

Treatment Protocol: Inguinal Buboes Syndrome
Examination and Differential Diagnosis to rule out Non-STI Causes:
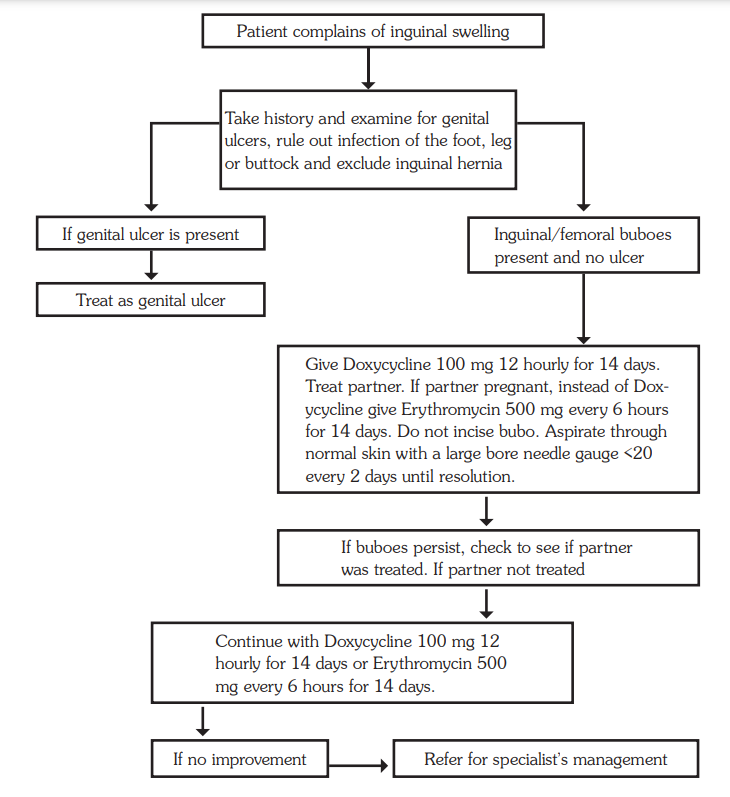
- Thorough clinical examination to rule out non-sexually transmitted infections causing inguinal swellings.
- Rule out infections in the foot, leg, or buttock.
- Exclude the possibility of an inguinal hernia.
- Differential diagnosis to consider both STI-related and non-STI-related etiologies.
Follow the Management Flow Chart:
- Adhere to the syndromic management flow chart for inguinal buboes.
- Treatment options may include antibiotics and other therapeutic measures based on the underlying cause.
- If a genital ulcer is present, initiate treatment following the established protocol.
- Administer doxycycline 100 mg orally every 12 hours for a duration of 14 days.
- Ensure treatment for both the patient and their partner.
Pregnant Partner Consideration:
- In cases involving a pregnant partner, substitute doxycycline with erythromycin.
- Administer erythromycin 500 mg orally every 6 hours for a period of 14 days.
Aspiration of Fluctuant Swellings:
- Fluctuant swellings, indicative of fluid accumulation, should be aspirated daily.
- Do not incise the bubo; instead, aspirate through normal skin using a large bore needle (gauge <20) every 2 days until resolution.
- As an alternative to doxycycline, azithromycin 1 g as a single dose can be considered.
- Caution: Never incise fluctuant swellings, as this may lead to sinus formation.
Address Underlying STI:
- If LGV or chancroid is diagnosed, initiate appropriate antibiotic therapy as per established guidelines.
- Consider partner notification and treatment to prevent further transmission.
Monitoring and Follow-up:
- Regular monitoring of the swelling’s progression and response to treatment.
- Follow-up examinations to assess resolution and ensure the absence of complications.
Persistent Bubo Treatment:
- If the inguinal bubo persists and the partner was not treated, continue the prescribed treatment for an additional 14 days.
Referral for Specialist Management:
- In cases where the condition does not show improvement, consider referral for specialist management.
Thanks for your support
Need some past papers