Clostridia and Gram-Positive Anaerobic Cocci
Clostridia and Gram-Positive Anaerobic Cocci
By the conclusion of this exhaustive, deeply detailed master guide, you will be highly conversant with:
- The fundamental microbiological characteristics and physiological constraints of obligate anaerobic bacteria.
- The structural mechanisms, neurological targets, and clinical manifestations of the lethal botulinum and tetanus neurotoxins.
- The pathophysiology, diagnostic algorithms, and modern pharmacological management of Clostridioides difficile infections.
- The devastating tissue destruction mediated by the alpha-toxin in Clostridium perfringens gas gangrene.
- The taxonomy, synergistic virulence, and clinical role of Gram-Positive Anaerobic Cocci (GPAC) in polymicrobial abscesses.
I. Introduction to Anaerobic Bacteria & The Genus Clostridium
The genus Clostridium comprises a massive family of Gram-positive, spore-forming, obligately anaerobic bacilli. They are ubiquitous in nature, heavily populating soil, decaying vegetation, marine sediments, and the intestinal tracts of humans and animals. From a clinical perspective, while many are harmless saprophytes, several specific species produce the most potent exotoxins known to science, causing severe, rapid, and often life-threatening neuroparalytic and necrotizing diseases.
The most critically important pathogenic species we will dissect in this guide include:
- C. botulinum: The causative agent of botulism (flaccid paralysis).
- C. tetani: The causative agent of tetanus (spastic paralysis).
- C. difficile: (Now formally reclassified as Clostridioides difficile) — the driver of pseudomembranous colitis and healthcare-associated diarrhea.
- C. perfringens: The aggressive agent behind gas gangrene (myonecrosis) and severe food poisoning.
II. General Characteristics of Clostridium
Before diving into the specific pathogens, it is absolutely crucial to understand the shared microbiological and physiological traits that define this lethal genus.
- Morphology: They present as large, thick Gram-positive rods (bacilli), measuring approximately 0.5–2.0 × 1.5–20 micrometers. Under the microscope, they often appear boxcar-shaped or filamentous.
- Oxygen Tolerance (The Anaerobic Constraint): They are obligate anaerobes.
Physiology Expansion: Why does oxygen kill them? Strict anaerobes generally lack crucial antioxidant enzymes, specifically superoxide dismutase (SOD) and catalase. When molecular oxygen is metabolized, it generates highly toxic free radicals (like the superoxide anion and hydrogen peroxide). Without SOD and catalase to neutralize these radicals, the bacteria's DNA and lipids are instantly shredded, resulting in cell death. However, it must be noted that some species (like C. perfringens) are "aerotolerant" and can survive brief exposures to low oxygen tensions. - Spore Formation (The Survival Mechanism): To survive oxygen-rich or nutrient-poor environments, they form highly resilient endospores. Spores are biologically dormant structures with heavily cross-linked keratin coats that resist boiling, drying, harsh chemicals, and ultraviolet radiation. Depending on the species, the spore can be terminal (at the very end), subterminal (near the end), or central. Because the spore is often wider than the bacillus itself, it causes a characteristic bulging appearance (often described pathologically as looking like a "tennis racket" or "drumstick").
- Motility: Most pathogenic clostridia are highly motile via peritrichous flagella (long whip-like tails projecting in all directions around the cell body). A notable, heavily tested exception is C. perfringens, which is strictly non-motile.
- Biochemical Identification: They are universally Catalase-negative. There is only one highly specific, extremely rare exception: C. botulinum Group I strains can sometimes express weak catalase activity.
III. Clostridium botulinum
A. General Features & The Neurotoxin
C. botulinum produces the botulinum neurotoxin (BoNT), which is definitively, molecule-for-molecule, the most potent and lethal biological toxin known to mankind.
- There are seven recognized toxin serotypes (designated A through G). However, only types A, B, E, and F cause human disease. (Type A is the most potent and is used commercially in Botox).
- Structure of BoNT: It is a 150 kDa protein initially produced by the bacteria as a single, inactive polypeptide chain. Host or bacterial proteases subsequently cleave it into a heavy chain (100 kDa) and a light chain (50 kDa), which remain tethered together by a crucial disulfide bond.
- The Heavy chain acts as the "key." It binds to highly specific receptors on peripheral presynaptic nerve terminals (gangliosides and the synaptic vesicle protein SV2). This binding tricks the nerve cell into swallowing the toxin via receptor-mediated endocytosis.
- Inside the nerve vesicle, the acidic environment breaks the disulfide bond, releasing the Light chain into the neuron's cytoplasm.
- The Light chain is a zinc metalloprotease (an enzyme that acts as molecular scissors). Once free, it violently cleaves SNARE proteins (specifically SNAP-25, Syntaxin, or Synaptobrevin, depending on the serotype).
- Physiological Expansion: SNARE proteins act like docking ropes. They are absolutely required to pull vesicles filled with the neurotransmitter Acetylcholine (ACh) to the cell membrane so they can be released. Without SNARE proteins, the ACh vesicles are trapped inside the cell.
- Because no Acetylcholine can be released into the neuromuscular junction, the muscle cannot be told to contract.
Physiological Effect: This results in a descending, systemic flaccid (limp) paralysis of voluntary and autonomic muscles.
Potency: The lethal human dose is approximately 1 nanogram per kilogram (1 ng/kg) intraperitoneally. A single gram of pure, aerosolized botulinum toxin could theoretically kill one million people, making it a Tier 1 high-risk potential bioterrorism agent.
B. Clinical Forms of Botulism
Botulism presents in several distinct clinical paradigms depending entirely on how the patient was exposed to the bacteria or the toxin.
- Foodborne Botulism: Caused by the ingestion of pre-formed toxin in heavily contaminated food. It is classically associated with improperly home-canned alkaline vegetables (like green beans or peppers) or fermented traditional fish products. Because the canning environment is strictly anaerobic, the spores germinate and pump out toxin into the food.
- Presentation: Onset is rapid (12-36 hours post-ingestion). Symptoms start with cranial nerve palsies—famously known as the "4 Ds": Diplopia (double vision), Dysarthria (slurred speech), Dysphonia (difficulty speaking), and Dysphagia (difficulty swallowing). This is followed by ptosis (drooping eyelids) and a rapid, descending flaccid paralysis that ultimately paralyzes the diaphragm, causing respiratory failure. Crucially, there is NO fever (because it is an intoxication, not an active, invasive bacterial infection) and the patient's mental status remains completely clear and alert while they are paralyzed.
- Infant Botulism: The most common form in the United States today. Caused by the ingestion of spores (often from contaminated raw honey, which is why pediatricians forbid honey in children under 1 year of age, or from environmental dust).
- Mechanism: Because an infant under 12 months lacks mature, competitive normal gut flora, the ingested spores find an empty niche. They germinate in the colon, colonize the gut, and produce the toxin in vivo (inside the baby).
- Presentation: "Floppy baby syndrome"—characterized initially by severe constipation (often the very first sign), poor feeding/suckling, weak crying, severe hypotonia (low muscle tone resembling a ragdoll), and progressive muscular weakness.
- Wound Botulism: Caused by spore germination directly deep inside an anaerobic, necrotic wound. Today, it is overwhelmingly associated with intravenous drug abuse, specifically the "skin popping" (subcutaneous injection) of contaminated black tar heroin. The clinical picture is identical to foodborne botulism but has a longer incubation period (up to 14 days) and entirely lacks the gastrointestinal prodromal symptoms (no nausea/vomiting).
- Adult Intestinal Toxemia (Rare): Pathogenically identical to infant botulism, but occurs in adults whose normal, healthy gut flora has been severely decimated by massive surgical bowel alterations or prolonged, heavy broad-spectrum antibiotic therapy, allowing swallowed spores to germinate.
- Iatrogenic Botulism: An accidental overdose of therapeutic injected botulinum toxin (Botox) used for cosmetic purposes, migraines, or severe muscle spasticity disorders (like achalasia or strabismus).
C. Diagnosis and Treatment of Botulism
- Diagnosis: Primarily relies on prompt clinical recognition, as delaying treatment is fatal. Laboratory confirmation utilizes the mouse bioassay (the gold standard, where patient serum, stool, or food extract is injected into live mice to see if they develop paralysis, which is then blocked by type-specific antitoxin). Direct culture of stool or deep wound samples on specialized anaerobic media is also performed.
- Treatment Protocols:
- Toxin Neutralization: Immediate administration of Botulinum antitoxin (an equine heptavalent antitoxin for adults, or human-derived Botulism Immune Globulin [BabyBIG] for infants). The antitoxin strictly neutralizes unbound toxin floating in the blood. It absolutely cannot reverse paralysis caused by toxin that has already entered the nerve terminal.
- Intensive Support: Prolonged mechanical ventilation and parenteral nutrition are often required for weeks to months.
- Surgical Debridement: Essential for wound botulism to physically cut out the dead, anaerobic tissue harboring the bacteria.
💡 The Antibiotic Paradox: A Critical Nursing & Medical Rule
Absolutely NO antibiotics should be given for Infant Botulism or Adult Intestinal Toxemia!
Physiological Expansion: Antibiotics cause massive, violent bacterial lysis (bursting of the bacterial cell wall). If you lyse the actively growing, toxin-producing clostridia in the infant's gut, they will instantly dump a massive, lethal bolus of pre-formed intracellular neurotoxin directly into the baby's bloodstream, severely worsening the paralysis and precipitating sudden respiratory arrest. (Antibiotics are, however, used in wound botulism alongside surgical debridement).
Prognosis: Mortality is 5-10% with rapid, modern supportive care. Recovery is agonizingly slow (taking months) because the cleaved SNARE proteins cannot be repaired by the cell. The paralyzed neuron must physically sprout entirely new axonal branches and form brand new neuromuscular synapses to restore motor function.
IV. Clostridium tetani
Both C. tetani and C. botulinum release 150 kDa zinc metalloprotease exotoxins that act by cleaving SNARE proteins. So why do they cause the exact opposite clinical symptoms?
- Botulinum toxin: Stays locally at the peripheral neuromuscular junction. It blocks excitatory Acetylcholine from motor neurons. Result = Flaccid (limp) paralysis.
- Tetanus toxin: Enters the peripheral nerve but then hijacks the cell's motor system, undergoing retrograde axonal transport all the way backward into the central nervous system (spinal cord). There, it targets and destroys SNARE proteins inside the inhibitory interneurons (Renshaw cells), blocking inhibitory neurotransmitters. Result = Spastic (rigid) paralysis.
A. Tetanus Toxin (Tetanospasmin)
- Structure: An A-B plasmid-encoded 150 kDa neurotoxin remarkably similar in structural blueprint to the botulinum toxin.
- Mechanism of Action:
- The heavy chain binds to gangliosides on somatic motor neurons at the site of the dirty wound.
- Instead of acting locally, it undergoes retrograde axonal transport up the axon, traveling at a rate of roughly 250 mm/day, until it reaches the ventral horn of the spinal cord.
- Once in the spinal cord, it moves into adjacent inhibitory interneurons (specifically Renshaw cells).
- The light chain (zinc metalloprotease) cleaves synaptobrevin.
- This utterly blocks the release of the primary inhibitory neurotransmitters GABA (gamma-aminobutyric acid) and glycine.
- Effect: Without GABA and glycine acting as the "brakes," the lower motor neurons undergo massive disinhibition. They fire continuously and uncontrollably, leading to violent, agonizing spastic (rigid) paralysis and tetanic muscle contractions.
B. Clinical Forms of Tetanus
Spores of C. tetani are universally present in soil and animal feces. Infection requires a penetrating injury (like stepping on a rusty nail, agricultural accidents, or contaminated puncture wounds) that creates a deep, low-oxygen pocket for the spores to germinate.
- Generalized Tetanus: The most common, highly dramatic form.
- Presentation: Begins with Trismus (profound spasm of the masseter muscles, causing 'lockjaw'). Progresses to Risus sardonicus (a creepy, fixed, grimacing sardonic smile due to sustained facial muscle spasms). The back muscles forcefully contract, lifting the patient completely off the bed, a terrifying posture known as Opisthotonus. Generalized, bone-breaking reflex spasms can be triggered violently by minor stimuli (a sudden bright light, a loud noise, or even a light touch).
- Autonomic Instability: The toxin also disinhibits the sympathetic nervous system, causing wild, erratic fluctuations (severe tachycardia, hypertensive crisis, profound diaphoresis/sweating, and cardiac arrhythmias), which is a major cause of death.
- Localized Tetanus: Rigidity isolated entirely to muscles surrounding the local wound site. While generally milder, it is a warning sign that may progress to the generalized, lethal form.
- Cephalic Tetanus: A rare variant involving isolated cranial nerve palsies (often presenting confusingly as facial nerve weakness) occurring shortly after a head, ocular, or facial wound.
- Neonatal Tetanus: A massive global health crisis in developing nations. Occurs via infection of the unhealed, raw umbilical stump. It is overwhelmingly common in neonates born to unimmunized mothers, often where the cord is cut with unsterile instruments (e.g., dirty agricultural blades) or dressed with contaminated materials like cow dung or ash. It presents as an inability to nurse, generalized rigidity, and carries an exceptionally high mortality rate exceeding 90% without modern ICU care.
C. Treatment and Prevention
- Immediate Management: Aggressive wound care, irrigation, and deep surgical debridement to completely eradicate the anaerobic, necrotic environment allowing the bacteria to breed.
- Toxin Neutralization: Immediate administration of human Tetanus Immune Globulin (TIG) directly into the muscle and sometimes injected around the wound. TIG neutralizes any unbound toxin currently floating in the circulation. (Like botulism, it cannot cross the blood-brain barrier and cannot reverse toxin already locked inside the spinal cord neurons).
- Antibiotics: Metronidazole (the absolute drug of choice) is administered intravenously to eliminate the actively growing vegetative organism and halt further toxin production. (Penicillin was historically used but is avoided by some because it acts as a weak GABA-antagonist, theoretically worsening spasms).
- Symptom Control: Heavy muscle relaxants like intravenous diazepam (Valium) or baclofen. In severe, unremitting generalized tetanus, complete neuromuscular blockade (paralysis with drugs like vecuronium) combined with heavy sedation and mechanical ventilation is required for weeks until the central nervous system slowly regenerates new synapses.
- Supportive Care: Keeping the patient isolated in a highly controlled, quiet, pitch-dark room to prevent sensory-triggered violent spasms.
- Vaccination & Prevention: Tetanus is uniquely 100% preventable via active immunization with the formalin-inactivated tetanus toxoid (part of the DTaP/Tdap/Td series). The toxin itself is so highly lethal that the amount required to kill a human is not enough to provoke an immune memory response; therefore, surviving clinical tetanus does NOT grant immunity. You must still be vaccinated after surviving! Proper emergency wound management always includes assessing the immediate need for a vaccine booster and/or TIG based on the patient's documented immunization history.
V. Clostridioides difficile (Formerly Clostridium difficile)
Recently reclassified based on advanced phylogenomic and phenotypic studies into a new genus, C. difficile is the undisputed most common cause of healthcare-associated infectious diarrhea globally, placing a massive financial and morbidity burden on hospital systems.
A. Pathogenesis & Virulence Factors
C. difficile is an opportunistic nightmare. It requires the host's defenses to be breached before it can strike.
- The Trigger (Antibiotic Exposure): The human colon is normally densely packed with a thick forest of healthy bacteria (the microbiome) that outcompetes C. diff for nutrients and produces bile acids that inhibit its growth. When a patient receives broad-spectrum antibiotics (classically Clindamycin, Fluoroquinolones, or 3rd/4th generation Cephalosporins), this healthy flora is wiped out. This massive ecological disruption allows naturally occurring (or nosocomially acquired via the unwashed hands of healthcare workers) C. diff spores to rapidly germinate and overgrow massively in the empty colon.
- Toxin A (Enterotoxin, TcdA): A massive 308 kDa protein. It binds to specific carbohydrate receptors on the apical brush border of enterocytes. It triggers a massive inflammatory cascade, attracting neutrophils and causing severe mucosal damage and massive fluid hypersecretion into the gut lumen (causing the watery diarrhea).
- Toxin B (Cytotoxin, TcdB): A 270 kDa protein that is significantly more potent and destructive than Toxin A. After entering the cell, it heavily glucosylates (adds sugar molecules to) Rho GTPases inside the cell. Rho GTPases control the cell's actin skeleton. Disabling them causes complete, catastrophic cytoskeletal disruption. The cells literally round up, detach from the basement membrane, and undergo rapid apoptosis (programmed cell death).
- Binary Toxin (CDT): An additional toxin produced only by highly virulent strains. It physically ADP-ribosylates cellular actin, further destroying the host cytoskeleton and aiding bacterial adherence to the intestinal wall.
- Hypervirulent Strains: Specifically, the notorious ribotype 027 (NAP1/BI) strain. This specific genetic strain is highly resistant to fluoroquinolones, produces the devastating binary toxin, and possesses a mutation in its tcdC regulatory gene. This broken "off-switch" causes the bacteria to produce vastly higher, uncontrolled amounts of Toxins A and B, leading to massive hospital outbreaks with severe mortality.
C. Difficile Toxins
Remember how the two main toxins work:
- Toxin A is for Apple (Apples go in the Enteric tract). It acts primarily as an Attractant for neutrophils and an Enterotoxin causing fluid release.
- Toxin B is for Bad and Broken. It breaks the actin cytoskeleton. It acts as a severe Cytotoxin causing apoptosis and mucosal necrosis.
B. Clinical Features
- Classic Presentation: Copious, foul-smelling, green, watery diarrhea (defined as ≥ 3 unformed episodes per day), distinct lower abdominal cramping, low-grade fever, and a profoundly elevated white blood cell count in the blood (leukocytosis, often exceeding 15,000 cells/mcL, and sometimes driving a leukemoid reaction up to 50,000 cells/mcL).
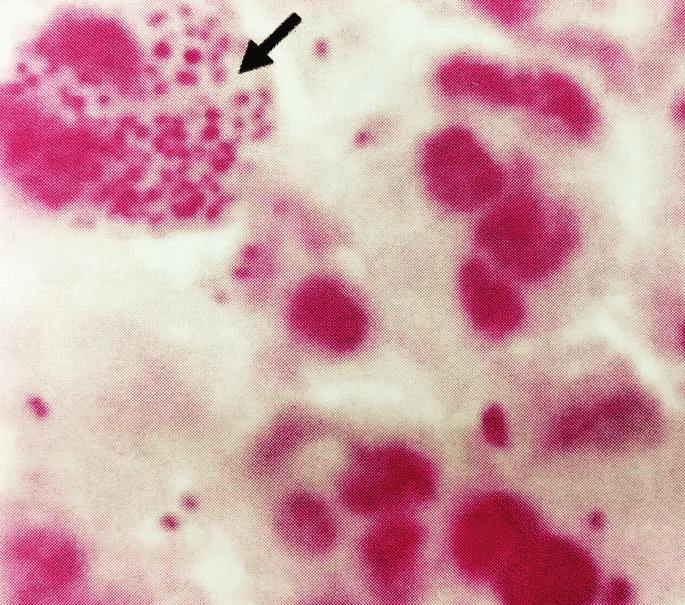
- Pseudomembranous Colitis: Severe, advanced inflammation of the colon. Upon colonoscopy, the gastroenterologist will see pathognomonic raised, yellowish-white plaques scattered across the inflamed, red colonic mucosa. These "pseudomembranes" are actually microscopic volcanos composed of a thick exudate of fibrin, mucin, dead neutrophils, and necrotic cellular debris spewing out from the destroyed mucosal crypts.
- Fulminant Colitis: A life-threatening progression resulting in systemic toxicity. The colon becomes so inflamed and paralyzed that it massively dilates (Toxic Megacolon), posing an imminent risk of transmural bowel perforation, severe fecal peritonitis, and septic shock, carrying a massive mortality rate ranging from 30% to 80%.
- Recurrent Infection: A highly frustrating clinical phenomenon. It occurs in 20-30% of patients shortly after their initial, successful antibiotic treatment finishes. It is rarely due to antibiotic failure, but rather due to the profound resilience of the C. diff spores left behind in the gut, which quickly hatch again before the normal protective gut flora has had time to grow back.
C. Laboratory Diagnosis: The Multi-Step Algorithm
Crucial Diagnostic Rule: You must ONLY test unformed (watery or loose) stools taking the shape of the container. Do not test solid, formed stools (because asymptomatic colonization is common and treating carriers is harmful), and NEVER perform a "test of cure" after a patient finishes treatment, as patients can shed harmless, dead genetic material and inactive spores for weeks.
Testing Modalities:
Glutamate dehydrogenase (GDH) antigen: A highly sensitive, rapid screening test. It confirms the physical presence of the C. diff organism in the stool (because all C. diff bugs secrete GDH). However, its critical flaw is that it cannot differentiate between a non-toxigenic (harmless) strain and a highly toxigenic (lethal) strain. It just proves the bug is there.
Toxin Enzyme Immunoassay (EIA): Directly detects the actively secreted, free Toxins A and/or B floating in the stool. A positive test absolutely proves active, dangerous disease. However, its major flaw is that it suffers from lower clinical sensitivity (it frequently gives false negatives if the toxin level in that specific stool scoop is slightly too low to trigger the chemical reaction).
Nucleic Acid Amplification Test (NAAT/PCR): Directly detects the actual toxin genes (like the tcdB gene) inside the bacterial DNA. It is exquisitely highly sensitive. However, its immense flaw is over-diagnosis; it cannot distinguish between active, toxin-producing disease and asymptomatic colonization (where the bug has the gene, but isn't currently using it to cause disease).
The Modern Two-step Algorithm: This is the global standard of care to balance sensitivity and specificity.
- Step 1: Start by running both the GDH screen + Toxin EIA simultaneously.
- Outcome A: If both are Positive, the patient definitively has active C. diff. Treat them.
- Outcome B: If both are Negative, the patient definitively does not have C. diff. Look for other causes of diarrhea.
- Step 2 (The Tie-Breaker): If the results are discrepant (e.g., GDH is positive meaning the bug is there, but Toxin EIA is negative meaning the test missed the toxin), you must immediately run a NAAT (PCR) to break the tie. If the NAAT is positive for the toxin gene, combined with their clinical symptoms, you diagnose and treat them for C. diff.
Note: Cell culture cytotoxicity assays were historically the absolute gold standard for Toxin B detection, but they require 48-72 hours and living cell lines, making them far too slow and labor-intensive for modern, fast-paced clinical care.
D. Treatment of C. Difficile
- First Episode (Initial Treatment): The universally preferred, first-line therapy is a 10-day course of Oral Fidaxomicin (a highly novel, narrow-spectrum macrolide antibiotic that aggressively kills C. diff while miraculously sparing the normal, healthy gut flora) OR Oral Vancomycin.
Pharmacokinetic Clinical Pearl: You MUST use oral vancomycin, not intravenous (IV). Intravenous vancomycin is a massive molecule that cannot cross the intestinal wall into the gut lumen. Giving it IV will completely miss the bacteria. Giving it orally ensures 100% of the drug stays trapped inside the gut lumen, washing directly over the infected colonic mucosa. Metronidazole, formerly a mainstay, is now heavily deprecated and only used if the primary options are financially or logistically unavailable. - Recurrent Infection: Treated with a complex, extended-pulsed regimen of Fidaxomicin, a heavily tapered/pulsed dose of Vancomycin (designed to kill the vegetative cells, let the spores hatch, and then hit them again over a month), or fundamentally, a Fecal Microbiota Transplantation (FMT). FMT involves taking highly screened, healthy donor feces and instilling it into the patient's colon (via colonoscopy or capsules) to instantly and robustly restore the healthy competing gut flora, achieving cure rates exceeding 90%. Additionally, a monoclonal antibody named Bezlotoxumab (which binds and neutralizes Toxin B) can be infused alongside antibiotics to prevent recurrences.
- Fulminant Colitis (ICU Emergency): Requires maximally aggressive dual therapy: Extremely high-dose Oral Vancomycin (often given via nasogastric tube or directly as a retention enema) PLUS high-dose IV Metronidazole (which can penetrate the inflamed tissue from the blood side). If there is no rapid response, rising serum lactate, or toxic megacolon develops, an emergency, life-saving surgical subtotal colectomy with end ileostomy is absolutely required.
VI. Clostridium perfringens
A non-motile, incredibly rapid-growing (capable of doubling its population every 8-10 minutes under optimal conditions) Clostridium species notorious worldwide for causing devastating, tissue-liquefying infections and widespread food poisoning.
A. Virulence Factors
C. perfringens is a veritable biological weapons factory, producing at least 12 distinct lethal toxins and tissue-destroying enzymes.
- Alpha-toxin (Phospholipase C / Lecithinase): The absolute most important, defining virulence factor. It actively and violently hydrolyzes phosphatidylcholine and sphingomyelin, which are structural pillars found in human eukaryotic cell membranes. This causes massive cell membrane destruction, making the toxin highly hemolytic (bursting red blood cells), necrotic (melting tissue), and causing massive platelet-aggregation (clogging local blood vessels to worsen ischemia).
Laboratory Note: This toxin is demonstrated in the lab using the Nagler reaction, where plating the bacteria on egg yolk agar produces a visible zone of opalescence (due to lecithinase breaking down the yolk lipids), which is specifically blocked by adding anti-alpha-toxin antibody on one half of the plate. It also produces a distinct "double-zone" of hemolysis on blood agar. - Perfringolysin O (Theta-toxin): A powerful, cholesterol-dependent cytolysin that oligomerizes to punch massive, gaping physical holes in host cell membranes.
- Enterotoxin (CPE): A 35 kDa protein that specifically causes severe food poisoning by physically inserting itself and forming massive ion-leaking pores directly in the tight junctions of the intestinal epithelium.
- Beta, Epsilon, and Iota Toxins: Primarily involved in devastating veterinary diseases (like lamb dysentery). C. perfringens is classified into typing schemes (Types A through E) based solely on the unique combination of these major toxins produced by a specific strain. Type A is the dominant human pathogen.
B. Clinical Syndromes
Clostridial Myonecrosis
A rapidly progressive, catastrophically lethal necrosis of deep muscle tissue following severe trauma (crush injuries, motorcycle accidents, deep shrapnel wounds) that introduces spores deep into oxygen-deprived muscle.
- Presentation: Begins with severe, agonizing, out-of-proportion pain at the injury site. The overlying skin rapidly takes on a classic, mottled bronze or deep purple discoloration, erupting with massive, foul-smelling, blood-tinged hemorrhagic bullae (blisters). Profound hypotension, massive intravascular hemolysis, and renal failure rapidly ensue.
- Hallmark Sign: Crepitus. When palpating the skin, the physician will feel a distinct crackling sensation (like bubble wrap) caused by the bacteria rapidly fermenting the muscle carbohydrates and releasing expansive pockets of hydrogen and carbon dioxide gas directly into the tissue planes.
- Treatment: It is an absolute surgical emergency. High-dose IV Penicillin G and Clindamycin (which specifically stops bacterial ribosomes from making more alpha-toxin) are given, but survival dictates urgent, radical surgical excision of all dead muscle, frequently requiring major limb amputation. Hyperbaric oxygen therapy is sometimes used adjunctively to force oxygen into the tissues to halt anaerobic growth.
Clostridial Enterotoxicosis
Caused overwhelmingly by Type A strains producing the heat-labile enterotoxin (CPE) inside the gut. It is classically associated with massive institutional food settings (buffet tables, catered events, prison cafeterias) serving reheated meat and thick poultry gravies.
- Mechanism: The tough spores survive the initial cooking of the meat. If the food is then left out to cool slowly at room temperature, the spores germinate back into vegetative cells and rapidly multiply in the gravy. When the heavily contaminated food is eaten, the bacteria sporulate inside the alkaline environment of the human small intestine, releasing the toxic CPE directly onto the gut wall.
- Presentation: Features an 8-16 hour incubation period. Characterized by severe, crampy abdominal pain and copious, watery diarrhea. Notably, there is typically NO vomiting and NO fever (which helps distinguish it from Staph aureus or Bacillus cereus food poisoning). It is highly self-limiting and resolves entirely on its own within 24-48 hours. No antibiotics are needed.
"Pigbel" Disease
A severe, fulminant, and often fatal disease caused by Type C strains producing the devastating beta-toxin, which completely liquefies segments of the small intestine.
- Historical Clinical Context: Famously documented occurring in local populations in Papua New Guinea during cultural feasts. It follows the massive consumption of undercooked, contaminated pork combined heavily with sweet potatoes. The sweet potatoes contain a powerful, natural trypsin inhibitor. Because human trypsin normally digests and destroys the bacterial beta-toxin, the sweet potato effectively shields the toxin, allowing it to destroy the bowel, causing horrific bloody diarrhea, bowel perforation, and high mortality.
VII. Gram-Positive Anaerobic Cocci (GPAC)
Moving away from the deadly bacilli, we turn our attention to the obligate anaerobic cocci, which are clinically highly significant, heavily playing a major role in opportunistic, deep-seated mixed infections.
- Taxonomy & Reclassification: Historically, these organisms were carelessly lumped together under the catch-all genus Peptostreptococcus. However, based on modern 16S rRNA genetic sequencing, they have now been highly differentiated and reclassified into multiple distinct genera, including the most clinically prominent: Finegoldia (specifically F. magna, the most pathogenic of the group), Anaerococcus, Peptoniphilus, and Parvimonas.
- Normal Flora Ecosystem: They are ubiquitous, harmless commensals, forming a heavy, protective part of the normal flora of the human skin, the oral cavity/mouth, the gastrointestinal (GI) tract, and the genitourinary (GU) tract.
- Pathogenesis & Clinical Significance:
- They almost never cause disease acting alone. They are notoriously, aggressively involved in mixed (polymicrobial) infections.
- Physiological Expansion (Synergism): How do obligate anaerobes survive in a skin wound exposed to the air? In deep traumatic wounds or bite wounds, facultative aerobic bacteria (like Staph or Strep) rapidly consume all the available oxygen in the local tissue. This creates a perfect, highly reduced, oxygen-free local microenvironment deep inside the wound, allowing the anaerobic GPACs to thrive, multiply, and secrete tissue-destroying enzymes.
- Clinical Examples: They are the primary culprits in massive, foul-smelling polymicrobial abscesses, severe diabetic foot ulcers, brutal human and animal bite wounds, brain abscesses (spreading from dental infections), necrotizing fasciitis, and deep-seated intra-abdominal/pelvic inflammatory disease (PID). The pus from these infections is notoriously foul-smelling, directly due to the bacteria producing short-chain fatty acids during anaerobic fermentation.
- Laboratory Identification:
- They are notoriously finicky and slow-growing on anaerobic blood agar plates, taking up to 48-72 hours to form small, convex, grey/white colonies.
- Gram stain reveals Gram-positive cocci arranged in distinct chains or massive, irregular clusters.
- Biochemically, they are characteristically resistant to sodium polyanethol sulfonate (SPS) (with the exception of Peptostreptococcus anaerobius, which is sensitive), a highly useful diagnostic trait which helps microbiologists distinguish them rapidly in the clinical lab.
❓ End of Module Review Question
Case: A 72-year-old hospital patient who was recently treated with a prolonged course of IV clindamycin for a severe diabetic foot infection develops severe, foul-smelling, watery diarrhea (8 times a day), lower abdominal cramping, and a markedly high white blood cell count of 18,000 cells/mcL. An urgent C. diff stool testing algorithm is ordered.
Question: The laboratory quickly reports that the Glutamate Dehydrogenase (GDH) test is POSITIVE, but the Toxin EIA test is returned as NEGATIVE. What does this exact combination mean pathologically, and what is the absolute next mandatory step according to the standard clinical algorithm?
Answer: The positive GDH test definitively proves that the physical cellular bodies of the C. difficile bacteria are present in the patient's colon. However, the negative Toxin EIA means the lab chemically failed to detect any actively secreted, free-floating toxin in that specific stool sample. Because the EIA test is notorious for lacking high sensitivity (false negatives are common), this is categorized as a discrepant result. The next absolute mandatory step is to run a NAAT (PCR) targeting the specific toxin gene (tcdB) acting as a tie-breaker. If the PCR confirms the gene is present, considering the patient's severe clinical symptoms, you officially diagnose toxigenic C. diff infection and immediately initiate Oral Vancomycin or Fidaxomicin therapy.
References & Recommended Clinical Reading
- Bennett, J. E., Dolin, R., & Blaser, M. J. (2019). Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases (9th ed.). Elsevier.
- Murray, P. R., Rosenthal, K. S., & Pfaller, M. A. (2020). Medical Microbiology (9th ed.). Elsevier.
- Infectious Diseases Society of America (IDSA) & Society for Healthcare Epidemiology of America (SHEA). (2021). Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children.
- Centers for Disease Control and Prevention (CDC). (2022). Botulism: Clinical Guidelines and Treatment Protocols.
- Centers for Disease Control and Prevention (CDC). (2023). Tetanus: For Clinicians.
- Levinson, W., Chin-Hong, P., Joyce, E. A., Nussbaum, J., & Schwartz, B. (2020). Review of Medical Microbiology and Immunology (16th ed.). McGraw-Hill Education.
Quick Quiz
Bacteriology Intro Quiz
Microbiology - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
Bacteriology Intro Quiz
Microbiology
Preparing questions...
Choose your answer and keep your streak alive.
Great effort.
Here is your quick performance summary.
Clostridia and Gram-Positive Anaerobic Cocci Read More »