain relief.
- Cognitive Impairment: Some sedation/memory deficit may occur for the first 3-5 days. This is NOT addiction; it is simply the brain adjusting. It usually resolves completely.
Many patients, families, and even health workers in Uganda fear morphine. These fears prevent patients from getting the relief they need. You must address each myth with facts.
| Myth / Fear | The Clinical Truth |
|---|---|
| "Morphine is only offered when death is imminent. / Reserved until the end." | The degree of pain, not the stage of illness, determines the need. Early use does not diminish later effectiveness. There is no upper dose limit! |
| "Morphine hastens death / kills patients." | Morphine relieves suffering, it does NOT speed up death. Properly prescribed, it allows patients to function and live with dignity. |
| "Pain medications always cause heavy sedation." | Initial sedation occurs due to chronic sleep deprivation. Once rested and pain-free, patients regain normal alertness. |
| "Injectable morphine is more effective than oral." | Oral morphine is well absorbed and is the preferred route (By the Mouth). Injections are only for when oral is impossible. |
| "Patients cannot experience pain while sleeping / laughing." | Pain can wake patients from sleep. Distraction (laughing/TV) reduces pain perception temporarily, but the physical pain is still there. |
| "Vital signs are reliable indicators of pain." | Vital signs can be completely NORMAL in chronic pain because the autonomic nervous system adapts. Always trust the patient's self-report! |
Adjuvants are drugs primarily used for other purposes but are highly effective in relieving pain under certain circumstances, especially for opiate semi-responsive and opiate-resistant pain.
- Use: Neuropathic pain (burning, electric, shooting nerve pain).
- Mechanism: Increases serotonin and norepinephrine in the spinal cord, which strengthens the descending inhibitory pain pathways.
- Dose: Start 12.5mg at night. It takes up to a week to see response. (Given at night because a side effect is drowsiness).
- Side effects: Anticholinergic effects (dry mouth, urinary retention, postural hypotension).
- Use: Neuropathic pain (stabbing/shooting nature).
- Mechanism: Blocks voltage-gated sodium/calcium channels, stopping the hyper-excitable "misfiring" of damaged nerves.
- Side effects: Sedation, ataxia (unsteady walking), dizziness.
- Use: Raised Intracranial Pressure (headache), Nerve compression, Metastatic bone pain, Organ capsule distension (liver tumor stretching capsule).
- Mechanism: Massively reduces peritumoral edema (swelling around the tumor).
- Side effects: Gastric irritation, oral thrush (candidiasis), fluid retention, steroid-induced diabetes. (Caution in HIV/AIDS patients - may need prophylactic fluconazole).
- Use: Spasmodic pain (biliary colic, bowel obstruction, ureteric colic).
- Use: Intractable metastatic bone pain. (Mechanism: Inhibits osteoclasts, stopping the tumor from destroying the bone).
- Antibiotics: For fungating, infected wounds.
- Frangipani petals: Traditional remedy for post-herpetic neuralgia (shingles pain).
- Capsaicin cream: Depletes Substance P in nerve endings for neuropathic pain.
Pain is influenced by psychological, cultural, social, and spiritual factors. These methods work alongside medicines — they do not replace them.
Why does massage or rubbing an injury make it feel better? According to Melzack & Wall's Gate Control Theory, non-painful tactile stimulation (rubbing/massage) activates large, fast A-beta nerve fibers. These fast fibers rush to the spinal cord and physically "close the gate" on the slower C-fibers that are trying to carry the pain signals up to the brain!
- Physical: Massage, heat/cold, physiotherapy, surgery, radiotherapy. (Shrinks tumors, reduces muscle tension).
- Psychological: Counseling, relaxation, imagery, distraction (music, TV). (Reduces anxiety which amplifies pain).
- Social: Financial/legal support, family counseling. (Resolves worries that make pain feel worse).
- Spiritual: Prayer, life review. (Addresses fear of death and loss of meaning).
- Not all methods suit every patient (e.g., do not massage a bone with metastases; do not use heat on an open wound).
- Do not tell a patient in severe pain to "just pray". Give morphine AND provide spiritual support.
- In resource-limited settings like Uganda, these methods are especially valuable when medicines are scarce.
- Buccal Absorption: Oral morphine can be absorbed through the buccal mucosa or rectum—useful for unconscious patients.
- Treat Pain First: A patient in severe pain cannot discuss psychosocial concerns or make end-of-life decisions. Control the physical pain first!
- Psychosocial Aggravation: No amount of analgesia will relieve pain if the root cause is untreated fear, guilt, or family conflict (Total Pain concept).
- Short-Term Use is Safe: Opiates can be used short-term for sickle cell crisis, burns, or cryptococcal meningitis without causing addiction.
- Constipation Prevention: Assess for side effects at every interaction. Constipation is the most common side effect and MUST be prevented proactively.
Case: A 45-year-old female with advanced cervical cancer presents with severe, burning, shooting pain radiating down her right leg. She is currently taking Morphine 10mg every 4 hours, but complains the pain is keeping her awake at night. What adjuvant medication would be the most appropriate addition to her regimen?
Answer: The burning, shooting nature of the pain indicates it is Neuropathic Pain (likely from the tumor pressing on the lumbosacral plexus). The best addition is an Antidepressant (e.g., Amitriptyline 12.5mg at night) or an Anticonvulsant (e.g., Gabapentin). Amitriptyline is especially useful here because it treats neuropathic pain and its side effect of drowsiness will help her sleep through the night.
- World Health Organization (WHO) Guidelines for the Pharmacological and Radiotherapeutic Management of Cancer Pain in Adults and Adolescents.
- Palliative Care Association of Uganda (PCAU) and Ministry of Health Uganda Clinical Guidelines on Pain Management.
- Melzack R, Wall PD. Pain mechanisms: a new theory. Science. 1965 Nov 19;150(3699):971-9.
Thanks for the great work. It’s really good