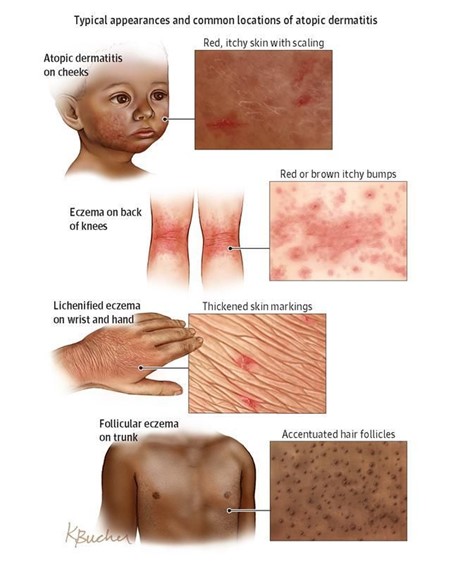
Signs and symptoms of Atopic Dermatitis
- Dry and scaly skin that spans the entire body, except perhaps the diaper area: Atopic dermatitis can cause dry, scaly skin that affects most of the body, except for areas that are usually covered by a diaper.
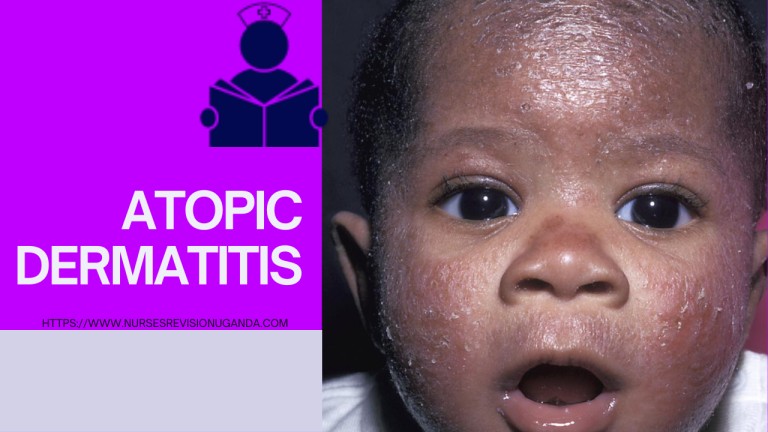
- Intensely itchy red, splotchy, raised lesions in the bends of the arms or legs, face, and neck: These lesions are a hallmark symptom of atopic dermatitis and can be extremely itchy. They often appear in the creases of the elbows, knees, and neck.
- Dennie-Morgan infraorbital fold, infra-auricular fissure, and periorbital pigmentation on the eyelids: These are subtle signs of atopic dermatitis that can appear on the eyelids. The Dennie-Morgan infraorbital fold is a crease below the lower eyelid, the infra-auricular fissure is a groove in front of the ear, and periorbital pigmentation is darkening of the skin around the eyes.
- Post-inflammatory hyperpigmentation on the neck, giving it a classic ‘dirty neck’ appearance: This is a darkening of the skin on the neck that can occur after inflammation from atopic dermatitis.
- Lichenification, excoriation, erosion, or crusting on the trunk, indicating secondary infection: Lichenification is a thickening and hardening of the skin, excoriation is scratching of the skin, erosion is a loss of the top layer of skin, and crusting is a buildup of dried fluid on the skin. These signs can indicate that a secondary infection has developed on the skin.
- Flexural distribution with ill-defined edges with or without hyperlinearity on the wrist, finger knuckles, ankle, feet, and hand: Flexural distribution means that the rash appears in the creases of the body, such as the elbows, knees, and wrists. Ill-defined edges means that the rash does not have a clear border. Hyperlinearity is an increase in the lines on the palms of the hands and soles of the feet.
Additionally;
- Dry, itchy skin: Intense itching is a hallmark symptom.
- Redness and inflammation: Skin appears red and inflamed, often with small bumps or blisters.
- Eczema: Dry, scaly patches of skin that can become crusty or oozing.
- Oozing or crusting: Blisters or lesions may break open and release fluid that crusts over.
- Lichenification: Thickening and hardening of the skin due to chronic scratching.

- Skin infections: Due to compromised skin barrier, infections such as staph or yeast can occur.
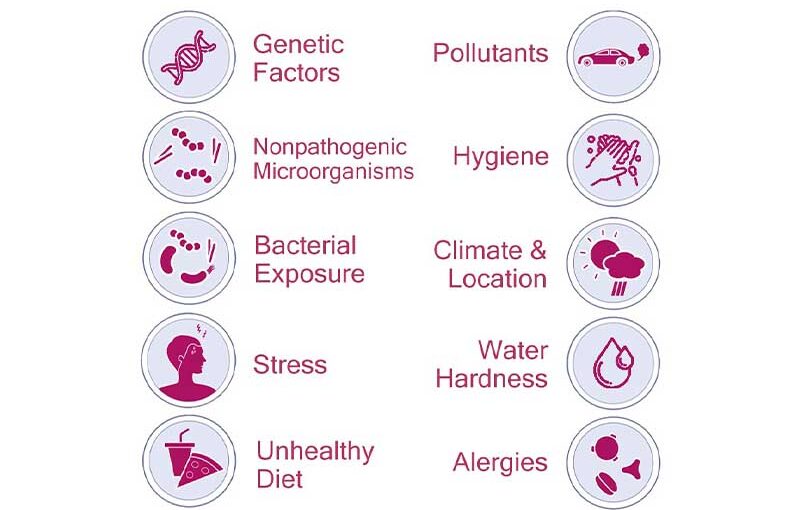
- Allergic reactions: Atopic dermatitis can be triggered by allergens, leading to flare-ups with symptoms such as hives, swelling, and itching.