Enterobacteriaceae II
Enterobacteriaceae: The Primary Pathogens
By the conclusion of this comprehensive module, you will master:
- The distinct virulence mechanisms that separate Primary Pathogens from opportunistic flora.
- The complex taxonomy, pathogenesis, and clinical staging of Salmonella infections (Typhoid vs. Non-Typhoidal).
- The severe localized tissue destruction, molecular spread, and systemic complications of Shigellosis.
- The epidemiological triad, historical significance, and unique clinical presentations of Yersinia species.
- Crucial laboratory diagnostic differentials and modern public health prevention strategies.
I. Introduction to Primary Pathogens
While the vast majority of the Enterobacteriaceae family (such as E. coli, Klebsiella, or Enterobacter) act as opportunistic pathogens—meaning they typically only cause infections when introduced to normally sterile sites (like the urinary tract) or in severely immunocompromised hosts—three specific genera stand apart: Salmonella, Shigella, and Yersinia.
These three genera are classified as Primary Pathogens. This designation means they are inherently, biologically capable of causing severe clinical disease even in perfectly healthy, fully immunocompetent individuals.
The Pathophysiological Edge:
These organisms have evolved highly specialized, aggressive virulence mechanisms. The most notable among these is the Type III Secretion System (T3SS). Operating literally like a microscopic, molecular syringe, the T3SS allows these bacteria to inject toxic "effector proteins" directly into the cytoplasm of host cells. This enables them to actively hijack host cellular machinery, force their own uptake into the cell, paralyze immune defenses (like macrophage digestion), and trigger severe inflammatory syndromes. Understanding these unique mechanisms is absolutely critical for effective clinical practice, laboratory diagnosis, and global public health.
II. Salmonella
1. Classification and Taxonomy
The nomenclature (naming system) of Salmonella is notoriously complex and historically confusing, but modern molecular taxonomy has simplified it into just two official, recognized species: Salmonella enterica and Salmonella bongori.
- S. enterica Subspecies: S. enterica is broadly divided into six distinct subspecies (enterica, salamae, arizonae, diarizonae, houtenae, and indica). The vast, overwhelming majority of human pathogens fall exclusively under subspecies enterica.
- Serotyping (The Kauffmann-White Classification System): Because clinical medicine relies heavily on specific serovars (serotypes) rather than true species names, over 2,600 unique serovars have been identified. They are classified based on the immunological reactivity of three distinct structural antigens:
- O Antigen (Somatic): The outermost portion of the cell wall Lipopolysaccharide (LPS). It is highly variable and determines the serogroup.
- H Antigen (Flagellar): Made of the protein flagellin, which makes up the whip-like tail used for motility. (Note: Salmonella can undergo "phase variation," switching between two different H antigens to evade the host immune system.)
- Vi Antigen (Capsular): Stands for "Virulence." A polysaccharide capsule found only in highly virulent, systemic strains.
Strict Human Pathogens (Systemic Disease)
- S. Typhi and S. Paratyphi A, B, C.
- Disease: Cause Enteric (Typhoid) fever.
- Key Epidemiological Characteristic: These are strictly, exclusively human pathogens. They possess no animal reservoir! You can only contract Typhoid from the feces of another infected human.
Zoonotic Pathogens (Gastroenteritis)
- S. Typhimurium and S. Enteritidis.
- Disease: Major causes of Non-Typhoidal Salmonellosis (NTS).
- Key Epidemiological Characteristic: These are highly zoonotic. They are heavily found in the gastrointestinal tracts of animals, especially chickens, turkeys, cattle, and pet reptiles (like small turtles and iguanas). Cross-contamination of poultry and raw eggs is the classic vector.
Other Notable Serovars: S. Heidelberg, S. Newport, S. Javiana — frequently associated with various agricultural animal reservoirs and massive, multi-state foodborne outbreaks.
2. Morphology and Culture Characteristics
- Gram Stain & Size: Gram-negative rods (bacilli), measuring roughly 2-3 x 0.4-0.6 micrometers.
- Motility: They are aggressively, actively motile by means of peritrichous flagella (flagella pointing outward in all directions around the entire cell body).
Exception: S. Gallinarum and S. Pullorum (which are strictly avian/bird pathogens causing fowl typhoid) are non-motile. - MacConkey Agar: They are Non-lactose fermenting. On MacConkey agar, they appear as transparent, colorless, or pale colonies. This visually distinguishes them instantly from normal healthy E. coli gut flora, which ferment lactose and turn the agar bright pink/red.
- XLD or HE Agar: They uniquely produce H2S (Hydrogen sulfide) gas due to the reduction of thiosulfate. On Xylose Lysine Deoxycholate (XLD) or Hektoen Enteric (HE) agar, they classically and unmistakably present as colorless or red colonies with striking, jet-black centers.
- Stool Culture Media: Because stool contains billions of normal bacteria, specialized selective media are used to suppress normal flora and isolate Salmonella, including XLD, HE, and Bismuth Sulfite (BS) agar (where they appear black with a metallic sheen).
Differentiating the Gut Pathogens
On a routine stool culture, both Salmonella and Shigella will grow as suspicious, colorless, non-lactose fermenting colonies on MacConkey agar. To tell them apart rapidly on the benchtop, the microbiologist will look at the H2S production on XLD or HE agar:
- Salmonella = Black centers (H2S positive).
- Shigella = Colorless/Clear (H2S negative).
3. Virulence Factors and Pathogenesis
Salmonella uses a highly sophisticated, sequential arsenal of weapons to breach the hostile gut lining, survive the brutal environment inside immune cells, and establish infection.
- Lipopolysaccharide (LPS): Possesses powerful Endotoxin activity that triggers massive systemic inflammation, fever, and potential shock. Smooth LPS (which has a complete, long O antigen chain) physically protects the bacteria from complement-mediated killing by the host's immune system.
- Type III Secretion Systems (T3SS): The defining virulence factor. Encoded by specific clusters of DNA known as Salmonella Pathogenicity Islands (SPI). Salmonella relies on two completely distinct systems:
- SPI-1 T3SS (The Breacher): Mediates the initial invasion of the intestinal epithelium. It injects effector proteins that cause massive, rapid host cytoskeleton rearrangement (a phenomenon called "membrane ruffling"). This forces the normally non-phagocytic epithelial cell to literally reach out and "swallow" (endocytose) the bacteria into the intestinal wall.
- SPI-2 T3SS (The Survivor): Once swallowed by a tissue macrophage, the bacteria should theoretically be destroyed by acid and enzymes. However, SPI-2 activates and injects proteins that physically prevent the deadly lysosome from fusing with the Salmonella-containing vacuole (SCV). This creates a safe, protected bubble where the bacteria can happily replicate deep inside the very immune cell meant to kill it!
- Vi Capsular Polysaccharide: Present almost exclusively in systemic S. Typhi and S. Paratyphi C. This dense, slippery sugar coating masks the O-antigen, making the bacteria powerfully anti-phagocytic. Because it is highly unique and immunogenic, it is the exact target used in the formulation of the modern Typhoid vaccine.
- Fimbriae (Pili): Multiple specialized fimbrial types mediate strong, targeted adherence to the intestinal epithelium, preventing the bacteria from simply being washed away by peristaltic bowel movements or diarrheal flushing.
4. Typhoid Fever (Enteric Fever)
Typhoid fever is a life-threatening, systemic, widely disseminating infection caused exclusively by S. Typhi. Because it is a strict human pathogen, transmission relies entirely on the fecal-oral route from a human carrier (e.g., contaminated municipal drinking water, or chronic shedding by food handlers lacking proper hand hygiene).
- The Pathogenesis (The Trojan Horse): Following ingestion and survival of stomach acid, the organisms penetrate the intestinal mucosa in the terminal ileum. They are taken up by M cells and underlying macrophages. Using SPI-2, they survive inside the macrophages and use them as a "taxi" or "Trojan Horse" to disseminate systemically via the lymphatics directly into the bloodstream, seeding the liver, spleen, and bone marrow.
- Incubation period: Typically 7 to 14 days, but can vary widely from 3 to 60 days depending on the infectious dose ingested.
Characteristic Clinical Features:
- Prolonged, gradually stepping-up fever: Fever slowly climbs higher each day over the first week.
- Severe headache, malaise, and "pea-soup" diarrhea (though constipation is actually common early in the disease).
- Relative bradycardia: A highly testable, classic clinical sign where the patient's heart rate is inexplicably slower than expected for the extreme degree of high fever (e.g., a temperature of 104°F/40°C but a pulse of only 70 bpm).
- Rose spots: A faint, blanching, salmon-colored maculopapular rash typically appearing on the chest and trunk during the second week of illness.
- Hepatosplenomegaly: Massive enlargement of the liver and spleen due to extreme macrophage infiltration and bacterial replication.
- Intestinal bleeding and perforation (The Surgical Emergency): Occurs in the critical 3rd week. The Peyer's patches (lymphoid tissue in the gut wall) become so hyperactive, swollen, and necrotic that they literally ulcerate and burst, spilling bowel contents into the sterile peritoneum, causing fatal peritonitis.
The Chronic Carrier State & Typhoid Mary
The bacteria have an extreme affinity for the biliary tract and love to colonize the Gallbladder, where they actively form thick biofilms on gallstones. Up to 5% of all recovered patients become chronic, asymptomatic carriers. They appear perfectly healthy but continuously shed millions of virulent bacteria in their feces for years. The most famous example is Mary Mallon ("Typhoid Mary"), an asymptomatic cook in New York who infected dozens of people through her meals.
Diagnosis Timeline for Typhoid Fever
To definitively remember which laboratory test is the most accurate during which specific week of Typhoid fever progression, use the classic medical mnemonic BASU:
- Week 1: Blood culture (Bacteria are actively in the blood spreading/bacteremia).
- Week 2: Agglutination (The Widal Test - Host antibodies against O and H antigens begin to rise significantly).
- Week 3: Stool culture (Bacteria are shed massively from the gallbladder back into the gut lumen).
- Week 4: Urine culture.
*Crucial Note: Bone marrow culture possesses the absolute highest sensitivity regardless of the week, yielding positive results even if the patient has already begun empirical antibiotic therapy!
5. Non-Typhoidal Salmonellosis (NTS)
Caused by zoonotic serovars like S. Typhimurium and S. Enteritidis. This is the single most common foodborne bacterial illness globally, responsible for millions of cases of food poisoning annually.
- Clinical Presentation: Unlike the deep systemic spread of Typhoid, NTS typically causes acute, brutal, but self-limiting gastroenteritis 6 to 72 hours after ingestion. The localized immune response is so aggressive it keeps the bacteria confined to the gut.
- Symptoms: Profuse watery diarrhea, severe abdominal cramps, low-grade fever, nausea, and vomiting. Usually resolves in 2-7 days without antibiotics.
- Risk Factors & Examples: Consumption of undercooked poultry (chicken/turkey), raw or undercooked eggs (cookie dough, raw mayonnaise), and cross-contaminated cutting boards. Also strongly linked to handling pet reptiles (turtles, snakes, iguanas) and backyard flocks (pet chickens).
Invasive NTS (iNTS) & Sickle Cell Disease
While usually confined to the gut, the bacteria can become invasive and enter the bloodstream in heavily immunocompromised individuals (HIV/AIDS, extreme age, severe malaria), particularly in sub-Saharan Africa.
Sickle Cell Connection: Patients with Sickle Cell Disease are uniquely, highly susceptible to Salmonella Osteomyelitis (bone infection). Micro-infarcts in their bones (due to sickling) create dead tissue that acts as a perfect nidus for circulating Salmonella to settle in, exacerbated by poor macrophage and splenic function.
6. Laboratory Diagnosis of Salmonella
Accurate, rapid identification is crucial for patient care, public health tracking, and identifying massive foodborne outbreak sources.
- Specimens: Blood (essential for typhoid fever diagnosis), stool (for gastroenteritis and identifying chronic carriers), urine, or bone marrow (the gold standard for typhoid).
- Culture Methods:
- Enrichment Broth: Because a stool sample contains billions of competing normal flora, the sample is first placed in Selenite F or Tetrathionate broth. These specialized liquids chemically inhibit normal gut flora while wildly enriching and multiplying the small numbers of Salmonella present.
- Selective Agar: The enriched sample is then plated on XLD or HE agar to look for black-centered colonies.
- Biochemical Identification:
- Lactose negative.
- H2S (hydrogen sulfide) positive.
- Lysine decarboxylase positive.
- Serotyping: Confirmed via slide agglutination tests using specific O (somatic) and H (flagellar) antisera to definitively name the serovar.
- Advanced Molecular Methods:
- PCR: For rapid amplification and detection of specific virulence genes.
- PFGE (Pulsed-Field Gel Electrophoresis): Historically used for outbreak investigation (creating a "DNA fingerprint" to link a sick patient to a specific contaminated food batch).
- WGS (Whole Genome Sequencing): The modern, absolute gold standard for global surveillance, precise strain tracking, and identifying exact antibiotic resistance genes.
The Classic Typhoid Presentation
Case: A 25-year-old chef presents to the clinic with a 10-day history of a steadily increasing fever, a severe, unrelenting headache, and a pulse rate of 65 bpm (despite an extremely high body temperature of 39.5°C). Upon physical examination, you notice faint, pink, blanching macules scattered across his abdomen. You strongly suspect Enteric Fever.
- What is the most likely causative organism?
- Given he is in exactly week 2 of his illness, what is the best non-invasive culture sample to obtain right now to confirm the diagnosis?
Answers:
- Salmonella Typhi (This is the absolutely classic, textbook presentation characterized by step-ladder fever, relative bradycardia, and rose spots on the trunk).
- Blood culture (or a Widal agglutination serology test. Stool culture yield will dramatically increase as he enters week 3, according to the BASU timeline).
III. Shigella
1. Classification
The genus Shigella is the classic agent of bacillary dysentery. Genetically, they are essentially highly specialized, aggressive clones of E. coli. They are divided into four distinct species (formerly called subgroups), categorized based on their biochemical profiles and specific O-antigens:
- S. dysenteriae (Group A): The most virulent, devastating species. Type 1 produces the deadly Shiga toxin and causes massive, severe, life-threatening epidemic disease, often seen in refugee camps and war zones.
- S. flexneri (Group B): The predominant species causing widespread endemic disease in developing countries.
- S. boydii (Group C): Relatively uncommon globally, restricted mostly to the Indian subcontinent.
- S. sonnei (Group D): The predominant species causing shigellosis in developed/industrialized countries (USA, Europe). Causes the mildest, watery form of the disease. Often spreads rapidly in daycare centers and among Men who have Sex with Men (MSM).
Shigella Subgroups
To rapidly memorize the groups A, B, C, and D strictly in order of their severity and names, use:
"Dirty Fingers Bring Shigella"
- Dysenteriae (Group A) - Most severe, deadly.
- Flexneri (Group B)
- Boydii (Group C)
- Sonnei (Group D) - Least severe, most common in the West.
2. Virulence Factors and Pathogenesis
Shigella is a master of targeted tissue destruction. Its entire life cycle is focused on invading the colon, destroying the lining, and avoiding the blood.
- Very Low Infectious Dose: It takes an incredibly tiny amount—only 10 to 100 organisms—to cause severe disease!
Physiology Expansion: Unlike Salmonella or Vibrio cholerae, which require millions of bacteria to be ingested because they are easily destroyed by stomach acid, Shigella is astonishingly acid-resistant. It effortlessly survives the brutal gastric acid barrier to reach the intestines. - Invasion (Type III Secretion System): Encoded by a massive, complex virulence plasmid. The T3SS acts as a molecular syringe to inject effector proteins, forcing the normally impenetrable colonic epithelium to engulf the bacteria.
- Pathogenesis Pathway: Shigella first enters through specialized M cells in the gut. It is swallowed by underlying macrophages, but quickly triggers rapid apoptosis (killing the macrophage from the inside out). Escaping the dead macrophage, it invades adjacent, healthy epithelial cells from the bottom up (basolaterally).
- Intracellular Spread (The IcsA Protein): Once inside the safety of the host cytoplasm, Shigella uses a unique surface protein called IcsA to physically hijack the host cell's actin cytoskeleton. It rapidly builds long "actin comet tails" at one end of the bacteria. This acts like a rocket engine, propelling the bacteria rapidly from the inside of one cell directly through the wall into the next adjacent cell, entirely avoiding the extracellular space and circulating antibodies! (Listeria monocytogenes uses a very similar mechanism).
- Systemic Confinement: Unlike Salmonella Typhi, Shigella almost never disseminates systemically into the bloodstream. It remains strictly confined to the intestinal epithelium, causing severe, localized, bloody tissue destruction and ulceration.
- Shiga Toxin (Stx): Produced exclusively by S. dysenteriae type 1.
- Mechanism: It is an A-B complex toxin. It acts by permanently, irreversibly inhibiting host cell protein synthesis. It does this by catalytically cleaving a highly specific adenine residue from the 28S rRNA of the 60S ribosomal subunit.
- Consequence: Kills vascular endothelial cells in the gut and kidneys. The damaged blood vessels trigger massive platelet aggregation, shredding red blood cells (creating schistocytes) and leading to the deadly Hemolytic Uremic Syndrome (HUS).
3. Clinical Features of Shigellosis
- Incubation period: Very short, typically 1 to 3 days.
- Bacillary Dysentery: The classic, defining presentation. Patients suffer from frequent, extremely small-volume stools that are densely packed with bright red blood, thick mucus, and pus. This is accompanied by severe lower abdominal cramps, high fever, and tenesmus (a painful, persistent, urgent, but completely unproductive spasm to defecate because the rectum is heavily inflamed, though empty).
- Severe Cases: S. dysenteriae type 1 causes the most devastating form of dysentery, carrying a high mortality rate, especially in pediatric populations in resource-limited settings without IV hydration.
- Severe Complications:
- Rectal prolapse: Due to extreme, repeated straining from tenesmus.
- Toxic megacolon: Complete inflammatory paralysis and massive, deadly dilation of the colon.
- Hemolytic Uremic Syndrome (HUS): The classic, testable triad of acute renal failure (Acute Kidney Injury), profound thrombocytopenia (low platelets), and microangiopathic hemolytic anemia (shredded red blood cells). Triggered directly by the circulating Shiga toxin.
4. Laboratory Diagnosis
- Specimen: Fresh stool is absolutely required (rectal swabs are significantly less sensitive and generally discouraged).
- Direct Microscopy: The visual presence of massive amounts of fecal leukocytes (neutrophils) and red blood cells under the microscope strongly, rapidly indicates invasive inflammatory diarrhea. This instantly differentiates it clinically from watery, toxin-mediated diarrheas like Cholera or ETEC.
- Culture: Uses selective media like XLD, HE, or Salmonella-Shigella (SS) agar. Shigella grows exclusively as non-lactose fermenting (colorless) colonies.
- Biochemical Identification (The "Negative" Bug): Shigella is notoriously and characteristically biochemically inert (lazy) compared to all other Enterobacteriaceae! It lacks almost all extra features:
- Non-motile (Lacks H-antigen flagella entirely).
- Lactose-negative.
- H2S-negative (Absolutely no black centers on XLD/HE agar).
- Lysine-negative.
- Non-gas-producing from glucose fermentation.
- Serotyping: Confirmed in reference labs via slide agglutination with specific Group A, B, C, or D antisera.
- Antimicrobial Susceptibility: Absolutely essential. Shigella has acquired widespread, rapidly increasing resistance globally, particularly rendering older drugs like Ampicillin useless, and now showing severe fluoroquinolone resistance.
IV. Yersinia
1. Classification and Overview
There are three specific species in this genus that cause human disease: Y. pestis (the terrifying agent of the plague), Y. enterocolitica (causing severe foodborne enterocolitis), and Y. pseudotuberculosis (a rare cause of mesenteric adenitis). Historically, Y. pestis is one of the most terrifyingly virulent bacterial pathogens known to human history, responsible for ancient pandemics with massive, civilization-altering mortality (e.g., The Black Death of the 14th century).
2. Yersinia pestis — The Plague
- Transmission: It is a highly deadly zoonotic pathogen maintained in wild rodent reservoirs (rats, mice, and notably prairie dogs in the Southwestern United States). It is transmitted between animals and to humans by flea vectors. Humans are merely incidental (accidental) dead-end hosts.
Flea Cycle Expansion: The bacteria multiply massively in the flea's gut, creating a biofilm that physically blocks the flea's digestive tract. The flea begins to starve, jumps to a human out of desperation, and violently regurgitates the blockage of bacteria directly into the human's bloodstream during a bite. - Microscopic Hallmark: Exhibits classic bipolar staining. When stained with Wayson or Giemsa stains, the ends of the rod stain darkly while the middle is clear, giving it an unmistakable 'safety pin' appearance.
Clinical Forms of Plague:
The most common form. Bacteria multiply massively in the regional draining lymph nodes nearest the flea bite, causing massively swollen, agonizingly exquisite, tender nodes called buboes (typically presenting in the groin or axilla/armpit).
Bacteria bypass the lymph nodes and replicate directly and massively in the bloodstream. The resulting endotoxic shock causes intravascular coagulation, leading to severe necrosis and gangrene of the extremities (fingers, toes, nose turning black—hence the name "Black Death").
Can be primary (inhaled directly from a coughing patient) or secondary (spread from the blood to the lungs in a bubonic patient). It is highly contagious from human to human via respiratory droplets and is nearly 100% fatal within 24-48 hours if untreated.
Virulence Factors & Treatment:
- F1 capsule: Strongly anti-phagocytic. Fascinatingly, it is expressed only at 37°C in the warm mammalian human host, but completely turned off in the cold flea.
- Plasminogen activator (Pla): A protease enzyme that actively degrades fibrin blood clots, preventing the body from walling off the infection and allowing the bacteria to rapidly spread through tissues.
- Type III Secretion System (Ysc) & V/W Antigens: Injects deadly Yop proteins directly to paralyze and destroy macrophages.
- Diagnosis & Treatment: Culture requires intense, high-security Biosafety Level 3 (BSL-3) precautions! Diagnosed via rapid antigen detection, serology, and PCR. Streptomycin or Gentamicin are absolute first-line treatments. Fluoroquinolones or Doxycycline are modern alternatives. Mortality wildly exceeds 50% if left untreated.
- Vaccine: A live attenuated vaccine is available, but due to side effects, it is restricted strictly to high-risk laboratory personnel studying the bug.
3. Yersinia enterocolitica
- Epidemiology: Occurs worldwide, especially prevalent in cooler northern climates (Scandinavia, Northern Europe). Transmission is typically via the consumption of contaminated, undercooked pork products (classically chitterlings/pork intestines) or unpasteurized milk.
- Clinical Syndromes:
- Enterocolitis: Presents with bloody diarrhea, fever, and severe abdominal pain.
- Mesenteric adenitis (Pseudoappendicitis syndrome): The classic, highly testable presentation in children and young adults. It causes massive, localized inflammation of the terminal ileum and mesenteric lymph nodes. It perfectly mimics acute appendicitis (presenting with right lower quadrant pain, fever, and high WBCs), routinely leading to many unnecessary appendectomies!
- Post-infectious sequelae: In genetically susceptible individuals (HLA-B27 positive), it can trigger Reactive arthritis (the triad of "can't see, can't pee, can't climb a tree") and Erythema nodosum (painful, raised, red nodules on the front of the shins).
- Unique Lab Characteristic (Psychrotrophic): Y. enterocolitica can survive, thrive, and actually grow exponentially at 4 degrees Celsius (refrigerator temperatures).
- Lab utility: This allows for "cold enrichment" in the lab. Incubating stool at 4°C for 1-3 weeks kills competing normal flora while Yersinia flourishes.
- Clinical danger: It can multiply silently in refrigerated blood-bank products (packed RBCs) harvested from an asymptomatic donor. When transfused into a patient, it causes massive, immediate, fatal endotoxic shock and transfusion reactions!
- Identification: Urease-positive, oxidase-negative. Grows specifically on CIN agar (cefsulodin-irgasan-novobiocin selective), where it uniquely ferments mannitol forming classic, unmistakable "bulls-eye" colonies with deep red centers and translucent borders.
- Pathogenic Biotypes: Biotype 1B is highly virulent (contains a high-pathogenicity island); biotypes 2-5 are moderately virulent. Virulence factors include InvA (for invasion), Yst enterotoxin, T3SS, and advanced iron acquisition systems.
V. Prevention and Control of Enterobacteriaceae
Because these primary pathogens heavily exploit the fecal-oral route, zoonotic animal reservoirs, and arthropod vector transmission, systemic public health measures and infrastructure are the absolute cornerstone of disease control.
- Proper, thorough cooking of poultry, eggs, and pork.
- Rigorous, standardized pasteurization of all commercial dairy products.
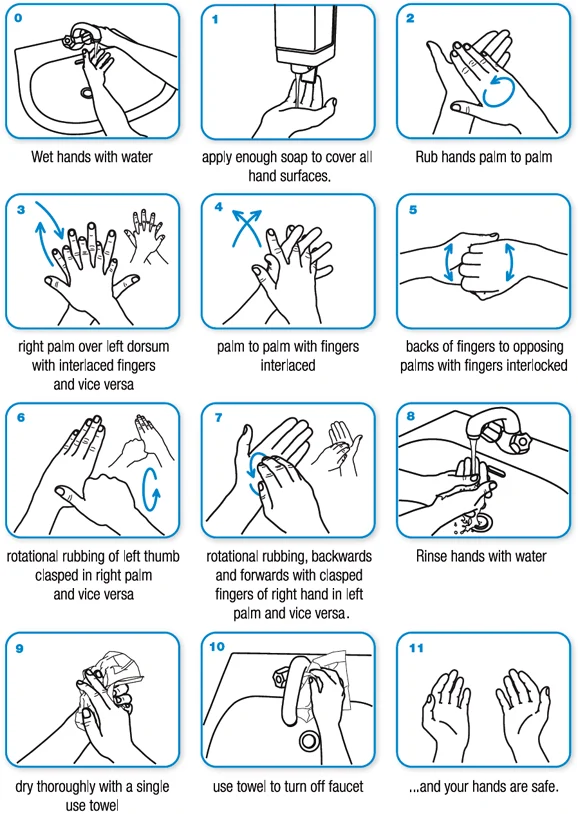
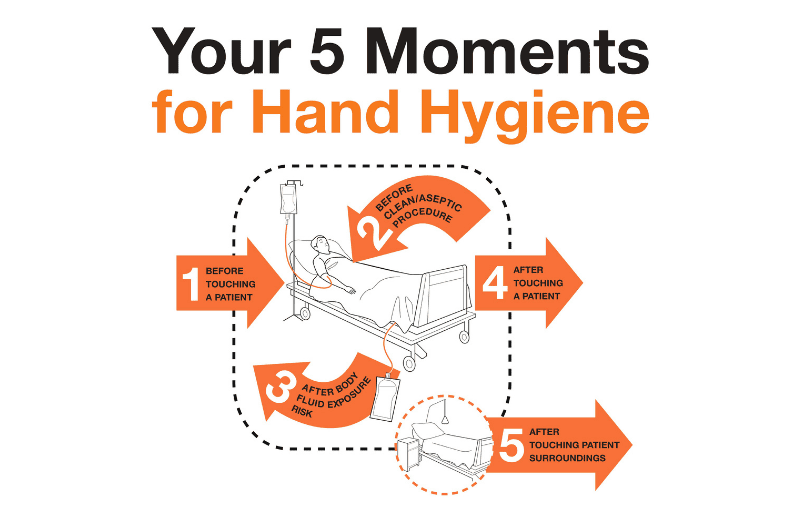
- Meticulous hand washing and kitchen hygiene to prevent cross-contamination (e.g., using separate cutting boards for raw chicken and vegetables). This is crucial for halting Non-Typhoidal Salmonella and Y. enterocolitica.
- Provision of clean, chemically treated drinking water and modernized sewage disposal infrastructure are absolutely critical for preventing massive, endemic outbreaks of Typhoid fever and Shigellosis in developing regions. Without basic sanitation, these pathogens spread uncontrollably.
- Typhoid Vaccines: Three types exist:
- Vi capsular polysaccharide vaccine (injectable, limits duration of immunity).
- Ty21a live attenuated oral vaccine.
- Vi-conjugate vaccine (TCV): The most modern and effective. The polysaccharide is attached to a carrier protein, making it highly effective in infants by eliciting a strong T-cell dependent immune response, providing longer-lasting immunity.
- Shigella Vaccine: Currently, there is no licensed vaccine available for Shigella, though several candidates are in clinical development.
- Strict rodent and flea vector control measures in endemic areas (e.g., controlling prairie dog populations in campsites).
- Immediate post-exposure antibiotic prophylaxis (e.g., oral Doxycycline) for individuals in close contact with a pneumonic plague patient to halt the deadly spread.
- Antibiotic Stewardship: Widespread, indiscriminate use of antibiotics in agriculture and human medicine has led to massive rises in multidrug-resistant (MDR) strains of S. Typhi and Shigella. Stewardship programs are absolutely critical to preserve the efficacy of last-line oral drugs like Fluoroquinolones and Third-Generation Cephalosporins.
❓ Applied Clinical Question: The Mimic
Case: A 10-year-old boy is rushed to the ER with severe, localized pain in his right lower abdominal quadrant, a high fever, and a drastically elevated white blood cell count. The surgical team strongly suspects acute appendicitis and takes him to the OR to remove the appendix. However, post-surgical pathology reveals a perfectly normal, healthy appendix, but heavily inflamed, swollen mesenteric lymph nodes nearby. Upon questioning, the mother mentions the family ate undercooked pork chops (chitterlings) a few days ago.
- What is the most likely causative organism?
- What specialized culture agar should the microbiology lab use to successfully isolate this specific pathogen?
Answers:
- Yersinia enterocolitica (This is the classic, highly testable presentation of pseudoappendicitis/mesenteric adenitis inextricably linked to the consumption of undercooked pork products).
- CIN agar (Cefsulodin-Irgasan-Novobiocin), incubated optimally at room temperature, which will selectively yield the classic "bulls-eye" colonies.
VI. List of References
- Murray, P. R., Rosenthal, K. S., & Pfaller, M. A. (2020). Medical Microbiology (9th ed.). Elsevier. (Excellent resource for detailed virulence factors and T3SS mechanisms).
- Bennett, J. E., Dolin, R., & Blaser, M. J. (2019). Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases (9th ed.). Elsevier. (The absolute gold standard for clinical presentation and epidemiological data of Enteric Fevers and Plague).
- Ryan, K. J., & Ray, C. G. (2018). Sherris Medical Microbiology (7th ed.). McGraw-Hill Education. (Provides exceptional biochemical and diagnostic agar plate descriptions).
- Centers for Disease Control and Prevention (CDC). Guidelines on Foodborne Illness, Typhoid Fever, and Plague (Yersinia pestis) surveillance. www.cdc.gov
- World Health Organization (WHO). Position papers on the administration and efficacy of the Typhoid Conjugate Vaccine (TCV). www.who.int
Quick Quiz
Bacteriology Intro Quiz
Microbiology - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
Bacteriology Intro Quiz
Microbiology
Preparing questions...
Choose your answer and keep your streak alive.
Great effort.
Here is your quick performance summary.
Enterobacteriaceae II Read More »