Cholesterol Metabolism Pathway
Cholesterol Metabolism
Cholesterol often gets a bad rap due to its association with heart disease, but it's crucial to understand that it is an essential molecule for life. Our bodies need cholesterol to function properly. The problem arises when its levels are imbalanced or when it's handled improperly within the body.
Importance and Physiological Functions of Cholesterol
Cholesterol is a lipid belonging to the steroid family. Its unique amphipathic structure (a polar hydroxyl group and a nonpolar steroid ring system and hydrocarbon tail) allows it to insert into cell membranes, giving it critical structural and signaling roles.
- Essential Component of Cell Membranes:
- Cholesterol is a major constituent of virtually all animal cell membranes.
- It modulates membrane fluidity, permeability, and stability, acting as a "buffer": at high temperatures, it stiffens the membrane, while at low temperatures, it prevents rigidity.
- It is particularly abundant in myelin sheaths, enhancing nerve signal transmission.
- Precursor for Steroid Hormones:
- Cholesterol is the obligate precursor for all five major classes of steroid hormones: Glucocorticoids (e.g., Cortisol), Mineralocorticoids (e.g., Aldosterone), Androgens (e.g., Testosterone), Estrogens (e.g., Estradiol), and Progestogens (e.g., Progesterone).
- Precursor for Bile Acids (and Bile Salts):
- In the liver, cholesterol is converted into primary bile acids.
- Bile acids emulsify dietary fats in the small intestine, facilitating their absorption. This is the primary way the body eliminates excess cholesterol.
- Precursor for Vitamin D Synthesis:
- 7-Dehydrocholesterol, a precursor in the cholesterol synthesis pathway, is converted to pre-vitamin D3 in the skin upon exposure to UV light.
- This is then converted to the active hormone, calcitriol, essential for calcium homeostasis.
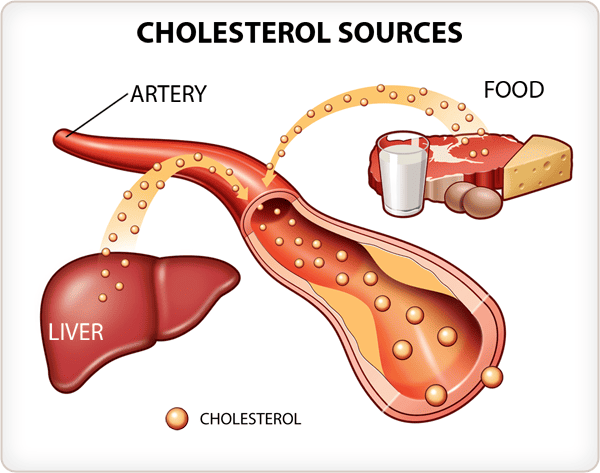
Sources of Cholesterol
The body acquires cholesterol from two main sources:
- Endogenous Synthesis (De Novo Synthesis):
- The vast majority of cholesterol (about 80%) is synthesized internally, primarily in the liver (~50% of total synthesis), but also in the intestine, adrenal cortex, and reproductive organs.
- Dietary Intake (Exogenous Cholesterol):
- Cholesterol is consumed in the diet, found exclusively in animal products (meat, eggs, dairy). Plant foods do not contain cholesterol.
- The amount absorbed can vary significantly among individuals.
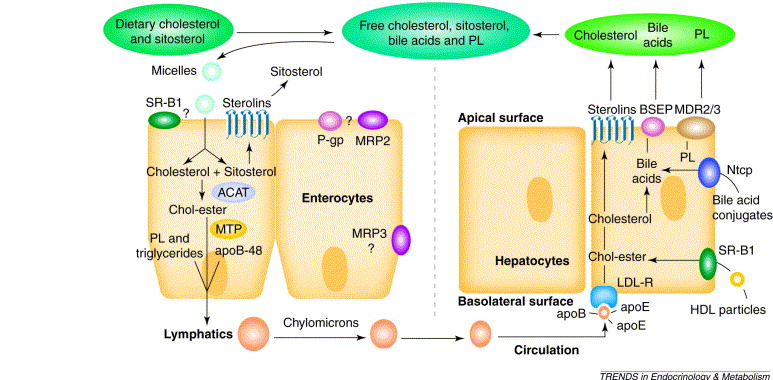
Absorption of Dietary Cholesterol
The process of dietary cholesterol absorption primarily occurs in the small intestine:
- Emulsification: Dietary cholesterol esters are emulsified by bile salts into smaller micelles.
- Hydrolysis: Cholesterol Esters (CE) are hydrolyzed into free cholesterol (FC) by pancreatic cholesterol esterase. Only free cholesterol can be absorbed.
- Micelle Formation: Free cholesterol and other digested lipids become incorporated into mixed micelles with bile salts.
- Uptake by Enterocytes:
- Mixed micelles diffuse to the brush border of the intestinal enterocytes.
- The primary transporter responsible for cholesterol uptake is the Niemann-Pick C1-Like 1 (NPC1L1) protein. This transporter is the target of the drug ezetimibe.
- Intracellular Processing and Re-esterification:
- Once inside the enterocyte, free cholesterol can be either effluxed back into the lumen via ABC G5/G8 transporters or re-esterified to cholesterol esters by the enzyme Acyl-CoA Cholesterol Acyltransferase 2 (ACAT2).
- Chylomicron Assembly and Secretion:
- The newly formed cholesterol esters and re-formed triacylglycerols are packaged with apolipoproteins (primarily apoB-48) into large lipoprotein particles called chylomicrons.
- Chylomicrons are then released into the lymphatic system, which eventually drains into the bloodstream.
Summary
So, to summarize, cholesterol is a vital molecule for cell structure, hormones, bile acids, and Vitamin D. We get it from both our diet and internal synthesis. Dietary cholesterol is absorbed in the small intestine via NPC1L1, processed, and then packaged into chylomicrons for transport.
Pathways of Cholesterol Synthesis (De Novo Synthesis)
Cholesterol is an indispensable molecule, and while we obtain some from our diet, the human body possesses the remarkable ability to synthesize nearly all the cholesterol it requires through a complex process known as de novo synthesis. This internal production ensures a constant supply for vital cellular functions.
Sites of Synthesis:
While virtually all nucleated cells can synthesize cholesterol, certain tissues are particularly active:
- The liver is the predominant site, responsible for approximately 50% of the body's synthesis.
- Other significant contributors include the intestine, the adrenal cortex, and the testes and ovaries.
Cellular Location of Enzymes:
The enzymatic machinery is distributed between two key cellular compartments:
- Enzymes for the initial stages are found in the cytoplasm.
- Enzymes for later stages are located within the membranes of the endoplasmic reticulum.
Requirements for Cholesterol Biosynthesis:
The synthesis of cholesterol is an energetically demanding process:
- Carbon Atoms: All 27 carbon atoms are derived from Acetyl-CoA. A total of 18 molecules are consumed.
- Reducing Equivalents: The process requires significant reducing power, supplied by NADPH (approx. 16 moles).
- Energy: The process requires considerable energy from ATP (approx. 36 moles).
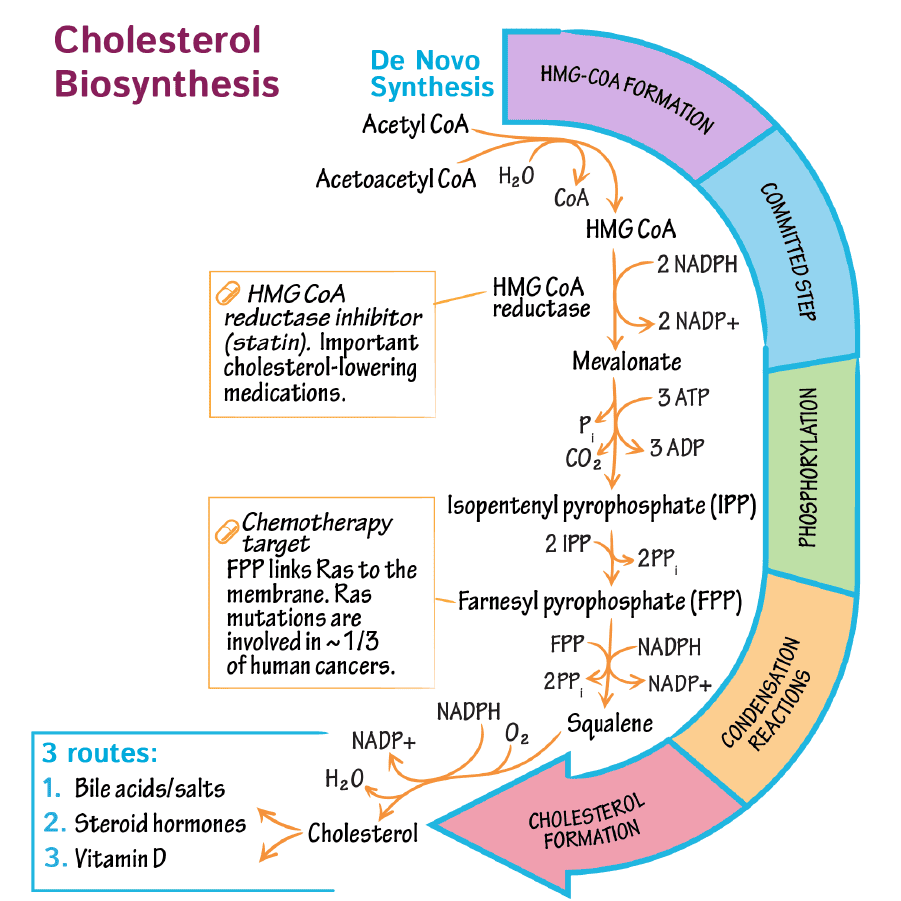
Steps of Cholesterol Biosynthesis: A Detailed Pathway
The complex pathway can be delineated into five principal stages:
Step 1: Formation of HMG-CoA
The synthesis initiates with the condensation of Acetyl-CoA units:
- Two molecules of Acetyl-CoA combine to form Acetoacetyl-CoA (catalyzed by thiolase).
- Acetoacetyl-CoA condenses with a third molecule of Acetyl-CoA to yield β-hydroxy-β-methylglutaryl-CoA (HMG-CoA), catalyzed by HMG-CoA synthase.
It is crucial to note the distinction from ketone body synthesis: the cytosolic HMG-CoA synthase produces HMG-CoA for cholesterol synthesis, while the mitochondrial HMG-CoA synthase participates in ketogenesis. This segregation ensures the pathways operate independently.
Step 2: Conversion of HMG-CoA to Mevalonate
This stage represents the rate-limiting and committed step in cholesterol biosynthesis:
- HMG-CoA is reduced to mevalonate in a reaction catalyzed by HMG-CoA reductase.
- This endoplasmic reticulum-bound enzyme requires two molecules of NADPH.
- HMG-CoA reductase is the primary therapeutic target for statins, a class of drugs that lower plasma cholesterol.
Step 3: Production of Activated Isoprenoid Units
Mevalonate is subsequently processed to generate activated 5-carbon units:
- Mevalonate undergoes a series of three phosphorylation steps, utilizing ATP.
- This is followed by decarboxylation to produce isopentenyl pyrophosphate (IPP), a 5-carbon isoprenoid unit.
- IPP can be isomerized to its structural cousin, dimethylallyl pyrophosphate (DMAPP).
Step 4: Synthesis of Squalene
The activated 5-carbon isoprenoid units are progressively linked:
- DMAPP condenses with IPP to form the 10-carbon geranyl pyrophosphate (GPP).
- GPP condenses with another IPP to yield the 15-carbon farnesyl pyrophosphate (FPP).
- Finally, two molecules of FPP condense head-to-head, mediated by squalene synthase and requiring NADPH, to form the 30-carbon linear molecule squalene.
Step 5: Conversion of Squalene to Cholesterol
The linear squalene molecule undergoes cyclization and a series of modifications:
- Squalene is first oxidized to squalene epoxide by squalene monooxygenase.
- Squalene epoxide undergoes a complex cyclization reaction to form lanosterol, the first true steroid compound in the pathway.
- From lanosterol, a multi-step process involving ~19 enzymatic reactions ensues, involving:
- Demethylation: Removal of three methyl groups, reducing the carbon count from 30 to 27.
- Double Bond Rearrangement: Shifts in the positions of double bonds.
- Reduction: Reduction of a double bond in the side chain.
These precise modifications culminate in the formation of cholesterol.
Regulation of Cholesterol Synthesis
The synthesis of cholesterol is a highly regulated process. The primary point of control is the enzyme HMG-CoA reductase, the rate-limiting step in the pathway. Regulation occurs through several sophisticated mechanisms:
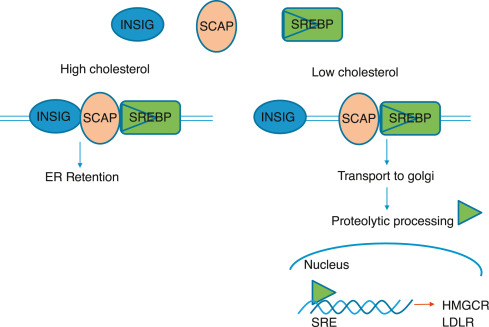
Transcriptional Control (Feedback Inhibition via SREBP Pathway):
- This is the most critical long-term regulatory mechanism.
- When intracellular cholesterol levels are high, they reduce the activity of SREBP-2 (Sterol Regulatory Element-Binding Protein 2).
- This leads to a reduction in the transcription of genes encoding HMG-CoA reductase and the LDL receptor, thus diminishing cholesterol synthesis.
- Conversely, low cellular cholesterol levels activate SREBP-2, promoting gene transcription and increasing both cholesterol synthesis and uptake.
Translational Control:
High concentrations of cholesterol also exert an inhibitory effect on the translation of HMG-CoA reductase mRNA, directly reducing the quantity of enzyme synthesized.
Enzyme Degradation (Proteolysis):
High sterol levels induce a conformational change in the reductase enzyme, making it more susceptible to ubiquitination and subsequent degradation by the proteasome. This shortens the enzyme's lifespan, leading to a quick reduction in its activity.
Covalent Modification (Hormonal Regulation and Energy Status):
HMG-CoA reductase exists in two interconvertible forms:
- Dephosphorylated form: More active.
- Phosphorylated form: Less active (inactive).
Phosphorylation is primarily mediated by AMP-activated protein kinase (AMPK), which is activated when cellular ATP is low. By phosphorylating and inactivating HMG-CoA reductase, AMPK conserves cellular energy.
Hormonal Influence:
- Insulin and Thyroid Hormones: Increase HMG-CoA reductase activity by promoting dephosphorylation (activation).
- Glucagon and Glucocorticoids: Decrease HMG-CoA reductase activity by promoting phosphorylation (inactivation).
Direct Inhibition by Drugs (Statins):
- Drugs such as lovastatin, simvastatin, and atorvastatin are competitive inhibitors of HMG-CoA reductase.
- They structurally resemble HMG-CoA and bind to the active site, blocking its ability to convert HMG-CoA to mevalonate and directly reducing the rate of cholesterol synthesis.
Inhibition by Bile Acids:
Bile acids, which are derivatives of cholesterol, can also contribute to feedback regulation by inhibiting HMG-CoA reductase activity.
Connecting to Cholesterol Transport:
While not a direct regulatory mechanism for synthesis, the major players in cholesterol transport are intrinsically linked to overall cholesterol homeostasis:
- Low-Density Lipoproteins (LDL): Primarily transport cholesterol from the liver to peripheral tissues. Often called "bad cholesterol."
- High-Density Lipoproteins (HDL): Transport excess cholesterol from peripheral tissues back to the liver for excretion or recycling (reverse cholesterol transport). Often called "good cholesterol."
Formation and Excretion of Bile Acids and Bile Salts
Bile acids are a family of steroid acids that represent the major catabolic products of cholesterol in the body. Their primary physiological function is to facilitate the digestion and absorption of dietary fats and fat-soluble vitamins in the small intestine. They also play a crucial role in cholesterol homeostasis by being the principal route for cholesterol excretion.
What is Bile?
Bile is a complex, watery, yellowish-green fluid produced by the liver. It consists of a watery mixture of organic and inorganic compounds.
The quantitatively most important organic components of bile are phosphatidylcholine (lecithin) and conjugated bile salts.
Bile can either pass directly from the liver into the duodenum (the first part of the small intestine) via the common bile duct, or it can be stored and concentrated in the gallbladder when not immediately needed for digestion.
A. Synthesis of Primary Bile Acids
The synthesis of bile acids, known as cholic acid and chenodeoxycholic acid, occurs exclusively in the liver. This multi-step pathway converts the hydrophobic cholesterol molecule into more polar, amphipathic bile acids, making them water-soluble.
Initiation - The Rate-Limiting Step:
The synthesis pathway involves the insertion of hydroxyl groups at specific positions on the steroid structure of cholesterol. The hydrocarbon chain is also shortened by three carbons.
The first and rate-limiting step in bile acid synthesis is the introduction of a hydroxyl group at carbon 7 of cholesterol, forming 7α-hydroxycholesterol.
This reaction is catalyzed by the enzyme cholesterol 7α-hydroxylase (CYP7A1).
CYP7A1 is a cytochrome P450 enzyme, requiring molecular oxygen (O₂) and NADPH.
Regulation: The activity of CYP7A1 is highly regulated. It is inhibited by bile acids (a feedback mechanism) and induced by cholesterol (when cholesterol levels are high). This ensures that bile acid synthesis is responsive to both bile acid demand and cholesterol availability.
Subsequent Reactions:
Following the initial hydroxylation, 7α-hydroxycholesterol undergoes a series of additional modifications. These steps involve:
- Further hydroxylations (e.g., at C-12 to form cholic acid, which is a triol - having three hydroxyl groups).
- Epimerization of the 3β-hydroxyl group to a 3α-hydroxyl group.
- Reduction of the double bond in the B ring.
- Oxidation of the side chain (carbon atoms 24, 25, 26, and 27) and its cleavage to introduce a carboxyl group at C-24, shortening the side chain from 8 to 5 carbons.
Formation of Primary Bile Acids:
These reactions ultimately lead to the formation of the two primary bile acids:
- Cholic acid: (a triol) Has hydroxyl groups at C-3α, C-7α, and C-12α.
- Chenodeoxycholic acid: (a diol) Has hydroxyl groups at C-3α and C-7α.
B. Conjugation of Primary Bile Acids to Form Bile Salts
To significantly improve their ability to emulsify fat and enhance their water solubility, primary bile acids are further modified in the liver through a process called conjugation. They are joined with either the amino acid glycine or taurine.
Mechanism:
The carboxyl group (–COOH) at the end of the bile acid side chain forms an amide bond with the amino group (–NH₂) of glycine or taurine.
This reaction is catalyzed by bile acid-CoA ligase (which activates the bile acid by forming a CoA thioester) and bile acid-CoA:amino acid N-acyltransferase.
Resulting Conjugated Bile Acids (Bile Salts):
This generates the conjugated bile acids:
- Taurocholic acid and Taurochenodeoxycholic acid
- Glycocholic acid and Glycocholic acid
These conjugated forms are all necessary to give bile its essential function in fat digestion.
At physiological pH, these conjugated bile acids exist as anions (negatively charged) due to the low pKa of their conjugates. Therefore, they are referred to as bile salts (e.g., taurocholate, glycocholate). The term "bile salts" specifically refers to these ionized forms.
Physiological Significance of Conjugation:
- Increased Solubility & Emulsification: Conjugation makes bile acids much more soluble and improves their amphipathic nature, crucial for emulsifying dietary fats.
- Effective Detergency: The salts are large, negatively charged ions that are not readily absorbed by passive diffusion in the upper region of the small intestine, ensuring sustained activity.
- PKA Reduction: Conjugation lowers the pKa of the bile acids, ensuring that they remain ionized (charged) even in the acidic environment of the upper small intestine.
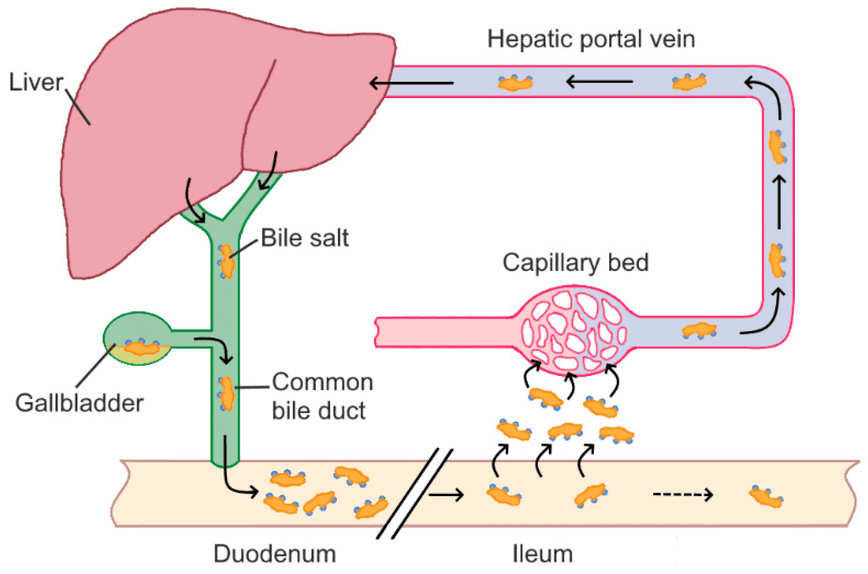
C. Enterohepatic Circulation of Bile Salts
Bile salts are essential for fat digestion, but the body has a highly efficient system to conserve them rather than synthesizing new ones for every meal. This system is called the enterohepatic circulation.
Secretion:
Synthesized and conjugated bile salts are secreted from the liver, stored in the gallbladder, and released into the duodenum after a fatty meal.
Function in Small Intestine:
In the duodenum and jejunum, bile salts emulsify dietary fats and form mixed micelles.
Reabsorption:
A remarkable 95% of bile salts are reabsorbed in the ileum (the final part of the small intestine). This reabsorption occurs via a specialized, active transport system known as the apical sodium-dependent bile acid transporter (ASBT) in the ileal enterocytes. Some passive reabsorption of unconjugated bile acids can also occur in the jejunum and colon.
Portal Vein Transport:
Once reabsorbed, bile salts enter the portal venous blood and are transported back to the liver, mostly bound to albumin.
Hepatic Uptake:
The liver efficiently extracts the bile salts from the portal blood via specific transporters.
Recycling:
The liver then re-secretes these reabsorbed bile salts into the bile, completing the circulation. This cycle can occur 4-12 times a day.
D. Formation and Excretion of Secondary Bile Acids
Not all bile acids are reabsorbed directly. Bacterial action in the gut leads to the formation of secondary bile acids.
Bacterial Deconjugation:
As bile salts travel through the colon, intestinal bacteria can deconjugate them, removing glycine or taurine.
Bacterial Dehydroxylation:
These free primary bile acids can then be further metabolized by gut bacteria, specifically undergoing 7α-dehydroxylation. This results in the formation of secondary bile acids:
- Deoxycholic acid (from cholic acid)
- Lithocholic acid (from chenodeoxycholic acid)
Fate of Secondary Bile Acids:
Most secondary bile acids are also reabsorbed and return to the liver. In the liver, deoxycholic acid can be re-conjugated. Lithocholic acid, which is less soluble, is often sulfonated before being secreted back into bile, which aids in its excretion.
E. Excretion of Cholesterol
The excretion of cholesterol from the body primarily occurs via two main routes:
- Conversion to Bile Acids and Excretion: A small fraction of bile salts (about 5%, or 0.2-0.6 grams per day) is not reabsorbed and is instead excreted in the feces. This represents a net loss and is the most significant route for cholesterol elimination.
- Direct Secretion of Unesterified Cholesterol into Bile: The liver can also secrete free, unesterified cholesterol directly into the bile. A portion of this is reabsorbed, but a significant amount is excreted. If the concentration of cholesterol in bile exceeds the solubilizing capacity of bile salts, it can precipitate, leading to cholesterol gallstones.
Synthesis of Steroid Hormones
Cholesterol is not merely a structural component of cell membranes or a precursor for bile acids; it is also the obligate precursor for all steroid hormones. These powerful signaling molecules regulate a vast array of physiological processes, including metabolism, inflammation, immune responses, salt and water balance, sexual development, and reproduction.
A. General Pathway for Steroid Hormone Synthesis
The synthesis of all steroid hormones follows a common, fundamental pathway that begins with cholesterol. This process primarily occurs in the mitochondria and endoplasmic reticulum of steroidogenic tissues.
Tissue-Specific Synthesis:
While virtually all cells contain cholesterol, steroid hormone synthesis is restricted to specialized endocrine tissues, including:
- Adrenal cortex: Produces glucocorticoids, mineralocorticoids, and some adrenal androgens.
- Gonads (Testes and Ovaries): Produce androgens, estrogens, and progestins.
- Placenta: Produces estrogens and progestins during pregnancy.
Rate-Limiting Step: Transport into Mitochondria:
- The first and rate-limiting step is the transport of cholesterol from the cytoplasm into the inner mitochondrial membrane.
- This transport is mediated by the Steroidogenic Acute Regulatory protein (StAR). StAR's activity is rapidly regulated by tropic hormones (e.g., ACTH, LH).
Initial Conversion: Cholesterol to Pregnenolone:
- Once inside the inner mitochondrial membrane, cholesterol is converted to pregnenolone.
- This is catalyzed by the cholesterol desmolase complex, also known as P450scc (cytochrome P450 side-chain cleavage enzyme), which requires NADPH and O₂.
- Pregnenolone is the universal precursor for all other steroid hormones.
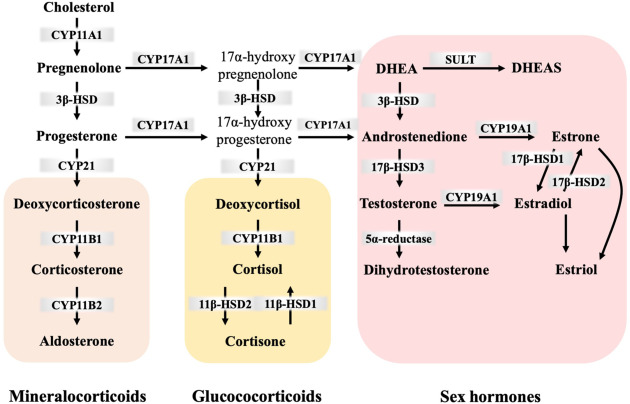
B. Major Classes of Steroid Hormones
From pregnenolone, the pathway diverges. The specific hormones produced depend on the enzymatic machinery present in the particular tissue.
Progestins (C21 Steroids):
- Progesterone is derived directly from pregnenolone.
- Function: Crucial for maintaining pregnancy and regulating the menstrual cycle.
- Primary site of synthesis: Ovaries (corpus luteum), adrenal cortex, placenta.
Glucocorticoids (C21 Steroids):
- Cortisol is the primary human glucocorticoid.
- Pathway: Pregnenolone → Progesterone → ... → Cortisol.
- Function: Regulates metabolism, suppresses immune responses, reduces inflammation, and helps adapt to stress.
- Primary site of synthesis: Adrenal cortex (zona fasciculata).
Mineralocorticoids (C21 Steroids):
- Aldosterone is the most potent human mineralocorticoid.
- Pathway: Pregnenolone → Progesterone → ... → Aldosterone.
- Function: Regulates electrolyte balance by promoting sodium reabsorption and potassium excretion, thus influencing blood pressure.
- Primary site of synthesis: Adrenal cortex (zona glomerulosa).
Androgens (C19 Steroids):
- Dehydroepiandrosterone (DHEA), Androstenedione, and Testosterone are key androgens.
- Function: Responsible for the development of male secondary sexual characteristics and libido in both sexes.
- Primary site of synthesis: Testes, adrenal cortex, ovaries.
Estrogens (C18 Steroids):
- Estradiol is the most potent and abundant human estrogen.
- Pathway: Estrogens are synthesized from androgens (testosterone or androstenedione) through a reaction catalyzed by the enzyme aromatase.
- Function: Responsible for the development of female secondary sexual characteristics and regulation of the menstrual cycle.
- Primary site of synthesis: Ovaries, placenta, adipose tissue, testes (to a lesser extent).
C. Regulation of Steroid Hormone Synthesis
The synthesis is tightly regulated by the hypothalamic-pituitary-adrenal/gonadal axes.
- Tropic Hormones: Specific peptide hormones from the anterior pituitary stimulate target endocrine glands:
- Adrenocorticotropic hormone (ACTH): Stimulates the adrenal cortex (cortisol).
- Luteinizing hormone (LH): Stimulates testosterone production in testes and progesterone in ovaries.
- Follicle-stimulating hormone (FSH): Stimulates estrogen production by ovarian follicles.
- Feedback Inhibition: High levels of circulating steroid hormones typically exert negative feedback on the hypothalamus and pituitary gland.
- Enzyme Specificity: The expression and activity of specific steroidogenic enzymes (e.g., 21-hydroxylase, aromatase) within different tissues dictate which hormones are produced. Genetic deficiencies can lead to disorders like congenital adrenal hyperplasia.
Transport of Cholesterol by Lipoproteins
Cholesterol, being a lipid, is largely insoluble in the aqueous environment of blood plasma. To be efficiently transported between tissues for synthesis, utilization, and excretion, cholesterol (along with other lipids like triglycerides and phospholipids) is packaged into complex particles called lipoproteins. These molecular transporters have a hydrophilic exterior and a hydrophobic core, allowing them to carry lipids through the bloodstream.
Cholesteryl ester in the diet is hydrolyzed to cholesterol, which is then absorbed by the intestine together with dietary unesterified cholesterol and other lipids. It is then incorporated into chylomicrons.
Ninety-five percent of the chylomicron cholesterol is delivered to the liver in chylomicron remnants. Most of the cholesterol secreted by the liver in VLDL is retained during the formation of IDL and ultimately LDL, which is taken up by the LDL receptor in liver and extrahepatic tissues.
A. Structure of Lipoproteins
All lipoproteins share a common structural organization:
- Hydrophobic Core: Contains the most water-insoluble lipids:
- Triglycerides (TGs)
- Cholesteryl esters (CEs)
- Hydrophilic Shell: Surrounds the core and allows the particle to be soluble in blood:
- Phospholipids
- Free (unesterified) Cholesterol
- Apolipoproteins: Proteins integral to the shell that provide structural integrity, act as enzyme cofactors (e.g., ApoC-II), and serve as ligands for cell surface receptors (e.g., ApoB-100).
B. Classes of Lipoproteins
Lipoproteins are classified based on their density (more lipid = less dense). From largest/least dense to smallest/most dense, the main classes are:
Chylomicrons (CM):
- Origin: Intestine.
- Primary Lipid: Dietary triglycerides (>80%).
- Main Apolipoproteins: ApoB-48, ApoC-II, ApoE.
- Function: Transport dietary (exogenous) lipids from the intestine to peripheral tissues and then to the liver.
- Metabolism: Nascent chylomicrons acquire ApoC-II and ApoE from HDL. ApoC-II activates lipoprotein lipase (LPL) in capillaries, which hydrolyzes TGs. The resulting chylomicron remnants, enriched in cholesteryl esters and ApoE, are taken up by the liver.
Very Low-Density Lipoproteins (VLDL):
- Origin: Liver.
- Primary Lipid: Endogenously synthesized triglycerides (50-60%).
- Main Apolipoproteins: ApoB-100, ApoC-II, ApoE.
- Function: Transport endogenously synthesized lipids from the liver to peripheral tissues.
- Metabolism: Similar to chylomicrons, LPL hydrolyzes TGs from VLDL. As VLDL loses TGs, it becomes smaller and denser, first forming intermediate-density lipoproteins (IDL).
Intermediate-Density Lipoproteins (IDL):
- Origin: Formed from VLDL after triglyceride hydrolysis.
- Primary Lipid: Roughly equal amounts of TGs and cholesteryl esters.
- Main Apolipoproteins: ApoB-100, ApoE.
- Function: An intermediate in the conversion of VLDL to LDL. About half are taken up by the liver, and the rest are metabolized to LDL.
Low-Density Lipoproteins (LDL):
- Origin: Primarily from the catabolism of VLDL and IDL.
- Primary Lipid: Cholesteryl esters (~45-50%).
- Main Apolipoprotein: ApoB-100.
- Function: Transport cholesterol from the liver to peripheral tissues. Often called "bad cholesterol."
- Metabolism: Cells needing cholesterol take up LDL particles via the LDL receptor, which specifically recognizes ApoB-100.
High-Density Lipoproteins (HDL):
- Origin: Liver and intestine.
- Primary Lipid: Relatively rich in protein (~50%) and phospholipids.
- Main Apolipoproteins: ApoA-I (major), ApoC-II, ApoE.
- Function: Often called "good cholesterol." HDL plays a crucial role in reverse cholesterol transport, collecting excess cholesterol from peripheral cells and transporting it back to the liver. It also serves as a reservoir for ApoC-II and ApoE.
- Metabolism: Nascent HDL particles acquire free cholesterol from peripheral cells. This cholesterol is esterified by lecithin-cholesterol acyltransferase (LCAT). Mature HDL can exchange cholesteryl esters for TGs with other lipoproteins (via CETP) and is finally taken up by the liver (via SR-B1).
C. Exogenous vs. Endogenous Pathways of Lipid Transport
- Exogenous Pathway: Deals with dietary lipids. Chylomicrons are the key lipoproteins.
- Endogenous Pathway: Deals with endogenously synthesized lipids. VLDL, IDL, and LDL are the main players for distribution, while HDL mediates reverse transport.
D. Role of Key Enzymes and Receptors
- Lipoprotein Lipase (LPL): Hydrolyzes TGs in chylomicrons and VLDL in capillaries.
- Hepatic Lipase (HL): Hydrolyzes TGs and phospholipids in IDL and HDL.
- Lecithin-Cholesterol Acyltransferase (LCAT): Esterifies free cholesterol to cholesteryl esters within HDL.
- Cholesteryl Ester Transfer Protein (CETP): Facilitates the exchange of cholesteryl esters and TGs between lipoproteins.
- LDL Receptor: Mediates the uptake of LDL (and IDL) via recognition of ApoB-100.
- Scavenger Receptor Class B Type 1 (SR-B1): Mediates selective uptake of cholesteryl esters from HDL by the liver.
Regulation of Cholesterol Synthesis, Metabolism, and Transport
Maintaining cholesterol homeostasis is critical. The body employs an intricate network of regulatory mechanisms, with the primary point of control being the enzyme HMG-CoA reductase.
A. Regulation of Cholesterol Synthesis
Transcriptional Control (Gene Expression):
- SREBP-2 (Sterol Regulatory Element-Binding Protein-2): This is the master regulator.
- Low Cellular Cholesterol: SREBP-2 is cleaved, moves to the nucleus, and binds to Sterol Regulatory Elements (SREs). This activates transcription of genes for HMG-CoA reductase and the LDL receptor, increasing both cholesterol production and uptake.
- High Cellular Cholesterol: SREBP-2 is retained in the ER, and transcription is suppressed.
Post-Translational Control (Enzyme Activity & Degradation):
- Phosphorylation (Covalent Modification):
- AMP-activated protein kinase (AMPK): When cellular energy is low, AMPK phosphorylates and inactivates HMG-CoA reductase.
- Insulin: Promotes dephosphorylation, activating the enzyme.
- Glucagon: Promotes phosphorylation, inactivating the enzyme.
- Proteasomal Degradation: High levels of cholesterol cause HMG-CoA reductase to be degraded by the proteasome.
B. Regulation of Bile Acid Synthesis
- Cholesterol 7α-hydroxylase (CYP7A1): This is the rate-limiting enzyme.
- Negative Feedback by Bile Acids: High levels of bile acids returning to the liver inhibit the transcription of the CYP7A1 gene.
- Positive Regulation by Cholesterol: Increased cholesterol induces CYP7A1 activity, ensuring excess cholesterol can be eliminated.
C. Regulation of Cholesterol Transport
LDL Receptor Regulation:
- The number of LDL receptors on the cell surface is the primary determinant of LDL clearance from the blood.
- High Cellular Cholesterol: Downregulates LDL receptor synthesis (via the SREBP-2 mechanism).
- Low Cellular Cholesterol: Upregulates LDL receptor synthesis.
- PCSK9: This enzyme promotes the degradation of the LDL receptor. Inhibitors of PCSK9 are a new class of drugs for lowering LDL.
Dietary and Hormonal Factors:
- Saturated and Trans Fats: Increase LDL cholesterol.
- Soluble Fiber: Lowers LDL cholesterol by interfering with bile acid reabsorption.
- Insulin: Promotes cholesterol synthesis.
- Estrogens: Tend to lower LDL and raise HDL.
D. Importance of Cholesterol Homeostasis
The tight regulation is vital because both insufficient (hypocholesterolemia) and excessive (hypercholesterolemia) cholesterol levels are detrimental. Excess cholesterol, particularly carried by LDL, can lead to its deposition in arterial walls, causing atherosclerosis.
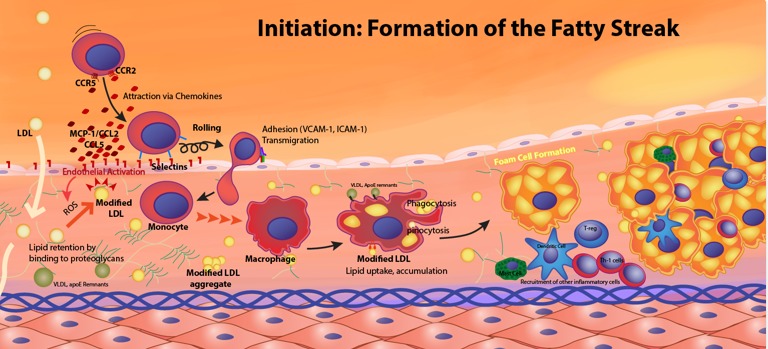
Clinical Significance of Cholesterol: Atherosclerosis
Atherosclerosis is a chronic inflammatory disease characterized by the buildup of fatty plaques within the arterial walls, leading to hardening and narrowing of the arteries.
A. Hypercholesterolemia and Dyslipidemia
- Hypercholesterolemia: Abnormally high levels of cholesterol in the blood.
- Dyslipidemia: A broader term for abnormal lipid levels, including high LDL ("bad cholesterol"), low HDL ("good cholesterol"), and high triglycerides.
B. The Role of Lipoproteins in Atherosclerosis
- Low-Density Lipoprotein (LDL) - The Primary Atherogenic Particle:
- High LDL levels lead to its infiltration into the arterial wall, where it becomes oxidized (oxLDL).
- Macrophages ingest oxLDL in an uncontrolled manner, transforming into foam cells.
- Accumulations of foam cells form fatty streaks, the earliest lesions of atherosclerosis.
- High-Density Lipoprotein (HDL) - The Anti-Atherogenic Particle:
- HDL is crucial for reverse cholesterol transport, removing excess cholesterol from arterial walls and transporting it to the liver.
- HDL also has antioxidant and anti-inflammatory properties. High HDL levels are associated with reduced CVD risk.
C. Pathogenesis of Atherosclerosis
The development of atherosclerotic plaques is a multi-stage process:
- Endothelial Dysfunction: Damage to the artery's inner lining.
- LDL Infiltration and Oxidation: LDL enters the arterial wall and becomes oxidized.
- Macrophage Recruitment and Foam Cell Formation: Immune cells are recruited and become lipid-laden foam cells.
- Smooth Muscle Cell Migration and Proliferation: These cells contribute to the bulk of the plaque.
- Fibrous Cap Formation: A cap of collagen and smooth muscle cells forms over the lipid core.
- Plaque Progression and Complications: Over time, plaques can grow, develop a necrotic core, and become unstable. Plaque rupture exposes the core to blood, leading to rapid thrombus (blood clot) formation, which can cause a heart attack or stroke.
D. Management of Dyslipidemia and CVD Risk
- Lifestyle Modifications: Diet, physical activity, weight management, and smoking cessation.
- Pharmacological Interventions:
- Statins (HMG-CoA Reductase Inhibitors): The most effective drugs for lowering LDL.
- Ezetimibe: Inhibits cholesterol absorption.
- PCSK9 Inhibitors: Prevent LDL receptor degradation.
- Bile Acid Sequestrants: Increase cholesterol excretion via bile acids.
Cholesterol Metabolism Pathway Read More »

Integrated Metabolism and Fuel Homeostasis
Integrated Metabolism and Fuel Homeostasis
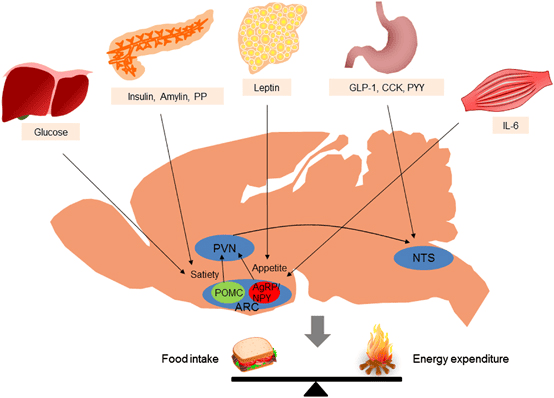
Fuel Homeostasis refers to the dynamic equilibrium and finely tuned regulation of energy substrates (glucose, fatty acids, ketone bodies, amino acids) in the body. Its primary goal is to ensure a continuous and adequate supply of fuel to all tissues, particularly the brain, under varying physiological conditions.
It is crucial for survival, allowing the body to adapt to fluctuations in nutrient availability and energy demand. Disruptions lead to metabolic diseases like diabetes, obesity, and metabolic syndrome.
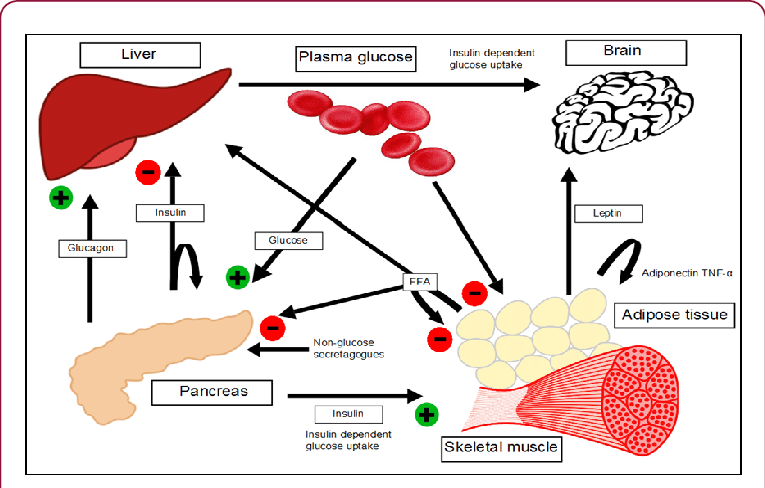
Key Metabolic Organs and Their Specialized Roles
The human body is a highly integrated system where different organs specialize in fuel storage, production, and utilization.
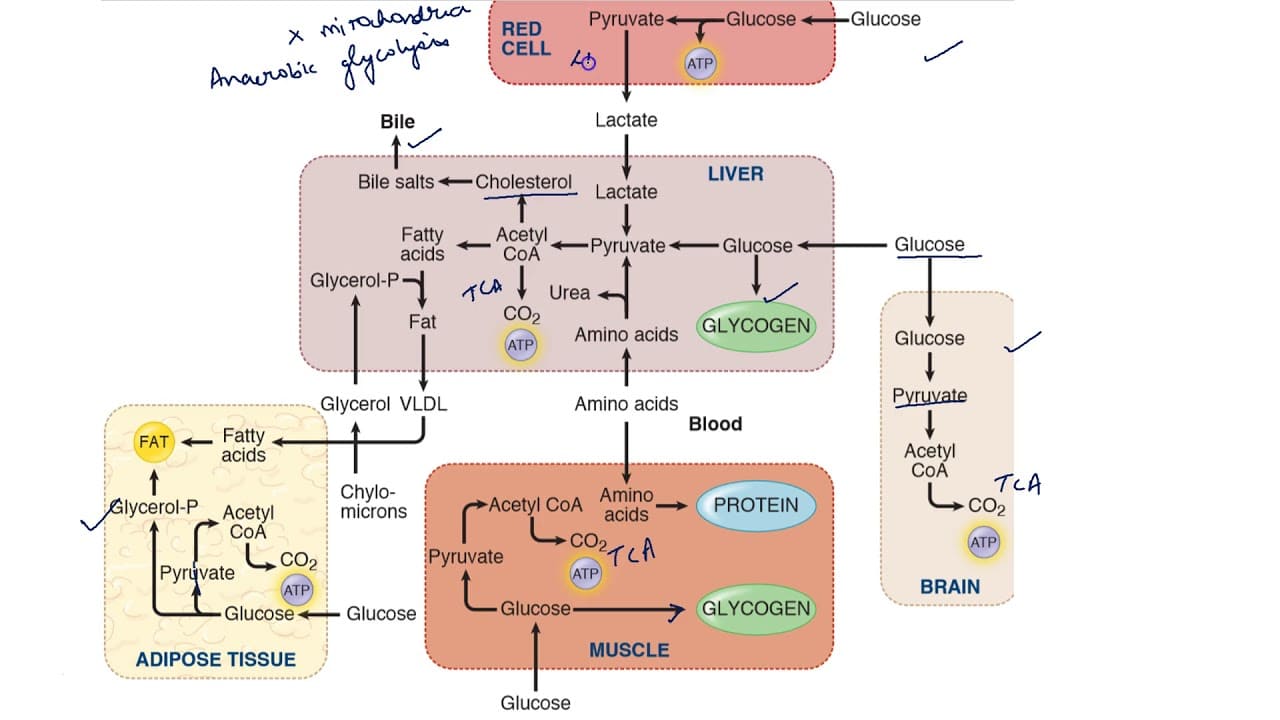
Liver (Hepatocytes): The Metabolic Hub
- Glucose Homeostasis: Central to maintaining blood glucose levels.
- Fed State: Takes up excess glucose, converting it to glycogen (glycogenesis) or fatty acids (lipogenesis).
- Fasting State: Releases glucose into the blood via glycogenolysis and gluconeogenesis.
- Lipid Metabolism: Site of de novo fatty acid synthesis, cholesterol synthesis, and VLDL assembly. It is also the primary site for ketogenesis during prolonged fasting.
- Amino Acid Metabolism: Site for amino acid uptake, protein synthesis, deamination, and the urea cycle.
- Lack of Ketone Body Utilization: Cannot use ketone bodies as fuel due to the absence of thiophorase.
Adipose Tissue (Adipocytes): The Energy Storehouse
- Storage: Primary site for the long-term storage of energy as triacylglycerols (TAGs).
- Mobilization: Releases free fatty acids and glycerol via lipolysis during fasting.
- Synthesis: Can synthesize TAGs from fatty acids and glycerol-3-phosphate.
- Endocrine Organ: Produces adipokines (e.g., leptin, adiponectin).
Skeletal Muscle (Myocytes): The Major Energy Consumer
- Fuel Utilization: Highly versatile; can use glucose, fatty acids, and ketone bodies.
- Glycogen Storage: Stores significant amounts of glycogen, but only for its own use (lacks glucose-6-phosphatase).
- Fatty Acid Oxidation: Major site for fatty acid oxidation, particularly during exercise and fasting.
- Protein Reservoir: A significant protein reserve that can be catabolized during prolonged fasting.
Brain (Neurons and Glial Cells): Obligate Glucose User, Adaptable in Fasting
- Primary Fuel: Under normal conditions, relies almost exclusively on glucose.
- Adaptation in Fasting: During prolonged fasting, the brain can adapt to utilize ketone bodies as a significant alternative fuel, sparing muscle protein.
- Cannot use Fatty Acids: Fatty acids cannot cross the blood-brain barrier.
Pancreas (Islets of Langerhans): The Endocrine Regulator
- Insulin (Beta Cells): Released in response to high blood glucose (fed state). Promotes fuel storage.
- Glucagon (Alpha Cells): Released in response to low blood glucose (fasting state). Promotes fuel mobilization.
- Somatostatin (Delta Cells): Inhibits secretion of both insulin and glucagon.
Major Hormones Orchestrating Fuel Homeostasis
These hormones act synergistically and antagonistically to maintain metabolic balance.
Insulin (Anabolic Hormone)
- Source: Pancreatic β-cells.
- Stimulus: High blood glucose, amino acids.
- Overall Effect: Promotes fuel storage; lowers blood glucose.
- Actions:
- Liver: Increases glycogenesis, lipogenesis; inhibits glycogenolysis, gluconeogenesis.
- Muscle: Increases glucose uptake (via GLUT4), glycogenesis, protein synthesis.
- Adipose: Increases glucose uptake (via GLUT4), TAG synthesis; inhibits lipolysis (inhibits HSL).
Glucagon (Catabolic Hormone)
- Source: Pancreatic α-cells.
- Stimulus: Low blood glucose.
- Overall Effect: Promotes fuel mobilization; raises blood glucose.
- Actions (primarily liver): Increases glycogenolysis, gluconeogenesis, ketogenesis; inhibits glycogenesis, lipogenesis.
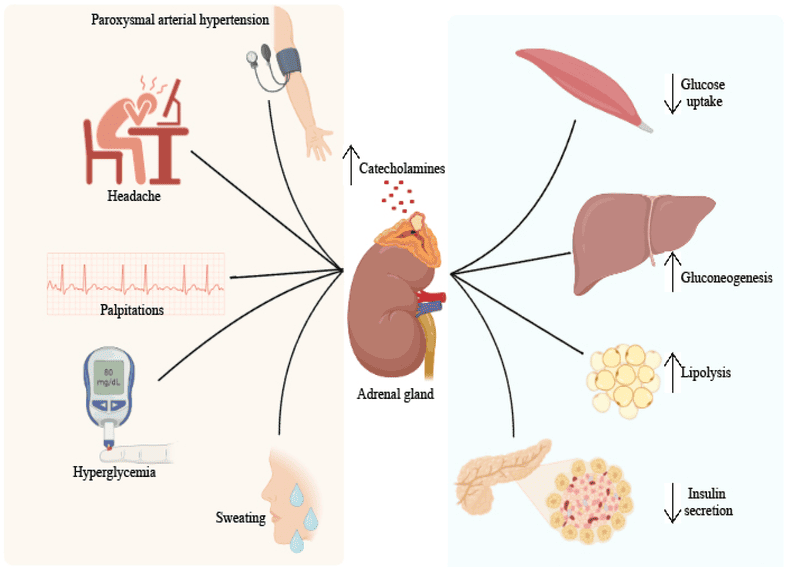
Catecholamines (Epinephrine, Norepinephrine - Stress Hormones)
- Source: Adrenal medulla, sympathetic nervous system.
- Stimulus: Stress, exercise, hypoglycemia.
- Overall Effect: "Fight or flight"; rapid mobilization of energy stores.
- Actions:
- Liver & Muscle: Increases glycogenolysis.
- Adipose: Potent activator of HSL, promoting lipolysis.
Cortisol (Glucocorticoid - Stress Hormone)
- Source: Adrenal cortex.
- Stimulus: Stress (chronic), low blood glucose.
- Overall Effect: Sustained glucose production; catabolic.
- Actions:
- Liver: Increases gluconeogenesis (by increasing enzyme synthesis).
- Muscle: Increases protein breakdown.
- Adipose: Increases lipolysis.
- Decreases peripheral glucose utilization.
The Fed State (Post-prandial Metabolism)
The fed state is characterized by nutrient absorption from the gastrointestinal tract, leading to elevated levels of glucose, amino acids, and triacylglycerols in the blood. The body's primary response is to store these excess nutrients and utilize glucose as the main fuel.
A. High Insulin:Glucagon Ratio:
- Following a meal, especially one rich in carbohydrates, blood glucose levels rise.
- This rise in glucose stimulates the pancreatic β-cells to release insulin.
- Simultaneously, high glucose inhibits the pancreatic α-cells, suppressing glucagon secretion.
- The resulting high insulin:glucagon ratio orchestrates the anabolic (storage) and glucose-utilizing responses.
B. Carbohydrate Metabolism: Glucose as the Primary Fuel and for Storage
Tissue-Specific Glucose Uptake and Utilization:
Liver:
- High Priority Uptake: Glucose enters hepatocytes via GLUT2 transporters.
- Phosphorylation: Glucokinase rapidly phosphorylates glucose to Glucose-6-Phosphate, trapping it inside.
- Glycogenesis (Glycogen Synthesis): G6P is directed towards glycogen synthesis. Insulin activates glycogen synthase.
- Glycolysis and Pyruvate Oxidation: Excess G6P enters glycolysis, and the resulting pyruvate is converted to Acetyl-CoA.
- Lipogenesis (Fatty Acid Synthesis): When energy and glycogen stores are full, Acetyl-CoA is channeled into de novo fatty acid synthesis. Insulin stimulates this process by activating Acetyl-CoA Carboxylase (ACC).
- VLDL Synthesis: Newly synthesized fatty acids are esterified to form TAGs, which are packaged into Very-Low-Density Lipoproteins (VLDL) and secreted into the bloodstream.
Adipose Tissue (Adipocytes):
- Insulin-Dependent Glucose Uptake: Insulin stimulates the translocation of GLUT4 transporters to the cell membrane.
- Glycerol-3-Phosphate Production: Glucose undergoes glycolysis to produce glycerol-3-phosphate, essential for esterifying fatty acids into TAGs.
- Fatty Acid Uptake: Adipose tissue takes up fatty acids from chylomicrons and VLDL via the action of Lipoprotein Lipase (LPL), which is activated by insulin.
Skeletal Muscle:
- Insulin-Dependent Glucose Uptake: Insulin stimulates GLUT4 translocation, increasing glucose uptake.
- Glycogenesis: Muscle cells synthesize glycogen for their own energy reserves.
- Glycolysis and Oxidation: Glucose is used as a primary fuel source for ATP production.
Brain:
- Insulin-Independent Glucose Uptake: Glucose uptake occurs via GLUT1 and GLUT3 transporters, ensuring a constant supply.
- High Glucose Utilization: The brain consumes a significant amount of glucose (about 120g/day).
C. Lipid Metabolism: Storage and Transport
- Dietary Fat Absorption and Chylomicron Formation: Dietary TAGs are hydrolyzed, absorbed, and then re-esterified within enterocytes. These TAGs are packaged into chylomicrons and released into the lymph and then the bloodstream.
- Chylomicron Metabolism: As chylomicrons circulate, their TAGs are hydrolyzed by Lipoprotein Lipase (LPL), an enzyme activated by insulin. This promotes the uptake of fatty acids into adipose tissue (for storage) and muscle (for use).
- Hepatic VLDL Production: As mentioned, the liver converts excess glucose into fatty acids, which are packaged as TAGs into VLDL particles and secreted. Like chylomicrons, VLDL TAGs are acted upon by LPL.
D. Amino Acid Metabolism: Protein Synthesis
- Amino Acid Absorption: Dietary proteins are digested into amino acids and transported to the liver via the portal circulation.
- Tissue-Specific Utilization:
- Liver: Uses amino acids for liver protein synthesis, synthesis of plasma proteins (e.g., albumin), and synthesis of non-protein nitrogenous compounds. Excess amino acids can be deaminated and their carbon skeletons used for energy or lipogenesis.
- Skeletal Muscle: Insulin promotes the uptake of amino acids. The primary fate is protein synthesis, to repair and build muscle mass.
- Other Tissues: Amino acids are taken up for the synthesis of new proteins and other molecules.
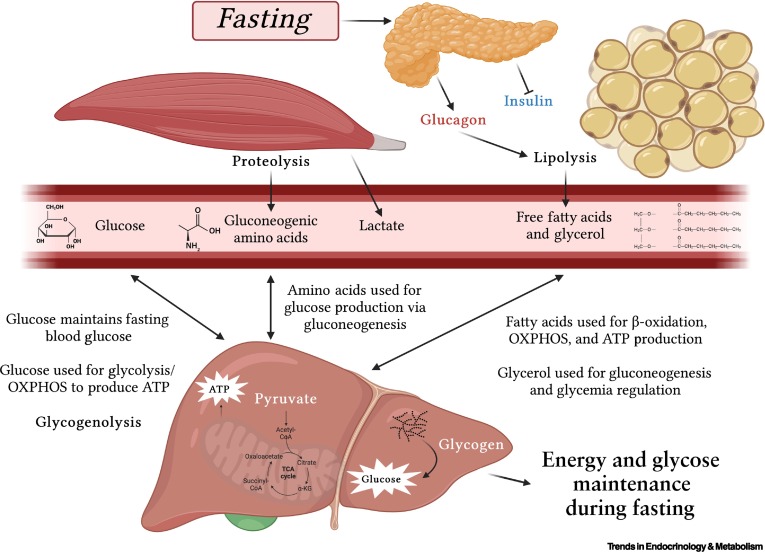
The Fasting State (Early Fasting, Overnight Fast)
The fasting state is characterized by the absence of nutrient intake. The body must now shift from storing fuels to mobilizing its endogenous reserves to maintain a steady supply of energy, especially for the brain. This transition is orchestrated by a low insulin:glucagon ratio.
A. Low Insulin:High Glucagon Ratio:
- As blood glucose levels fall, pancreatic β-cells reduce insulin secretion.
- Concurrently, falling glucose stimulates pancreatic α-cells to increase glucagon secretion.
- The resulting low insulin:high glucagon ratio is the primary signal that triggers the mobilization of stored fuels and the production of new glucose.
- Catecholamines (epinephrine, norepinephrine) and cortisol also play supportive roles.
B. Carbohydrate Metabolism: Glucose Production and Sparing
The primary goal is to maintain blood glucose levels for the brain and other glucose-dependent tissues.
Glycogenolysis (Glycogen Breakdown):
- Liver Glycogen: This is the first line of defense. Hepatic glycogen is rapidly mobilized, stimulated by glucagon and epinephrine. The resulting glucose-6-phosphate is dephosphorylated by glucose-6-phosphatase (present only in the liver) to release free glucose into the blood.
- Duration: Liver glycogen can maintain blood glucose for about 12-24 hours.
- Muscle Glycogen: Muscle glycogen is used only by the muscle itself for energy and cannot be released into the blood.
Gluconeogenesis (New Glucose Synthesis):
- As liver glycogen is depleted, gluconeogenesis becomes the primary mechanism for maintaining blood glucose. This is highly active in the liver.
- Substrates for Gluconeogenesis:
- Lactate: From anaerobic glycolysis in red blood cells.
- Glycerol: Released from the breakdown of TAGs in adipose tissue.
- Glucogenic Amino Acids: Derived from protein breakdown, primarily in skeletal muscle.
- Hormonal Regulation: Glucagon and cortisol are major stimulators.
Glucose Sparing:
To conserve glucose for the brain, other tissues switch their fuel preference to fatty acids and ketone bodies.
C. Lipid Metabolism: Mobilization of Stored Fat
Lipolysis in Adipose Tissue:
- Hormone-Sensitive Lipase (HSL): Glucagon and catecholamines activate HSL in adipocytes via a cAMP-dependent cascade.
- HSL hydrolyzes stored TAGs into free fatty acids (FFAs) and glycerol.
- FFAs: Released into the bloodstream, bind to albumin, and are transported to tissues for β-oxidation.
- Glycerol: Released into the bloodstream and travels to the liver to serve as a substrate for gluconeogenesis.
Fatty Acid Oxidation (β-Oxidation):
- Liver: Becomes a major site of fatty acid oxidation, providing ATP for gluconeogenesis. Excess Acetyl-CoA fuels ketogenesis.
- Skeletal Muscle, Heart, Kidneys: Utilize fatty acids as their primary fuel, thereby sparing glucose.
Ketogenesis (Ketone Body Formation):
- Location: Liver mitochondria.
- Stimulus: High rate of fatty acid oxidation in the liver produces large amounts of Acetyl-CoA. When the TCA cycle is saturated (due to OAA being diverted for gluconeogenesis), the excess Acetyl-CoA is diverted to ketone body synthesis.
- Products: Acetoacetate and β-hydroxybutyrate.
- Purpose: Ketone bodies are water-soluble fuels that can be transported to extrahepatic tissues, particularly the brain, muscle, and heart.
D. Amino Acid Metabolism: Protein Breakdown for Glucose Production
Protein Breakdown in Muscle:
- As fasting continues, skeletal muscle protein becomes a significant source of amino acids for gluconeogenesis. Cortisol promotes this breakdown.
- Glucogenic Amino Acids: Released into the bloodstream and transported to the liver (e.g., alanine, glutamine).
- Alanine Cycle (Cahill Cycle): Pyruvate in muscle is transaminated to alanine, which travels to the liver. In the liver, alanine is converted back to pyruvate for gluconeogenesis.
- Glutamine: Plays a major role in transporting amino groups from muscle to the liver and kidneys.
Urea Cycle:
The amino groups removed from amino acids are converted to ammonia, which is detoxified in the liver via the urea cycle, producing urea for excretion. The rate of the urea cycle increases during fasting.
In summary, the early fasting state is a period of catabolism driven by a low insulin:glucagon ratio. The body prioritizes maintaining blood glucose through glycogenolysis and gluconeogenesis, while other tissues shift to fatty acid oxidation. Ketone body production begins to ramp up, setting the stage for their increased utilization in prolonged starvation.
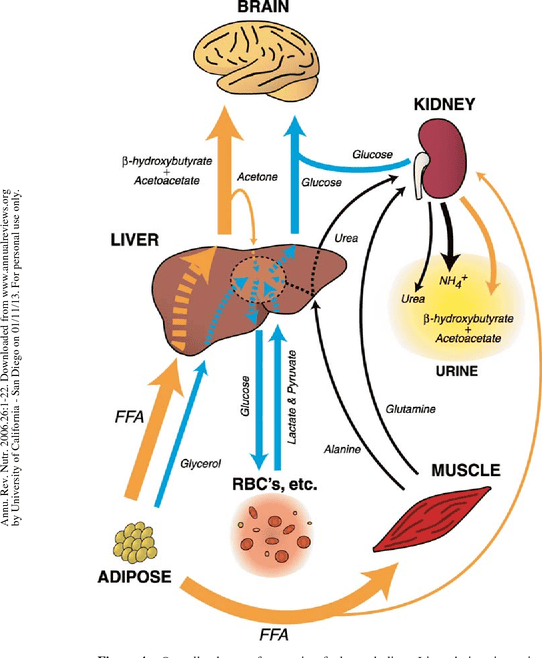
The Starved State (Prolonged Fasting/Starvation)
The starved state represents an extended period of nutrient deprivation, pushing the body's metabolic adaptations to their limits. The primary goals shift to:
- Glucose Sparing: Minimizing the use of glucose by peripheral tissues.
- Protein Sparing: Reducing the breakdown of essential muscle protein.
- Increased Reliance on Fat and Ketone Bodies: Maximizing energy production from abundant fat stores.
A. Continued Low Insulin:High Glucagon Ratio (and elevated stress hormones):
- The hormonal profile established in early fasting persists and may even intensify.
- Insulin levels remain very low, while glucagon, cortisol, and epinephrine remain elevated, reinforcing the catabolic drive.
B. Carbohydrate Metabolism: Extreme Glucose Sparing and Gluconeogenesis Adaptation
Liver Glycogen Depletion:
By the time the starved state is reached (typically after 24-48 hours), liver glycogen stores are almost completely depleted. The body can no longer rely on glycogenolysis.
Sustained Gluconeogenesis (but with changing substrates):
- Gluconeogenesis remains the sole source of new glucose, with kidney gluconeogenesis becoming increasingly significant (up to 40-50% of total production).
- Shift in Substrates:
- Glycerol: Becomes a relatively constant source due to ongoing lipolysis.
- Amino Acids: The rate of muscle protein breakdown decreases significantly after several days/weeks. This is a crucial adaptation to preserve essential lean body mass. The contribution of amino acids to gluconeogenesis gradually declines.
- Lactate: Continues to contribute to a minor extent.
Brain's Adaptation to Ketone Bodies (Glucose Sparing):
- This is the most critical adaptation in the starved state. The brain significantly increases its utilization of ketone bodies (β-hydroxybutyrate and acetoacetate) for energy.
- Mechanism: Ketone bodies cross the blood-brain barrier and are converted back to Acetyl-CoA for the TCA cycle.
- Impact: By shifting to ketone bodies, the brain dramatically reduces its demand for glucose (from ~120g/day to as low as 30-40g/day). This reduces the need for gluconeogenesis from amino acids, thereby sparing muscle protein.
C. Lipid Metabolism: Maximized Mobilization and Ketone Body Production
Maximized Lipolysis:
Lipolysis in adipose tissue continues at a very high rate, providing a continuous supply of fatty acids (for fuel) and glycerol (for gluconeogenesis). Fat stores are the largest energy reserve.
Massive Ketogenesis:
The liver's production of ketone bodies reaches its peak. The high influx of fatty acids, coupled with the low insulin state, promotes maximal β-oxidation and subsequent conversion of Acetyl-CoA into acetoacetate and β-hydroxybutyrate. Blood ketone body levels rise to very high concentrations, serving as the primary fuel for the brain, heart, and skeletal muscle.
D. Amino Acid Metabolism: Protein Sparing and Reduced Nitrogen Excretion
Reduced Muscle Protein Breakdown:
After an initial period of high protein catabolism, the body adapts to significantly reduce muscle protein breakdown. This is directly linked to the brain's increased use of ketone bodies, as less glucose needs to be synthesized from amino acids. This adaptation is critical for long-term survival.
Decreased Urea Production:
As amino acid catabolism decreases, the amount of nitrogen released also decreases. Consequently, the liver's production of urea via the urea cycle significantly declines. This is reflected in a reduced excretion of urea in the urine, signifying the shift to protein-sparing metabolism.
Summary of the Starved State: The starved state is characterized by extreme adaptations aimed at survival. The body shifts almost entirely to fat and ketone body metabolism to preserve its vital protein reserves. The brain becomes a major consumer of ketone bodies, dramatically reducing its glucose requirement and allowing for a significant reduction in the breakdown of muscle protein. This allows individuals to survive for extended periods without food.
Diabetes Mellitus as a Disorder of Fuel Homeostasis
Diabetes Mellitus (DM) is a group of metabolic diseases characterized by hyperglycemia (high blood glucose) resulting from defects in insulin secretion, insulin action, or both. This chronic hyperglycemia is associated with long-term damage and failure of various organs.
The core problem is a breakdown in the body's ability to regulate glucose, leading to a state that inappropriately resembles a constant "fasted" or even "starved" state in some tissues, despite abundant glucose in the blood.
A. Overview of Types of Diabetes:
Type 1 Diabetes Mellitus (T1DM): Absolute Insulin Deficiency
- Cause: Autoimmune destruction of the pancreatic β-cells, leading to an absolute deficiency of insulin production.
- Onset: Typically in childhood or adolescence.
- Metabolic State: Resembles a perpetual, severe starved state because glucose cannot enter insulin-dependent cells.
Type 2 Diabetes Mellitus (T2DM): Insulin Resistance with Relative Insulin Deficiency
- Cause: A combination of insulin resistance (target cells fail to respond to insulin) and progressive pancreatic β-cell dysfunction.
- Onset: Typically in adulthood, but increasingly seen in adolescents.
Gestational Diabetes Mellitus (GDM):
- Cause: Insulin resistance that develops during pregnancy, often resolving after childbirth but increasing future risk of T2DM.
B. Metabolic Consequences of Absolute Insulin Deficiency (Type 1 Diabetes)
This leads to a profound metabolic crisis, an exaggerated fasted state, if untreated.
Hyperglycemia (High Blood Glucose):
- Increased Hepatic Glucose Production: Unchecked glycogenolysis and gluconeogenesis due to unopposed glucagon.
- Decreased Glucose Utilization: Insulin-dependent tissues (muscle, adipose) cannot take up glucose due to the lack of GLUT4 translocation.
- Result: Blood glucose soars, leading to osmotic diuresis (excessive urination) and thirst (polydipsia).
Increased Lipolysis and Hypertriglyceridemia:
- Unchecked Lipolysis: The absence of insulin means Hormone-Sensitive Lipase (HSL) is constantly active, leading to massive breakdown of stored TAGs.
- Increased Fatty Acids & VLDL: High levels of free fatty acids are released, and the liver continuously synthesizes VLDL, leading to high blood triglycerides.
Exaggerated Ketogenesis and Diabetic Ketoacidosis (DKA):
- This is a life-threatening complication of uncontrolled T1DM.
- Mechanism: A high influx of fatty acids to the liver, coupled with their rapid β-oxidation, generates huge amounts of Acetyl-CoA. Uninhibited ketogenesis converts this Acetyl-CoA into ketone bodies.
- Metabolic Acidosis: The ketone bodies (acetoacetate and β-hydroxybutyrate) are strong acids. Their overproduction overwhelms the body's buffering capacity, causing blood pH to drop.
- Symptoms: Nausea, fruity breath (due to acetone), Kussmaul respiration (deep, labored breathing), confusion, and coma.
Protein Catabolism and Muscle Wasting:
The absence of insulin inhibits protein synthesis and promotes muscle protein breakdown. The released amino acids contribute to hepatic gluconeogenesis, exacerbating hyperglycemia and leading to significant weight loss.
C. Metabolic Consequences of Insulin Resistance (Type 2 Diabetes):
Hyperglycemia:
- Insulin Resistance in Muscle/Adipose: Reduced glucose uptake.
- Insulin Resistance in Liver: Fails to suppress hepatic glucose production.
- β-cell Dysfunction: Eventually, insulin secretion becomes inadequate to overcome resistance.
Dyslipidemia:
Insulin resistance leads to increased lipolysis, increased VLDL production, low HDL cholesterol, and the formation of small, dense LDL particles, increasing cardiovascular disease risk.
Less Prone to Ketoacidosis:
Patients with T2DM usually produce some insulin, which is often enough to suppress massive ketogenesis. A more common acute complication is Hyperosmolar Hyperglycemic State (HHS), characterized by extreme hyperglycemia and dehydration without significant ketoacidosis.
D. Key Principles of Treatment:
Type 1 Diabetes:
- Insulin Replacement: Essential for survival.
- Diet and Exercise: Crucial for managing blood glucose.
Type 2 Diabetes:
- Lifestyle Modifications: Diet and exercise are foundational.
- Oral Medications: Metformin (reduces hepatic glucose production), Sulfonylureas (stimulate insulin secretion), and others.
- Insulin Therapy: May be required as the disease progresses.
Integrated Metabolism and Fuel Homeostasis Read More »
Fatty Acid Metabolism
Fatty Acid Mobilization and Transport
When energy is needed, stored triacylglycerols (TAGs) in adipose tissue must be broken down, and the resulting fatty acids transported to other tissues for oxidation.
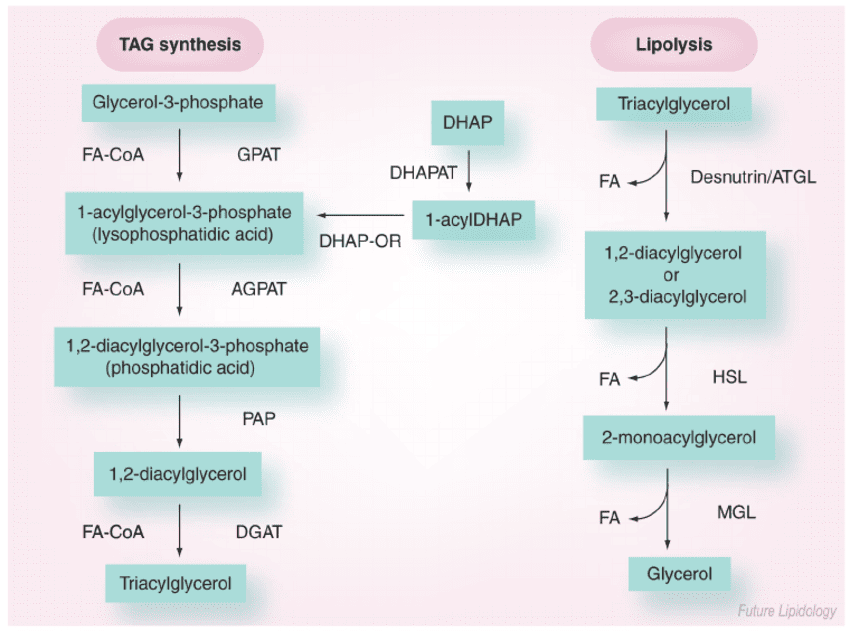
1. Triacylglycerol (TAG) Mobilization (Lipolysis)
Lipolysis is the process of breaking down stored TAGs into fatty acids and glycerol, occurring in adipocytes.
- Stimuli: Hormones like epinephrine, norepinephrine, and glucagon signal a low-energy state and activate lipolysis. Insulin inhibits it.
- Key Players (Lipases):
- Hormone-Sensitive Lipase (HSL): The rate-limiting enzyme, activated by phosphorylation via a PKA-dependent pathway.
- Adipose Triglyceride Lipase (ATGL): Initiates the first step, converting TAGs to DAGs.
- Monoacylglycerol Lipase (MAGL): Catalyzes the final step.
- Products of Lipolysis: Free Fatty Acids (FFAs) and Glycerol are released into the bloodstream.
- Fate of Glycerol: Travels to the liver, where it can enter glycolysis or gluconeogenesis. Adipocytes lack the enzyme (glycerol kinase) to re-utilize it.
2. Transport of Free Fatty Acids (FFAs) in Blood
Long-chain fatty acids are hydrophobic and require a carrier in the blood.
- Carrier Protein: Albumin, the most abundant plasma protein, serves as the primary carrier for FFAs.
- Mechanism: FFAs bind non-covalently to hydrophobic pockets on the albumin molecule.
- Delivery to Tissues: Fatty acid-albumin complexes deliver FFAs to tissues like muscle and heart, where they are taken up by specific fatty acid transporters.
3. Transport into Mitochondria (The Carnitine Shuttle)
Long-chain fatty acids (LCFAs) cannot directly cross the inner mitochondrial membrane. They require the Carnitine Shuttle to enter the mitochondrial matrix for beta-oxidation.
Steps of the Shuttle:
- Activation (Cytosol): The FFA is first activated to a fatty acyl-CoA by Fatty Acyl-CoA Synthetase, consuming 2 ATP equivalents.
- Transfer to Carnitine (Outer Membrane): The fatty acyl group is transferred from CoA to carnitine by Carnitine Palmitoyltransferase I (CPT-I), forming fatty acylcarnitine. CPT-I is the rate-limiting step and is inhibited by malonyl-CoA.
- Translocation (Inner Membrane): Carnitine-Acylcarnitine Translocase (CACT) transports fatty acylcarnitine into the matrix while simultaneously transporting a free carnitine out.
- Transfer Back to CoA (Matrix): Inside the matrix, Carnitine Palmitoyltransferase II (CPT-II) transfers the fatty acyl group back to a mitochondrial CoA, regenerating fatty acyl-CoA (now ready for beta-oxidation) and freeing carnitine for reuse.
Now, with the fatty acyl-CoA ready in the mitochondrial matrix, we can move on to the actual breakdown process: Fatty Acid Oxidation (Beta-Oxidation).
Fatty Acid Oxidation (Beta-Oxidation)
Once long-chain fatty acids (as fatty acyl-CoA) have successfully entered the mitochondrial matrix via the carnitine shuttle, they are ready for a cyclic process called β-oxidation. This pathway systematically cleaves two-carbon units from the carboxyl end of the fatty acyl-CoA, generating acetyl-CoA, NADH, and FADH₂, which then feed into the citric acid cycle and oxidative phosphorylation for ATP production.
- Primary Location: Mitochondrial matrix.
- Purpose: To generate energy (ATP) from stored fatty acids.
The Sequential Steps of β-Oxidation for Saturated Fatty Acyl-CoAs
Beta-oxidation is a four-step cyclic process. Each cycle shortens the fatty acyl-CoA by two carbons and produces one molecule of Acetyl-CoA, one NADH, and one FADH₂.
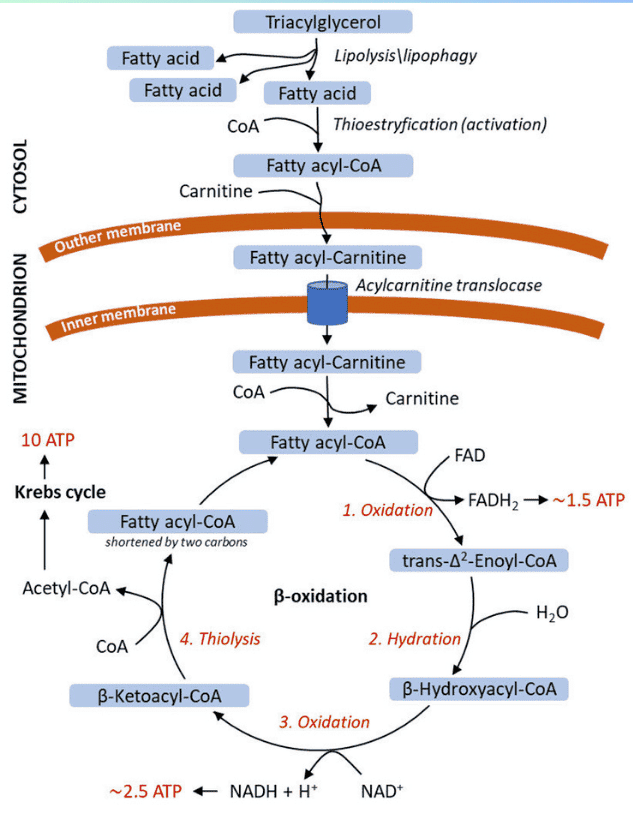
The Four Steps of One Cycle:
-
Oxidation (by FAD):
- Enzyme: Acyl-CoA Dehydrogenase (specific for chain length, e.g., VLCAD, LCAD, MCAD, SCAD).
- Reaction: Introduces a trans double bond between the α (C-2) and β (C-3) carbons of the fatty acyl-CoA, producing a trans-Δ²-enoyl-CoA.
- Product: FADH₂ (reduced flavin adenine dinucleotide). This FADH₂ then donates its electrons to Coenzyme Q in the electron transport chain, yielding ~1.5 ATP.
-
Hydration:
- Enzyme: Enoyl-CoA Hydratase (also known as Crotonase).
- Reaction: Adds water across the double bond of the trans-Δ²-enoyl-CoA, forming a hydroxyl group on the β-carbon. This produces L-β-hydroxyacyl-CoA.
-
Oxidation (by NAD⁺):
- Enzyme: β-hydroxyacyl-CoA Dehydrogenase.
- Reaction: Oxidizes the hydroxyl group on the β-carbon to a ketone group, producing β-ketoacyl-CoA.
- Product: NADH (reduced nicotinamide adenine dinucleotide). This NADH then donates its electrons to Complex I of the electron transport chain, yielding ~2.5 ATP.
-
Thiolytic Cleavage (Thiolysis):
- Enzyme: β-ketoacyl-CoA Thiolase (also known as Acyl-CoA Acetyltransferase).
- Reaction: Cleaves the bond between the α and β carbons. A molecule of Coenzyme A (CoA-SH) attacks the β-keto carbon, releasing one molecule of Acetyl-CoA and a new fatty acyl-CoA that is two carbons shorter than the original.
- Products: Acetyl-CoA (enters the Citric Acid Cycle) and a shortened fatty acyl-CoA (which re-enters the β-oxidation cycle).
Summary of One Cycle of β-Oxidation:
Input: Fatty Acyl-CoA (n carbons) → Output: 1 Acetyl-CoA + 1 FADH₂ + 1 NADH + Fatty Acyl-CoA (n-2 carbons)
Calculating the Net ATP Yield from Palmitate (16:0)
- Number of carbons: 16
- Number of Acetyl-CoA units produced: 16 / 2 = 8 Acetyl-CoA.
- Number of β-oxidation cycles needed: 8 - 1 = 7 cycles.
- ATP Yield Calculation:
- From β-oxidation cycles:
- 7 cycles × 1 FADH₂/cycle = 7 FADH₂
- 7 FADH₂ × 1.5 ATP/FADH₂ = 10.5 ATP
- 7 cycles × 1 NADH/cycle = 7 NADH
- 7 NADH × 2.5 ATP/NADH = 17.5 ATP
- Total from cycles = 10.5 + 17.5 = 28 ATP
- From Acetyl-CoA entering the Citric Acid Cycle (TCA Cycle):
- 8 Acetyl-CoA × (1 FADH₂ + 3 NADH + 1 GTP)/Acetyl-CoA
- 8 FADH₂ × 1.5 ATP/FADH₂ = 12 ATP
- 8 NADH × 2.5 ATP/NADH = 20 ATP
- 8 GTP × 1 ATP/GTP = 8 ATP
- Total from Acetyl-CoA = 12 + 20 + 8 = 40 ATP
- Initial Activation Cost:
- Activating the fatty acid consumes 2 ATP equivalents.
- Cost = -2 ATP
- From β-oxidation cycles:
- Net ATP Yield: (28 from cycles) + (40 from Acetyl-CoA) - 2 (activation) = 106 ATP.
Modifications for Unsaturated and Odd-Chain Fatty Acids
A. Unsaturated Fatty Acids:
- Problem: The presence of double bonds interferes with the standard pathway.
- Solutions:
- Enoyl-CoA Isomerase: For cis double bonds, this enzyme converts them to the trans form, bypassing the FADH₂-producing step in that cycle.
- 2,4-Dienoyl-CoA Reductase: For polyunsaturated fatty acids, this reductase (requiring NADPH) helps handle conjugated double bonds.
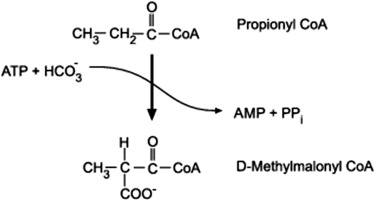
B. Odd-Chain Fatty Acids:
- Problem: The final cycle yields one Propionyl-CoA (3 carbons), which cannot enter the TCA cycle directly.
- Solution (Propionyl-CoA Pathway): Propionyl-CoA is converted to Succinyl-CoA (a TCA cycle intermediate) in a multi-step process requiring Biotin and Vitamin B12.
- Significance: This makes odd-chain fatty acids the only fatty acids that can yield a net glucose precursor.
Other Forms of Fatty Acid Oxidation
A. α-Oxidation:
- Location: Peroxisomes and Endoplasmic Reticulum.
- Purpose: Degrades fatty acids with a methyl group on the β-carbon (e.g., phytanic acid).
- Process: Removes one carbon at a time from the carboxyl end.
- Clinical Significance: A defect causes Refsum disease, leading to neurological damage.
B. ω-Oxidation:
- Location: Endoplasmic Reticulum of the liver and kidneys.
- Purpose: A minor pathway that becomes more important when β-oxidation is defective.
- Process: Oxidizes the methyl (ω) carbon at the opposite end of the chain, creating a dicarboxylic acid that can then undergo β-oxidation from both ends.
- Products: Succinate (4 carbons) and Adipate (6 carbons).
Ketone Body Metabolism (Ketogenesis and Ketolysis)
Under certain physiological conditions, particularly prolonged fasting, starvation, or uncontrolled diabetes, the liver produces significant amounts of ketone bodies from Acetyl-CoA. These ketone bodies serve as an alternative fuel source for extrahepatic (outside the liver) tissues, especially the brain, which cannot directly use fatty acids for energy.
Conditions That Lead to Ketogenesis
Ketogenesis is stimulated when:
- Low Glucose Availability: This is the primary driver. When glucose is scarce, the body turns to fat as its main energy source.
- High Rate of Fatty Acid Oxidation: Increased breakdown of fatty acids in the liver leads to an abundance of Acetyl-CoA.
- Low Oxaloacetate (OAA) Levels in the Liver: OAA is a crucial intermediate in the Citric Acid Cycle (TCA cycle) that combines with Acetyl-CoA to form citrate.
- During fasting, OAA is diverted to gluconeogenesis (glucose synthesis) in the liver to maintain blood glucose levels.
- This depletion of OAA means that Acetyl-CoA cannot efficiently enter the TCA cycle.
- High Glucagon/Insulin Ratio: Glucagon promotes fatty acid mobilization and gluconeogenesis, further contributing to the conditions favoring ketogenesis.
- Clinical States: Starvation/Fasting, Uncontrolled Diabetes Mellitus (Type 1), Low Carbohydrate, High-Fat Diets (Ketogenic Diets).
In essence, ketogenesis is a response to an oversupply of Acetyl-CoA (from fat breakdown) and an undersupply of OAA (due to gluconeogenesis) in the liver.
Synthesis of Ketone Bodies (Ketogenesis) in the Liver
Ketogenesis occurs exclusively in the mitochondrial matrix of liver cells.
The Three Ketone Bodies:
- Acetoacetate: The primary ketone body produced.
- β-Hydroxybutyrate: Formed by the reduction of acetoacetate.
- Acetone: A volatile byproduct of acetoacetate breakdown, produced in smaller quantities and excreted via breath.
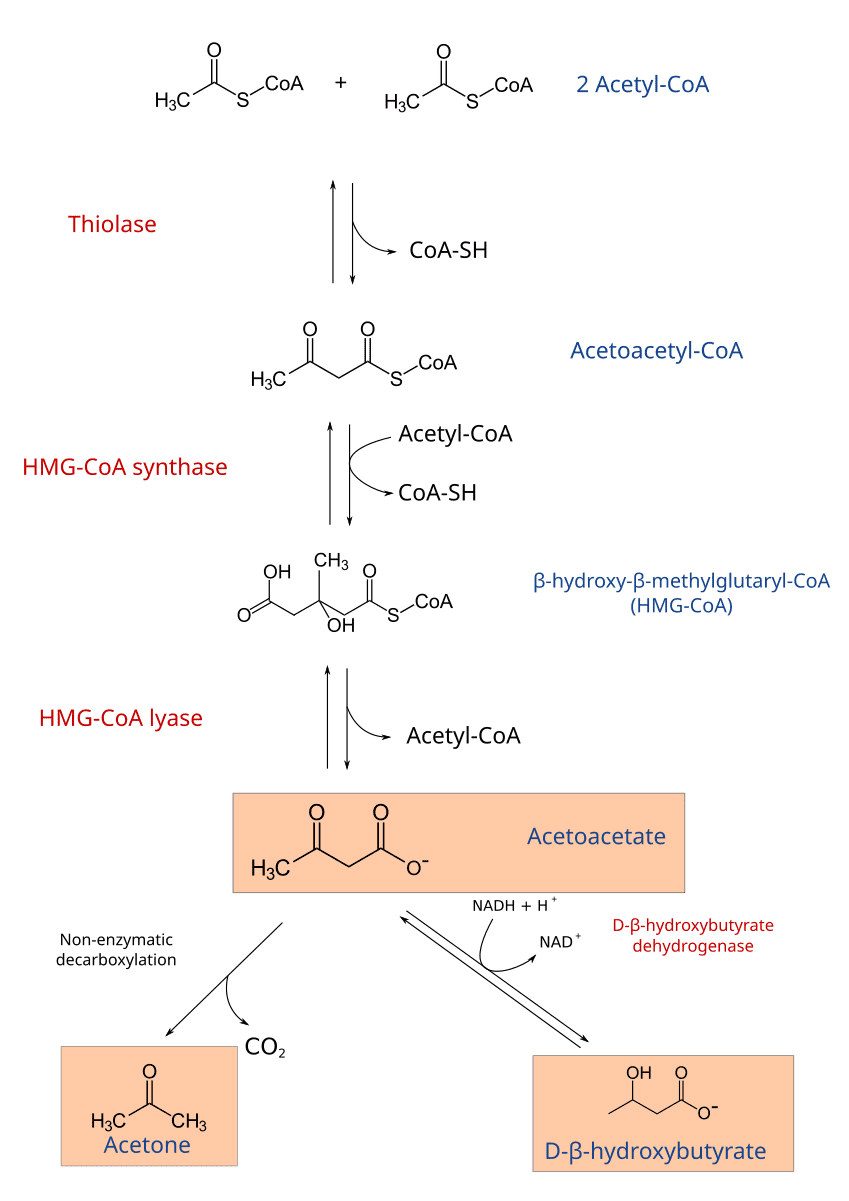
Steps of Ketogenesis:
-
1. Condensation of Two Acetyl-CoA Molecules:
- Enzyme: Thiolase (the reverse reaction of the last step of β-oxidation).
- Reaction:
2 Acetyl-CoA → Acetoacetyl-CoA + CoA-SH
-
2. Condensation with a Third Acetyl-CoA:
- Enzyme: HMG-CoA Synthase (Hydroxymethylglutaryl-CoA Synthase).
- Reaction:
Acetoacetyl-CoA + Acetyl-CoA + H₂O → β-hydroxy-β-methylglutaryl-CoA (HMG-CoA) + CoA-SH - Note: This is the rate-limiting step of ketogenesis.
-
3. Cleavage of HMG-CoA:
- Enzyme: HMG-CoA Lyase.
- Reaction:
HMG-CoA → Acetoacetate + Acetyl-CoA - This reaction produces the first ketone body, acetoacetate.
-
4. Interconversion and Breakdown of Acetoacetate:
- Acetoacetate can be reduced to β-hydroxybutyrate.
- Enzyme: β-hydroxybutyrate Dehydrogenase.
- Reaction:
Acetoacetate + NADH + H⁺ ⇌ β-Hydroxybutyrate + NAD⁺
- Acetoacetate can also spontaneously decarboxylate to Acetone (
Acetoacetate → Acetone + CO₂).
- Acetoacetate can be reduced to β-hydroxybutyrate.
Utilization (Ketolysis) of Ketone Bodies by Extrahepatic Tissues
Ketone bodies are water-soluble and can be transported via the bloodstream to peripheral tissues, which then convert them back into Acetyl-CoA for energy. The liver cannot utilize ketone bodies because it lacks a key enzyme for ketolysis.
Tissues that use Ketone Bodies: Brain, heart, skeletal muscle, renal cortex.
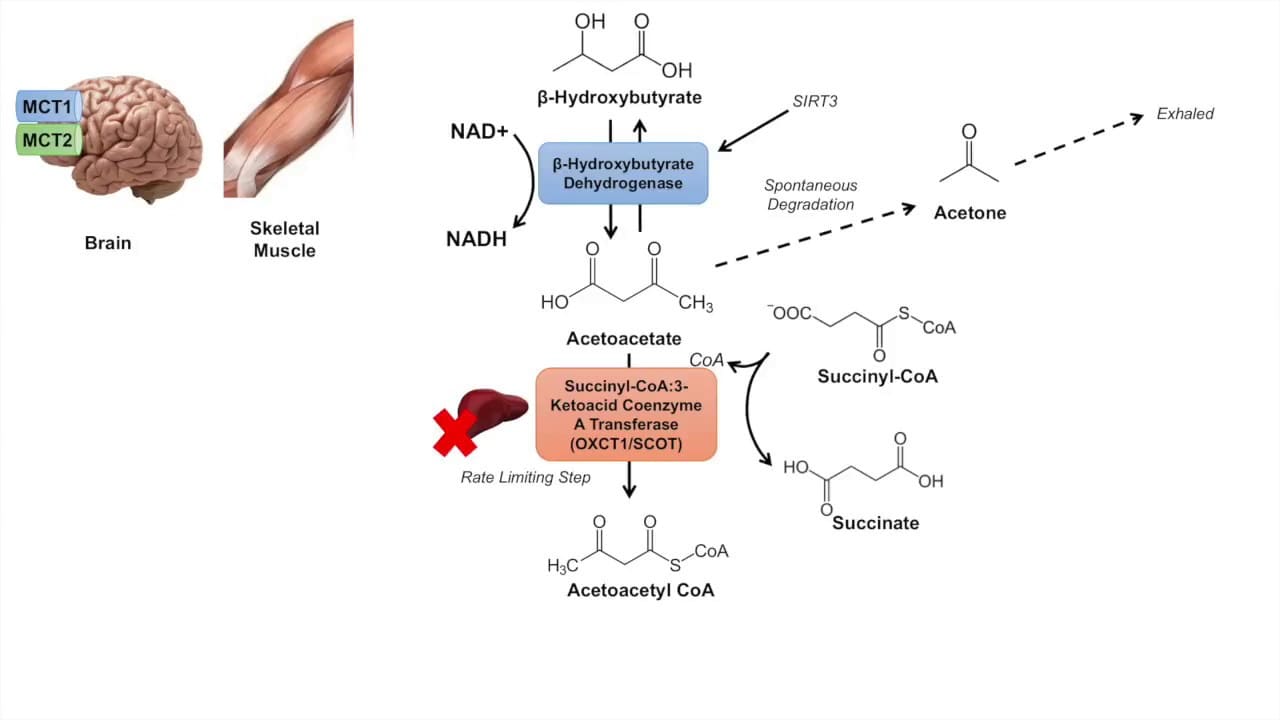
Steps of Ketolysis (Example: in the Brain/Muscle):
-
1. Conversion of β-Hydroxybutyrate to Acetoacetate:
- Enzyme: β-hydroxybutyrate Dehydrogenase.
- Reaction:
β-Hydroxybutyrate + NAD⁺ → Acetoacetate + NADH + H⁺
-
2. Activation of Acetoacetate:
- Enzyme: β-ketoacyl-CoA Transferase (also called Thiophorase).
- Reaction:
Acetoacetate + Succinyl-CoA → Acetoacetyl-CoA + Succinate - Crucial: This enzyme is absent in the liver, which is why the liver produces but cannot utilize ketone bodies.
-
3. Cleavage of Acetoacetyl-CoA:
- Enzyme: Thiolase.
- Reaction:
Acetoacetyl-CoA + CoA-SH → 2 Acetyl-CoA
The 2 molecules of Acetyl-CoA produced can then enter the Citric Acid Cycle to generate ATP.
Clinical Significance of Ketogenesis
The production and utilization of ketone bodies are normally well-regulated. However, imbalances can lead to serious clinical conditions.
- Physiological Ketosis: A normal and beneficial state that occurs during prolonged fasting, starvation, or a strict ketogenic diet. Ketone bodies provide a crucial fuel source, especially for the brain, preserving muscle protein.
- Pathological Ketosis (Ketoacidosis):
- Diabetic Ketoacidosis (DKA): This is a life-threatening complication of Type 1 Diabetes Mellitus.
- Cause: Absolute or severe relative insulin deficiency combined with elevated glucagon levels.
- Mechanism: Lack of insulin means cells cannot take up glucose, leading to severe hyperglycemia. Simultaneously, high glucagon promotes massive lipolysis and unchecked ketogenesis in the liver.
- Consequences: The rapid and excessive production of acidic ketone bodies overwhelms the body's buffering capacity, leading to a significant drop in blood pH (acidosis), dehydration, electrolyte imbalances, and potentially coma and death if untreated.
- Acetone: The increased production of acetoacetate leads to increased spontaneous decarboxylation to acetone, giving the breath of DKA patients a characteristic "fruity" odor.
- Alcoholic Ketoacidosis: Can occur in chronic alcoholics, often exacerbated by poor nutrition. Alcohol metabolism produces excess NADH, which shifts OAA to malate and inhibits gluconeogenesis, leading to a similar state of excessive ketogenesis and acidosis.
- Diabetic Ketoacidosis (DKA): This is a life-threatening complication of Type 1 Diabetes Mellitus.
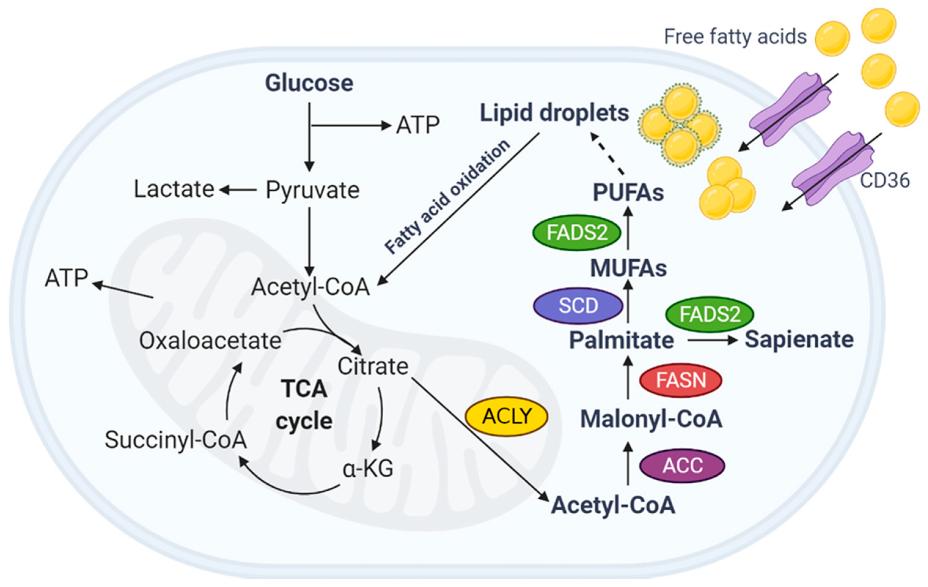
Fatty Acid Synthesis (Lipogenesis)
When the body has an abundance of energy, especially from a diet rich in carbohydrates, it converts excess glucose into fatty acids for long-term storage as triacylglycerols. This process is called lipogenesis.
Overview and Key Tissues
- Definition: The metabolic pathway that synthesizes fatty acids from acetyl-CoA.
- Primary Precursor: Acetyl-CoA, which is largely derived from carbohydrate metabolism (pyruvate oxidation).
- Location: Primarily in the cytosol of cells.
- Major Sites:
Liver: The most active site of fatty acid synthesis.Adipose Tissue: Also synthesizes fatty acids.Lactating Mammary Glands: Synthesize fatty acids for milk production.
- Main Product: Palmitate (16:0), a saturated 16-carbon fatty acid.
Key Steps and Enzymes in Fatty Acid Synthesis
Fatty acid synthesis is essentially a reversal of β-oxidation, but it uses different enzymes, occurs in a different cellular compartment, and employs a different electron donor.
A. Transport of Acetyl-CoA from Mitochondria to Cytosol:
- Problem: Acetyl-CoA is produced in the mitochondrial matrix, but synthesis occurs in the cytosol. The inner mitochondrial membrane is impermeable to Acetyl-CoA.
- Solution: The Citrate Shuttle
- Condensation: Acetyl-CoA combines with oxaloacetate (OAA) in the mitochondrial matrix to form citrate (catalyzed by Citrate Synthase).
- Transport: Citrate is transported across the inner mitochondrial membrane into the cytosol.
- Cleavage: In the cytosol, citrate is cleaved back into Acetyl-CoA and OAA by ATP Citrate Lyase. This step requires ATP.
Citrate + ATP + CoA-SH → Acetyl-CoA + OAA + ADP + Pi - Recycling OAA: The cytosolic OAA is converted to malate and then pyruvate (producing NADPH in the process via malic enzyme) before returning to the mitochondria.
B. Carboxylation of Acetyl-CoA to Malonyl-CoA:
- Enzyme: Acetyl-CoA Carboxylase (ACC).
- Reaction:
Acetyl-CoA + HCO₃⁻ + ATP → Malonyl-CoA + ADP + Pi - Significance: This is the rate-limiting and committed step of fatty acid synthesis.
- Requirements: Biotin and ATP.
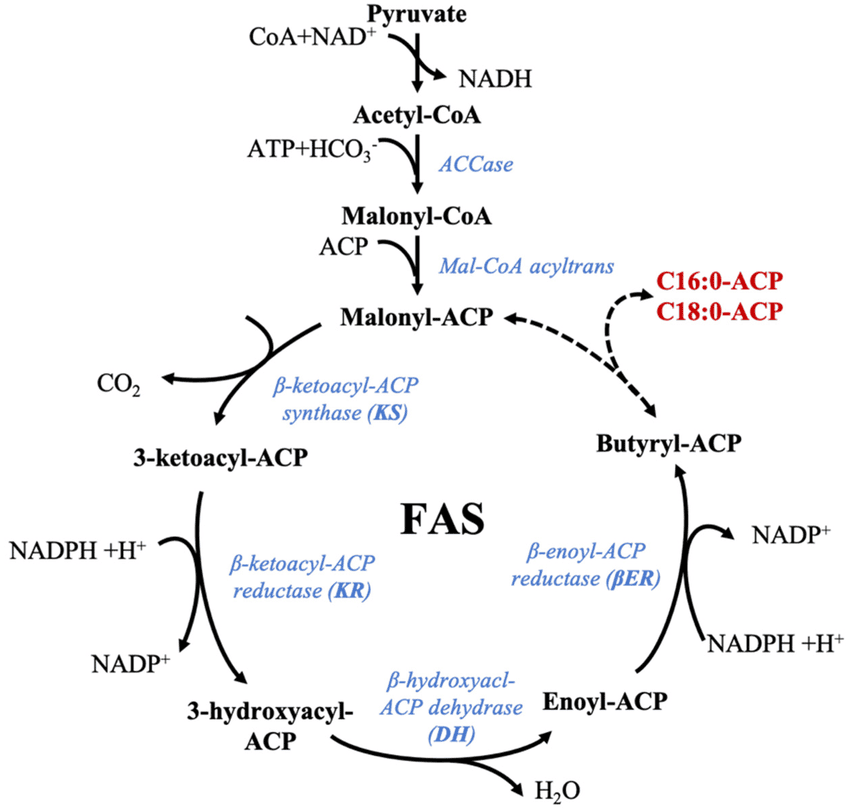
C. The Fatty Acid Synthase Complex:
Synthesis is carried out by a multi-enzyme complex called Fatty Acid Synthase (FAS). It contains seven different enzymatic activities and an acyl carrier protein (ACP).
- Electron Donor: NADPH (not NADH or FADH₂).
Steps of the FAS Cycle (Repeated 7 Times):
Each cycle adds a two-carbon unit from Malonyl-CoA and involves four steps:
- Condensation: The growing fatty acyl chain condenses with malonyl-ACP, releasing CO₂. (Enzyme: β-ketoacyl-ACP Synthase).
- Reduction (by NADPH): The β-keto group is reduced to a β-hydroxy group. (Enzyme: β-ketoacyl-ACP Reductase).
- Dehydration: Water is removed, creating a double bond. (Enzyme: β-hydroxyacyl-ACP Dehydratase).
- Reduction (by NADPH): The double bond is reduced, resulting in a saturated acyl-ACP chain that is two carbons longer. (Enzyme: Enoyl-ACP Reductase).
After 7 cycles, the 16-carbon palmitoyl-ACP is formed and then released as free palmitate by a Thioesterase.
Summary of Palmitate Synthesis:
Overall Reaction: 8 Acetyl-CoA + 7 ATP + 14 NADPH → Palmitate + 8 CoA + 7 ADP + 7 Pi + 14 NADP⁺ + 6 H₂O
Regulation of Fatty Acid Synthesis
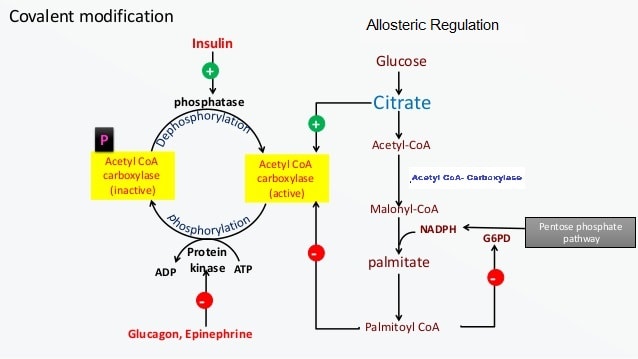
A. Short-Term Regulation (of ACC):
- Allosteric Activators: Citrate. High levels of citrate indicate excess energy and activate ACC.
- Allosteric Inhibitors: Long-Chain Fatty Acyl-CoAs. High levels of the end-product inhibit ACC.
- Covalent Modification:
- Dephosphorylation (Activation): Insulin activates a phosphatase that dephosphorylates and activates ACC.
- Phosphorylation (Inhibition): Glucagon and Epinephrine activate PKA, which phosphorylates and inactivates ACC. AMP-activated protein kinase (AMPK) also inactivates ACC when cellular energy is low.
B. Long-Term Regulation (Gene Expression):
- Dietary Factors: High-carbohydrate, low-fat diets increase the synthesis of ACC and FAS enzymes. Fasting or high-fat diets decrease their synthesis.
- Hormonal Factors: Insulin increases the synthesis of enzymes for fatty acid synthesis.
Elongation and Desaturation of Fatty Acids
Once palmitate (16:0) is synthesized, it can be further modified:
- Elongation: Occurs primarily in the endoplasmic reticulum (ER). Adds two carbons at a time, using Malonyl-CoA and NADPH, to produce stearate (18:0) and other longer fatty acids.
- Desaturation: Occurs in the ER. Introduces double bonds into saturated fatty acids.
- Enzymes: Fatty Acyl-CoA Desaturases, which require O₂, NADH (or NADPH), and cytochrome b5.
- Limitations: Mammals can introduce double bonds at Δ9, Δ6, and Δ5 positions but cannot introduce double bonds beyond Δ9. This is why linoleic acid (Δ9,12) and α-linolenic acid (Δ9,12,15) are essential fatty acids.
Fatty Acid Metabolism Read More »
Pentose Phosphate Pathway
Pentose Phosphate Pathway (PPP)
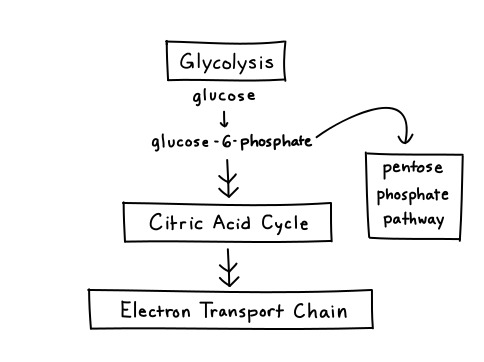
The Pentose Phosphate Pathway (PPP), also known as the Hexose Monophosphate Shunt (HMP Shunt), is an alternative metabolic route for glucose metabolism that runs parallel to glycolysis. The HMP pathway is also known as the Warburg-Dickens pathway. About 10% of glucose entering this pathway per day. The liver & RBCs metabolise about 30% of glucose by this pathway.
Unlike glycolysis, its primary purpose is not to generate ATP. Instead, its main functions are:
- Production of NADPH: Essential for reductive biosynthetic reactions and for protecting cells from oxidative stress.
- Production of Ribose-5-Phosphate: A vital precursor for the synthesis of nucleotides (DNA, RNA) and coenzymes.
Think of the PPP as a "shunt" because it diverts glucose-6-phosphate away from glycolysis to serve these distinct purposes, and can then feed intermediates back into glycolysis. It primarily occurs in the cytosol of cells.
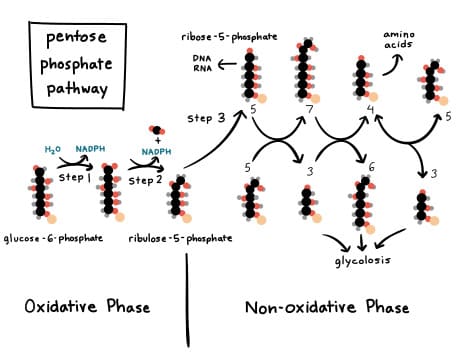
Two Major Phases of the PPP
The Pentose Phosphate Pathway is divided into two distinct phases:
a) The Oxidative (Irreversible) Phase:
- Function: This phase is responsible for the generation of NADPH and the production of ribulose-5-phosphate (which is then converted to ribose-5-phosphate).
- Nature: It is largely irreversible.
- Key Reactions: Involves oxidative decarboxylation reactions where glucose-6-phosphate is oxidized, releasing CO₂, and reducing NADP⁺ to NADPH.
b) The Non-Oxidative (Reversible) Phase:
- Function: This phase interconverts various sugar phosphates, primarily transforming pentose phosphates into glycolytic intermediates (fructose-6-phosphate and glyceraldehyde-3-phosphate). This allows carbon skeletons to be recycled back into glycolysis or used for gluconeogenesis.
- Nature: This phase is entirely reversible.
- Key Enzymes: Involves transketolase and transaldolase enzymes, which facilitate the transfer of two-carbon and three-carbon units, respectively.
Products of the PPP
The PPP is critically important because it provides two essential molecules:
a) NADPH (Nicotinamide Adenine Dinucleotide Phosphate, reduced form)
- Structure: Similar to NADH, but with an additional phosphate group.
- Function: Unlike NADH (used in catabolism for ATP), NADPH is predominantly used in anabolic (biosynthetic) processes and as a reductant in antioxidant defense.
- Reductive Biosynthesis: Providing reducing power for the synthesis of fatty acids, cholesterol, and steroid hormones. Tissues actively involved in these syntheses (e.g., liver, adipose tissue, adrenal cortex) have a highly active PPP.
- Antioxidant Defense: Protecting cells from damage by reactive oxygen species (ROS) by maintaining the reduced state of glutathione.
b) Ribose-5-Phosphate
- Structure: A five-carbon sugar phosphate.
- Function: This molecule is the direct precursor for the synthesis of:
- Nucleotides: The building blocks of DNA and RNA.
- Coenzymes: Such as ATP, NADH, FADH₂, and Coenzyme A.
- Demand: Cells that are rapidly dividing (e.g., bone marrow, skin, cancer cells) will have a high demand for ribose-5-phosphate.
Location of the pathway
- The enzymes are located in the cytosol.
- The tissues such as liver, adipose tissue, adrenal gland, erythrocytes, testes & lactating mammary gland, are highly active in the HMP shunt.
- Most of these tissues are involved in the biosynthesis of fatty acids and steroids, which are dependent on the supply of NADPH.
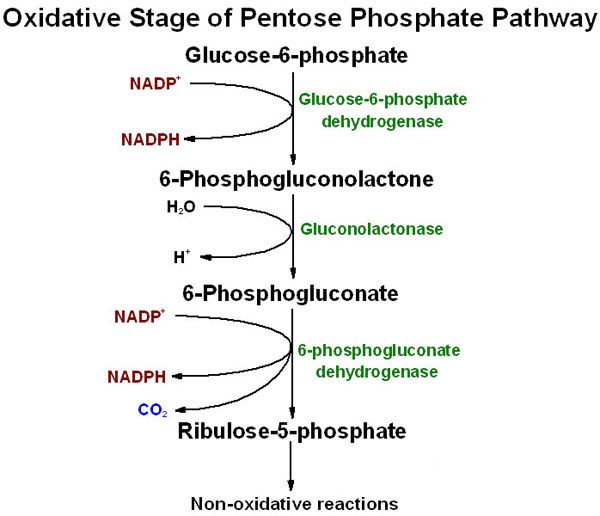
The Oxidative (Irreversible) Phase
This phase consists of three main reactions, starting with glucose-6-phosphate and culminating in the production of NADPH and ribulose-5-phosphate.
Key Concepts of the Oxidative Phase:
- Irreversible: The reactions in this phase are essentially unidirectional under physiological conditions.
- NADPH Production: This is the primary site of NADPH generation. Each molecule of glucose-6-phosphate entering this phase yields two molecules of NADPH.
- Substrate: Glucose-6-phosphate, which is also an intermediate in glycolysis.
- Location: Occurs in the cytosol.
The Three Reactions of the Oxidative Phase:
The oxidative phase involves the following sequential reactions:
1. Glucose-6-Phosphate Dehydrogenation (The Rate-Limiting Step)
- Enzyme: Glucose-6-Phosphate Dehydrogenase (G6PD)
- Reaction: Glucose-6-phosphate is oxidized, and NADP⁺ is reduced to NADPH. A lactone (cyclic ester) intermediate, 6-phosphogluconolactone, is formed.
- Equation:
Glucose-6-phosphate + NADP⁺ → 6-Phosphogluconolactone + NADPH + H⁺ - Significance: This is the rate-limiting and committed step of the entire Pentose Phosphate Pathway. The activity of G6PD is highly regulated.
2. Hydrolysis of 6-Phosphogluconolactone
- Enzyme: 6-Phosphogluconolactonase
- Reaction: The lactone ring is hydrolyzed to an open-chain carboxylic acid, 6-phosphogluconate.
- Equation:
6-Phosphogluconolactone + H₂O → 6-Phosphogluconate - Significance: This step prepares the molecule for the second oxidative reaction.
3. Oxidative Decarboxylation of 6-Phosphogluconate
- Enzyme: 6-Phosphogluconate Dehydrogenase
- Reaction: 6-phosphogluconate undergoes oxidative decarboxylation, meaning it is oxidized (another molecule of NADP⁺ is reduced to NADPH) and a molecule of CO₂ is released. The product is Ribulose-5-phosphate.
- Equation:
6-Phosphogluconate + NADP⁺ → Ribulose-5-phosphate + NADPH + H⁺ + CO₂ - Significance: This reaction generates the second molecule of NADPH and the first pentose phosphate, which serves as the entry point into the non-oxidative phase.
Summary of the Oxidative Phase:
The net reaction for the oxidative phase is:
→
Ribulose-5-phosphate + 2 NADPH + 2 H⁺ + CO₂
Key Takeaways from the Oxidative Phase:
- Two molecules of NADPH are produced per molecule of glucose-6-phosphate.
- One molecule of CO₂ is released.
- Ribulose-5-phosphate (a pentose sugar) is the final product.
- G6PD is the critical, rate-limiting enzyme.
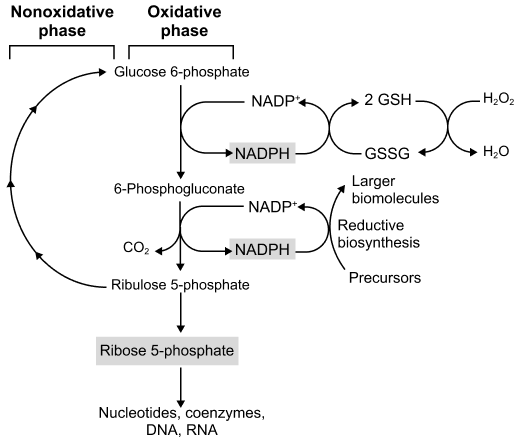
The Non-Oxidative (Reversible) Phase
The non-oxidative phase is a series of reversible reactions that interconvert various sugar phosphates. Its primary functions are:
- Conversion of Ribulose-5-Phosphate: To other pentose phosphates, including ribose-5-phosphate (essential for nucleotide synthesis).
- Recycling of Carbon Skeletons: To produce glycolytic intermediates (fructose-6-phosphate and glyceraldehyde-3-phosphate) from excess pentose phosphates, linking the PPP back to glycolysis.
- Flexibility: The reversibility allows the cell to adjust the production of ribose-5-phosphate and NADPH according to its needs.
Key Enzymes and Reactions of the Non-Oxidative Phase
This phase involves three main enzymes: an isomerase, an epimerase, and two transketolases/transaldolases.
1. Interconversion of Pentose Phosphates
The ribulose-5-phosphate generated in the oxidative phase needs to be converted into other pentose sugars.
a) Ribulose-5-Phosphate Isomerase
- Enzyme: Ribose-5-phosphate Isomerase
- Reaction: Converts the ketose sugar ribulose-5-phosphate into the aldose sugar ribose-5-phosphate. This is crucial as ribose-5-phosphate is the direct precursor for nucleotide synthesis.
- Equation:
Ribulose-5-phosphate ⇌ Ribose-5-phosphate
b) Ribulose-5-Phosphate Epimerase
- Enzyme: Xylulose-5-phosphate Epimerase
- Reaction: Converts ribulose-5-phosphate into another ketose sugar, xylulose-5-phosphate, which is important for subsequent transketolase reactions.
- Equation:
Ribulose-5-phosphate ⇌ Xylulose-5-phosphate
2. Transketolase and Transaldolase Reactions (The "Shunt" Part)
These two enzymes are responsible for moving two-carbon and three-carbon units between sugar phosphates to produce glycolytic intermediates.
a) Transketolase
- Enzyme: Transketolase
- Cofactor: Requires Thiamine Pyrophosphate (TPP).
- Function: Transfers a two-carbon (ketol) unit.
- First Reaction: Transfers 2 carbons from Xylulose-5-phosphate (5C) to Ribose-5-phosphate (5C), producing Glyceraldehyde-3-phosphate (3C) and Sedoheptulose-7-phosphate (7C).
b) Transaldolase
- Enzyme: Transaldolase
- Function: Transfers a three-carbon unit.
- Reaction: Transfers 3 carbons from Sedoheptulose-7-phosphate (7C) to Glyceraldehyde-3-phosphate (3C), producing Erythrose-4-phosphate (4C) and Fructose-6-phosphate (6C).
c) Second Transketolase Reaction
- Enzyme: Transketolase (again, requires TPP)
- Reaction: Transfers 2 carbons from another Xylulose-5-phosphate (5C) to Erythrose-4-phosphate (4C), producing another Glyceraldehyde-3-phosphate (3C) and another Fructose-6-phosphate (6C).
Overall Summary of the Non-Oxidative Phase
If 3 molecules of glucose-6-phosphate enter the oxidative phase, they produce 3 molecules of ribulose-5-phosphate and 6 NADPH. These 3 molecules of ribulose-5-phosphate are then processed through the non-oxidative phase:
These glycolytic intermediates can then enter glycolysis, be used for gluconeogenesis, or be recycled to continue the PPP.
Flexibility of the PPP
The reversibility of the non-oxidative phase is key, allowing the pathway to operate in different modes:
- If the cell needs more NADPH than ribose-5-phosphate: The oxidative phase is active, and pentose phosphates are recycled back to glucose-6-phosphate to maintain the flow.
- If the cell needs more ribose-5-phosphate than NADPH: The oxidative phase can be bypassed, and glycolytic intermediates can enter the non-oxidative phase in reverse to produce ribose-5-phosphate.
- If the cell needs both NADPH and ATP: The oxidative phase produces NADPH, and the non-oxidative phase converts pentose phosphates into F6P and G3P, which then enter glycolysis for ATP production.
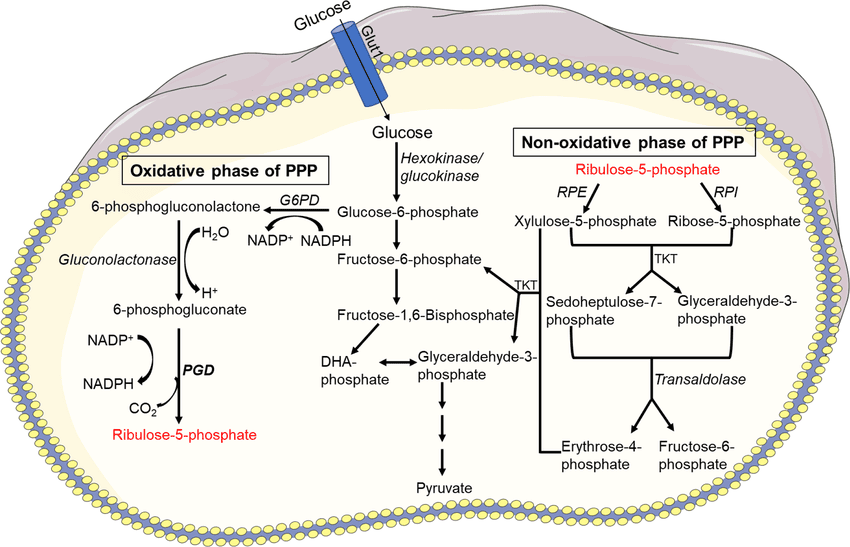
Primary Tissues/Cells of Activity
The activity of the PPP varies significantly among different tissues, directly reflecting their metabolic demands for its key products: NADPH and ribose-5-phosphate.
Tissues with High Demand for NADPH:
Liver (Hepatocytes)
The liver is a central metabolic hub with a high demand for NADPH for:
- Fatty acid synthesis
- Cholesterol and steroid synthesis
- Drug detoxification (cytochrome P450 system)
Adipose Tissue (Adipocytes)
Adipocytes are specialized for fat storage and have a very high demand for NADPH to support the massive amount of fatty acid synthesis that occurs here.
Red Blood Cells (Erythrocytes)
RBCs lack mitochondria and are constantly exposed to oxidative stress. The PPP is their only source of NADPH for antioxidant defense, used to maintain reduced glutathione (GSH) and protect the cell.
Steroidogenic Tissues
Tissues like the adrenal cortex, testes, and ovaries are primary sites of steroid hormone synthesis and have a high demand for NADPH for these hydroxylation reactions.
Mammary Gland (Lactating)
During lactation, the mammary gland synthesizes large amounts of fatty acids for milk production, requiring a high supply of NADPH.
Tissues with High Demand for Ribose-5-Phosphate:
Rapidly Dividing Cells
Tissues like bone marrow, skin, intestinal mucosa, and tumors are continuously proliferating and require constant DNA and RNA synthesis. They have a high demand for ribose-5-phosphate for nucleotide synthesis.
The non-oxidative phase can be reversed in these cells to primarily produce ribose-5-phosphate from glycolytic intermediates.
Pentose Phosphate Pathway Read More »

Gluconeogenesis
GLUCONEOGENESIS
The term "gluconeogenesis" literally means "new formation of glucose" (from Greek: glykys = sweet, neos = new, genesis = origin). It is a metabolic pathway that results in the generation of glucose from non-carbohydrate carbon substrates such as lactate, glycerol, and certain amino acids.
Primary Purpose:
The purpose of gluconeogenesis is to maintain blood glucose homeostasis, especially during periods when carbohydrate intake is insufficient (e.g., fasting, starvation, prolonged exercise).
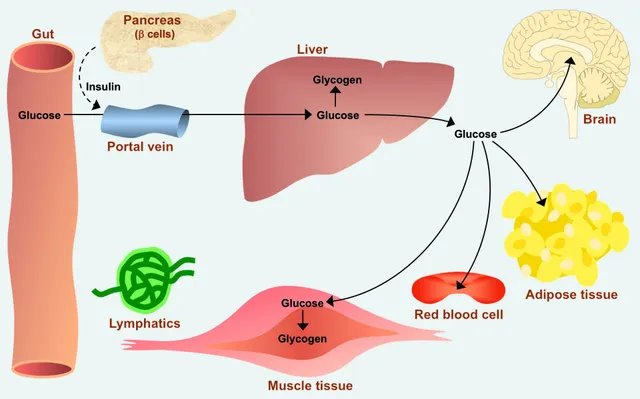
Why is this critical? The brain and red blood cells rely almost exclusively on glucose for their energy needs. Without gluconeogenesis, blood glucose levels would drop dangerously low (hypoglycemia) once glycogen stores are depleted, leading to severe physiological consequences.
Primary Tissues/Organs:
Gluconeogenesis primarily occurs in two organs:
- Liver (Hepatic Gluconeogenesis): This is the major site of gluconeogenesis. The liver can synthesize glucose and release it into the bloodstream for use by other tissues. Approximately 90% of all gluconeogenesis occurs in the liver.
- Kidney (Renal Gluconeogenesis): The kidneys also play a significant role, especially during prolonged fasting. The kidney can contribute up to 10% of glucose production during an overnight fast, and up to 40% during prolonged starvation.
Key Precursors:
Gluconeogenesis utilizes various non-carbohydrate molecules as starting materials. These precursors are ultimately converted into oxaloacetate, which then proceeds through the pathway. The three main classes are:
- Origin: Produced by anaerobic glycolysis in actively contracting skeletal muscle and in red blood cells.
- Conversion: Lactate is transported to the liver, where it is converted back to pyruvate by lactate dehydrogenase. This cycle (muscle lactate to liver glucose) is known as the Cori Cycle.
- Origin: Derived primarily from the breakdown of muscle protein, especially during fasting.
- Conversion: The carbon skeletons of many amino acids can be converted into pyruvate or TCA cycle intermediates (e.g., α-ketoglutarate, succinyl-CoA). Alanine is particularly important, forming the Glucose-Alanine Cycle.
- Note: Fatty acids cannot be directly converted to glucose in animals because the conversion of acetyl-CoA (from fatty acid breakdown) to pyruvate or oxaloacetate is not possible.
- Origin: Released during the hydrolysis of triglycerides (fats) in adipose tissue.
- Conversion: Glycerol is transported to the liver, where it is phosphorylated and then oxidized to dihydroxyacetone phosphate (DHAP). DHAP is an intermediate in both glycolysis and gluconeogenesis, readily entering the pathway.
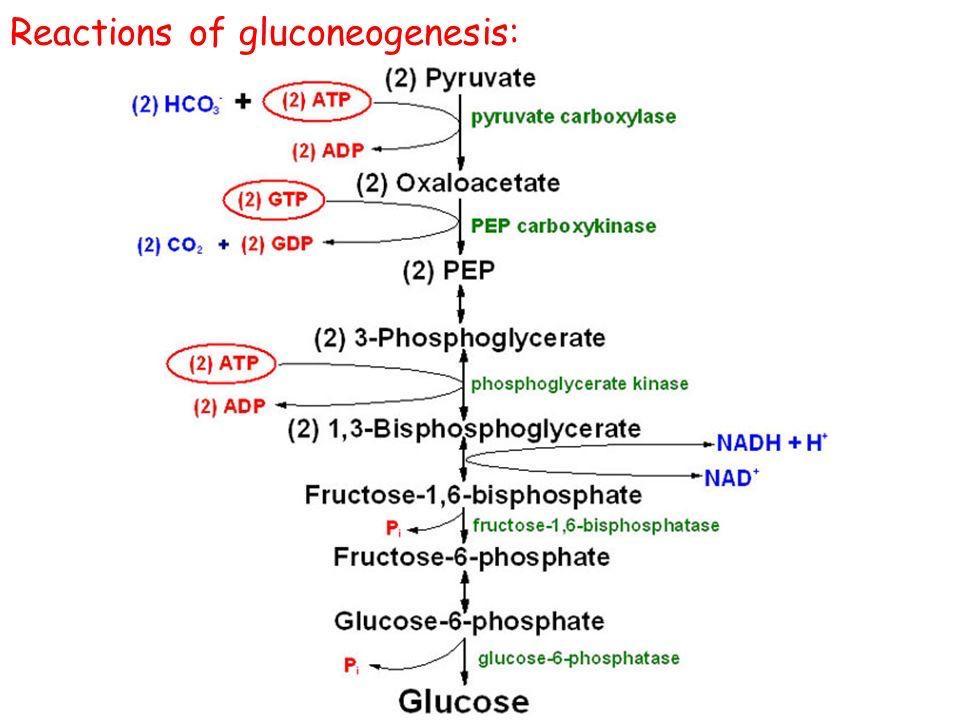
Major Steps and Bypassing Irreversible Glycolysis Reactions
Gluconeogenesis is NOT simply the reversal of glycolysis. While it shares many reversible steps, there are three highly exergonic (irreversible) steps in glycolysis that must be bypassed by different enzymes in gluconeogenesis. These bypasses are crucial for the pathway to be thermodynamically favorable and for regulatory control.
Overview of the Pathway (from Pyruvate to Glucose)
The overall process can be thought of as reversing glycolysis, but with four unique "bypass" reactions:
- Bypass 1: Pyruvate → Phosphoenolpyruvate (PEP)
- Bypass 2: Fructose-1,6-bisphosphate → Fructose-6-phosphate
- Bypass 3: Glucose-6-phosphate → Glucose
Detailed Steps & Key Enzymes
Let's start from pyruvate, a common entry point for lactate and some amino acids.
1. Pyruvate to Phosphoenolpyruvate (PEP) - The First Bypass
This bypass replaces the highly irreversible pyruvate kinase step of glycolysis. It requires two enzymes and crosses the mitochondrial membrane.
Step 1a: Pyruvate to Oxaloacetate (in Mitochondria)
- Enzyme: Pyruvate Carboxylase (PC)
- Reaction: Pyruvate + CO₂ + ATP → Oxaloacetate + ADP + Pi
- Cofactor: Biotin (carries CO₂)
- Key Point: This enzyme is in the mitochondrial matrix and is allosterically activated by acetyl-CoA. High acetyl-CoA signals that pyruvate should be directed towards glucose synthesis.
Step 1b: Oxaloacetate to PEP (Mitochondria and/or Cytosol)
Oxaloacetate cannot directly cross the mitochondrial membrane. It must first be converted via one of two options, often involving a malate shuttle, to generate cytosolic NADH which is needed later.
- Enzyme: PEP Carboxykinase (PEPCK)
- Reaction: Oxaloacetate + GTP → PEP + GDP + CO₂
2. PEP to Fructose-1,6-bisphosphate
From PEP, the pathway essentially reverses the reversible steps of glycolysis using the same enzymes, but in the reverse direction:
- PEP → 2-Phosphoglycerate → 3-Phosphoglycerate (via Enolase, Phosphoglycerate mutase)
- 3-Phosphoglycerate → 1,3-Bisphosphoglycerate (via Phosphoglycerate kinase, consuming ATP)
- 1,3-Bisphosphoglycerate → Glyceraldehyde-3-phosphate (via Glyceraldehyde-3-phosphate dehydrogenase, consuming NADH)
- Glyceraldehyde-3-phosphate ↔ Dihydroxyacetone phosphate (DHAP) (via Triose phosphate isomerase). DHAP from glycerol enters here.
- Glyceraldehyde-3-phosphate + DHAP → Fructose-1,6-bisphosphate (via Aldolase)
3. Fructose-1,6-bisphosphate to Fructose-6-phosphate - The Second Bypass
This bypass replaces the irreversible phosphofructokinase-1 (PFK-1) step of glycolysis.
- Enzyme: Fructose-1,6-bisphosphatase (FBPase-1)
- Reaction: Fructose-1,6-bisphosphate + H₂O → Fructose-6-phosphate + Pi
- Key Point: This is a hydrolysis reaction, releasing inorganic phosphate (Pi). It is a critical, reciprocally regulated point with PFK-1.
4. Fructose-6-phosphate to Glucose-6-phosphate
- Enzyme: Phosphohexose isomerase (reversible, same as glycolysis)
- Reaction: Fructose-6-phosphate ↔ Glucose-6-phosphate
5. Glucose-6-phosphate to Free Glucose - The Third Bypass
This bypass replaces the irreversible hexokinase/glucokinase step of glycolysis.
- Enzyme: Glucose-6-phosphatase
- Reaction: Glucose-6-phosphate + H₂O → Glucose + Pi
- Key Point: This enzyme is found primarily in the liver and kidney and is located in the endoplasmic reticulum membrane. It allows free glucose to be released into the bloodstream. Muscle cells lack this enzyme.
Summary of the Bypasses and Key Enzymes:
| Glycolysis Irreversible Step (Enzyme) | Gluconeogenesis Bypass Enzyme(s) | Location |
|---|---|---|
| Glucose → G6P (Hexokinase/Glucokinase) | Glucose-6-phosphatase | ER lumen (liver, kidney) |
| F6P → FBP (PFK-1) | Fructose-1,6-bisphosphatase (FBPase-1) | Cytosol |
| PEP → Pyruvate (Pyruvate Kinase) | 1. Pyruvate Carboxylase 2. PEP Carboxykinase (PEPCK) |
Mitochondria & Cytosol |
Energy Requirements
Synthesizing glucose from non-carbohydrate precursors is an energy-intensive, anabolic process. Let's calculate the ATP and GTP expenditure required to synthesize one molecule of glucose from two molecules of pyruvate.
Here's a breakdown of the energy-consuming steps:
- Pyruvate to Oxaloacetate (x2):
Catalyzed by Pyruvate Carboxylase, this step consumes 1 ATP per pyruvate.
Total cost: 2 ATP - Oxaloacetate to Phosphoenolpyruvate (PEP) (x2):
Catalyzed by PEP Carboxykinase, this step consumes 1 GTP per oxaloacetate.
Total cost: 2 GTP - 3-Phosphoglycerate to 1,3-Bisphosphoglycerate (x2):
Catalyzed by Phosphoglycerate Kinase, this step consumes 1 ATP per 3-phosphoglycerate.
Total cost: 2 ATP
Important Considerations:
- NADH Requirement: In addition to ATP and GTP, the pathway consumes 2 NADH during the conversion of 1,3-bisphosphoglycerate to glyceraldehyde-3-phosphate.
- Energy Balance and Futile Cycles: This significant energy investment highlights why gluconeogenesis and glycolysis must be reciprocally regulated. If both were active simultaneously, it would result in a "futile cycle," simply burning ATP and GTP to generate heat.
Reciprocal Regulation with Glycolysis
To prevent a wasteful "futile cycle," glycolysis and gluconeogenesis are reciprocally regulated. Conditions that activate one pathway typically inhibit the other. This occurs at the three irreversible steps.
Pyruvate Kinase ↔ Pyruvate Carboxylase / PEPCK
- High ATP & Alanine: Inhibit Pyruvate Kinase (Glycolysis).
- High Acetyl-CoA: Activates Pyruvate Carboxylase (Gluconeogenesis). This is a key signal from fatty acid breakdown, diverting pyruvate to glucose synthesis.
PFK-1 ↔ FBPase-1 (The Main Control Point)
- High ATP & Citrate: Inhibit PFK-1 (Glycolysis), signaling high energy.
- High AMP: Activates PFK-1 (Glycolysis) and inhibits FBPase-1 (Gluconeogenesis), signaling low energy.
- Fructose-2,6-bisphosphate (F2,6BP): This is the most potent regulator.
- High F2,6BP: Strongly activates PFK-1 (Glycolysis) and inhibits FBPase-1 (Gluconeogenesis).
- Low F2,6BP: Relieves inhibition of FBPase-1, promoting Gluconeogenesis.
- How is F2,6BP regulated? Its levels are controlled by a bifunctional enzyme (PFK-2/FBPase-2), which is in turn regulated by insulin (increases F2,6BP) and glucagon (decreases F2,6BP).
Hexokinase/Glucokinase ↔ Glucose-6-Phosphatase
- High Glucose-6-Phosphate (G6P): Inhibits Hexokinase (Glycolysis).
- Transcriptional Control: The gene expression of Glucose-6-Phosphatase is significantly upregulated by glucagon and inhibited by insulin, a long-term adaptation to fasting.
Summary of Reciprocal Regulation
| Regulatory Molecule | Glycolysis (Effect) | Gluconeogenesis (Effect) | Physiological Context |
|---|---|---|---|
| High ATP | ↓ (Inhibits) | ↑ (Activates) | High energy state |
| High AMP | ↑ (Activates) | ↓ (Inhibits) | Low energy state |
| High Citrate | ↓ (Inhibits) | -- | Abundant TCA intermediates |
| High Acetyl-CoA | ↓ (Inhibits) | ↑ (Activates) | Fatty acid oxidation |
| High F2,6BP | ↑ (Activates) | ↓ (Inhibits) | High glucose (Insulin) |
| Low F2,6BP | ↓ (Inhibits) | ↑ (Activates) | Low glucose (Glucagon) |
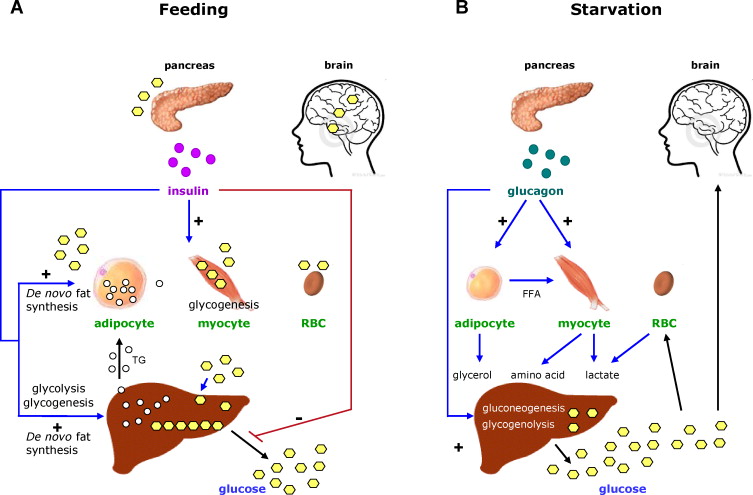
Hormonal Control
The activity of gluconeogenesis is tightly regulated by hormones that respond to changes in blood glucose levels and overall energy status. The primary hormones involved are glucagon, insulin, and cortisol.
The "Low Blood Glucose" Hormone
- Released from: Alpha cells of the pancreas.
- Stimulus: Low blood glucose (hypoglycemia).
- Target Tissue: Primarily the liver (muscle cells lack glucagon receptors).
- Mechanism: Glucagon binds to its receptor, increasing intracellular cAMP, which activates Protein Kinase A (PKA). PKA then phosphorylates the bifunctional PFK-2/FBPase-2 enzyme, activating its FBPase-2 domain. This decreases the concentration of Fructose-2,6-bisphosphate (F2,6BP).
- Overall Effect: Lower F2,6BP levels inhibit glycolysis (PFK-1) and activate gluconeogenesis (FBPase-1). PKA also promotes the gene expression of gluconeogenic enzymes. This stimulates gluconeogenesis to raise blood glucose.
The "High Blood Glucose" Hormone
- Released from: Beta cells of the pancreas.
- Stimulus: High blood glucose (hyperglycemia).
- Target Tissues: Liver, muscle, and adipose tissue.
- Mechanism: Insulin activates Protein Phosphatase 1 (PP1). PP1 dephosphorylates the bifunctional PFK-2/FBPase-2 enzyme, activating its PFK-2 domain. This increases the concentration of Fructose-2,6-bisphosphate (F2,6BP).
- Overall Effect: Higher F2,6BP levels activate glycolysis (PFK-1) and inhibit gluconeogenesis (FBPase-1). Insulin also suppresses the gene expression of gluconeogenic enzymes. This inhibits gluconeogenesis to lower blood glucose.
A "Stress" Hormone
- Released from: Adrenal cortex.
- Stimulus: Stress, prolonged fasting.
- Mechanism: Cortisol acts primarily by regulating gene expression over a longer time frame. It increases the transcription of genes for key gluconeogenic enzymes (Pyruvate Carboxylase, PEPCK, FBPase-1, Glucose-6-Phosphatase).
- Overall Effect: Cortisol enhances gluconeogenesis by providing both enzymes and substrates (by promoting muscle protein breakdown), contributing to maintaining blood glucose during prolonged stress or fasting.
Summary of Hormonal Effects on Gluconeogenesis:
| Hormone | Physiological Context | Effect on Gluconeogenesis | Primary Mechanism |
|---|---|---|---|
| Glucagon | Low blood glucose (fasting) | Stimulates | Activates PKA → decreases F2,6BP → activates FBPase-1; increases gene expression. |
| Insulin | High blood glucose (fed state) | Inhibits | Activates PP1 → increases F2,6BP → inhibits FBPase-1; decreases gene expression. |
| Cortisol | Stress, prolonged fasting | Stimulates | Increases gene expression of gluconeogenic enzymes; mobilizes amino acid precursors. |
A. Connection to Physiological States
Gluconeogenesis is vital for maintaining metabolic homeostasis under various conditions.
- Fasting (Short-Term): During an overnight fast (12-24 hours), gluconeogenesis supplements glycogenolysis. As glycogen stores deplete, it becomes the primary source of glucose.
- Precursors: Lactate, alanine, and glycerol.
- Hormones: High glucagon, low insulin.
- Starvation (Long-Term): After 24 hours, gluconeogenesis is essential for survival, providing all glucose for the brain and RBCs. To spare muscle protein, the body shifts to using fatty acids and ketone bodies as primary fuel.
- Hormones: High glucagon, low insulin, elevated cortisol.
- The kidneys significantly increase their contribution (up to 40%).
- Prolonged Exercise: During endurance exercise, gluconeogenesis helps maintain blood glucose. The liver efficiently recycles lactate (Cori Cycle) and alanine (Glucose-Alanine Cycle) produced by muscles.
- Hormones: Increased glucagon and epinephrine.
- High-Protein Diet: If carbohydrate intake is very low, gluconeogenesis ensures a sufficient supply of glucose by using amino acids derived from dietary protein as the primary precursors.
B. Clinical Relevance
Dysregulation of gluconeogenesis is central to several metabolic disorders.
A hallmark of diabetes is overproduction of glucose by the liver due to unrestrained gluconeogenesis, contributing significantly to hyperglycemia.
- Type 1: Absence of insulin means glucagon's effects are unopposed.
- Type 2: The liver becomes resistant to insulin's signal to suppress gluconeogenesis.
- Therapeutic Target: Metformin, a common diabetes drug, works primarily by inhibiting hepatic gluconeogenesis.
Heavy alcohol consumption can lead to hypoglycemia by inhibiting gluconeogenesis, especially in a fasted state.
- Mechanism: Alcohol metabolism generates a large amount of NADH. This high NADH/NAD⁺ ratio shifts key reactions away from gluconeogenesis precursors (converts pyruvate to lactate and oxaloacetate to malate), starving the pathway.
- Fructose-1,6-bisphosphatase Deficiency: A rare disorder where the FBPase-1 enzyme is deficient. Patients cannot synthesize glucose efficiently, leading to severe hypoglycemia and lactic acidosis, especially during fasting.
- Von Gierke's Disease (GSD Type I): A deficiency in Glucose-6-phosphatase, the final enzyme of both gluconeogenesis and glycogenolysis. This leads to severe fasting hypoglycemia, lactic acidosis, and an enlarged liver (hepatomegaly) because glucose cannot be released.
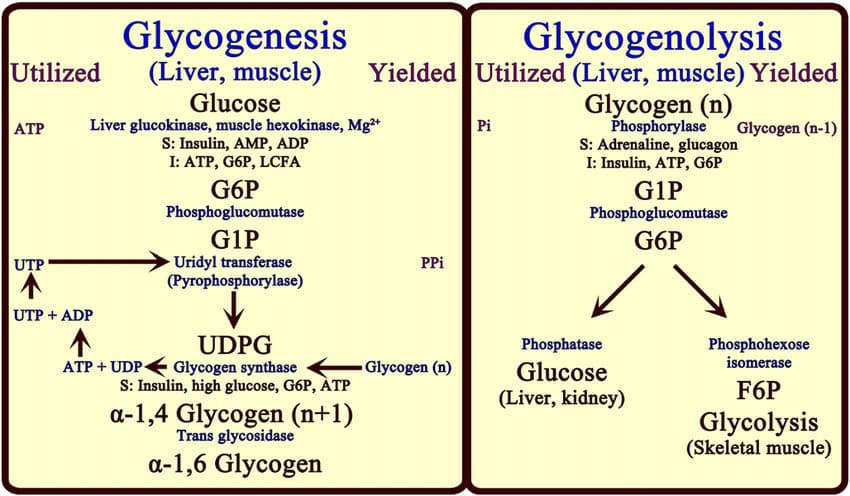
Glycogenolysis and Glycogenesis
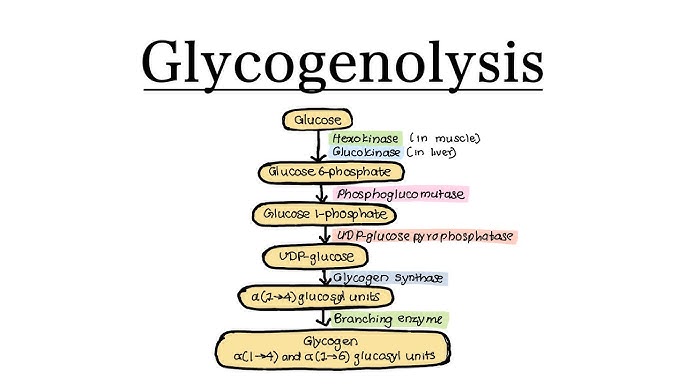
Key Enzymes
The breakdown of glycogen is a well-orchestrated process involving a few critical enzymes working in sequence. These enzymes ensure that glucose units are efficiently released from the glycogen molecule.
The three main enzymes (or enzyme complexes) are:
- Glycogen Phosphorylase
- Debranching Enzyme (which has two enzymatic activities)
- Phosphoglucomutase
Let's look at each one:
1. Glycogen Phosphorylase
- Function: This is the primary enzyme responsible for breaking down glycogen. It catalyzes the phosphorolysis (breaking a bond using inorganic phosphate, not water) of the
α(1,4)glycosidic bonds that link glucose units. - Mechanism: It removes glucose units one by one from the non-reducing ends of the glycogen molecule. The bond is broken by the addition of inorganic phosphate (Pᵢ), yielding glucose-1-phosphate.
- Limitation: Glycogen phosphorylase cannot break the
α(1,6)glycosidic bonds at the branch points. It stops cleaving when it reaches about four glucose residues away from a branch point, leaving behind a "limit dextrin."
2. Debranching Enzyme (Glycogen Debranching Enzyme)
Since glycogen phosphorylase cannot handle the branch points, this specialized enzyme complex is required. It has two distinct catalytic activities:
a. Oligo-α(1,4)-α(1,4)-glucantransferase activity (Transferase activity):
- Function: This activity transfers a block of three glucose residues from a branch to a non-reducing end of another chain. It forms a new
α(1,4)bond, making the chain longer and available for further action by glycogen phosphorylase.
b. Amylo-α(1,6)-glucosidase activity (Glucosidase activity):
- Function: After the transferase activity, this activity hydrolyzes the single remaining glucose residue at the
α(1,6)branch point, releasing it as free glucose (not glucose-1-phosphate). - Significance: This is the only step in glycogenolysis that directly produces free glucose (about 8% of the glucose from glycogen is released this way).
3. Phosphoglucomutase
- Function: This enzyme is responsible for interconverting glucose-1-phosphate and glucose-6-phosphate.
- Mechanism: Glycogen phosphorylase produces glucose-1-phosphate. For this glucose to enter glycolysis (as glucose-6-phosphate) or to be released into the bloodstream (as free glucose in the liver), it first needs to be converted. Phosphoglucomutase catalyzes this reversible isomerization.
Summary of Enzyme Action:
- Glycogen Phosphorylase removes glucose units as glucose-1-phosphate from the linear parts of glycogen.
- Debranching Enzyme "cleans up" the branch points: its transferase activity moves most of the branch, and its glucosidase activity releases the final branched glucose as free glucose.
- Phosphoglucomutase converts the glucose-1-phosphate into glucose-6-phosphate, which is the entry point for further metabolism.
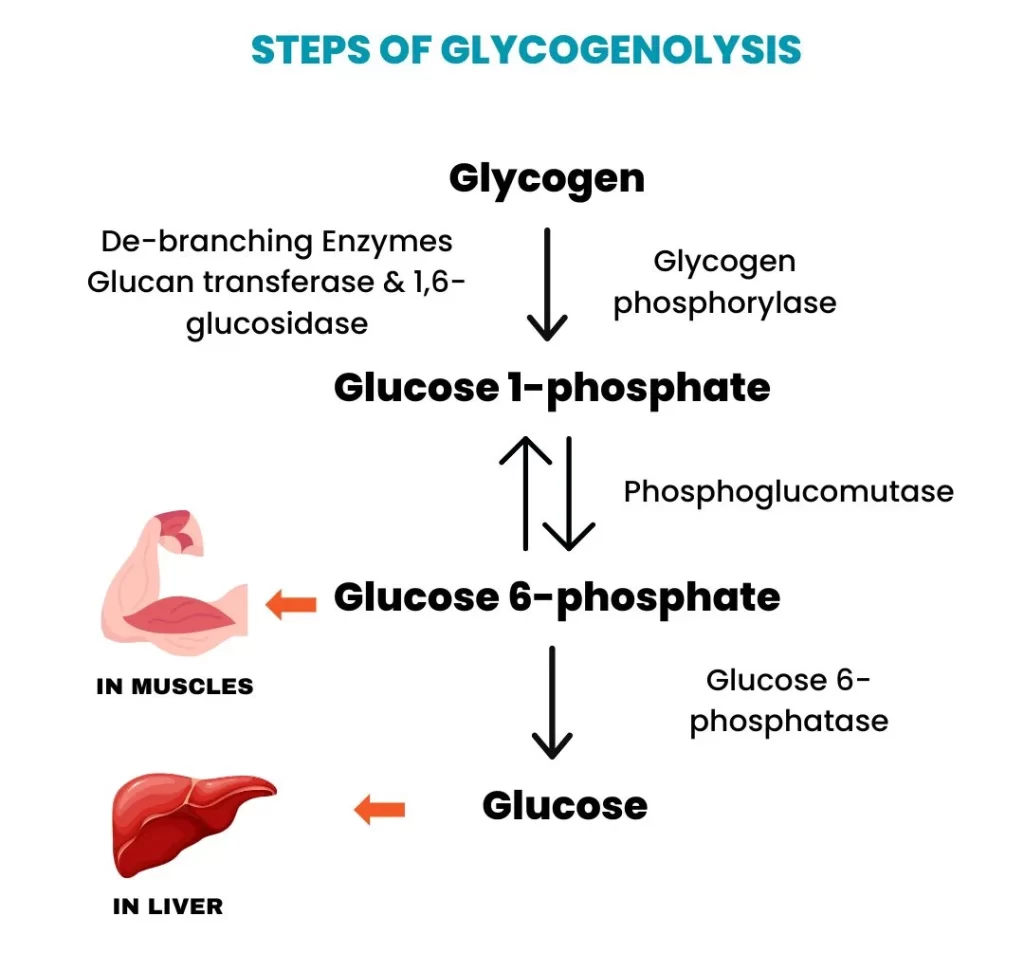
Steps of the Glycogenolysis Pathway
Here's a step-by-step breakdown of how glycogen is degraded to release glucose units, incorporating the enzymes we just discussed.
Overall Goal: To convert glycogen into individual glucose units that can be used for energy or released into the bloodstream.
Step 1: Phosphorolytic Cleavage of α(1,4) Glycosidic Bonds
- Enzyme: Glycogen Phosphorylase
- Action: Begins acting on the non-reducing ends of the glycogen molecule, cleaving the
α(1,4)glycosidic bonds. - Product: Each cleavage releases a molecule of glucose-1-phosphate (G1P). This process is called phosphorolysis because inorganic phosphate (Pᵢ) is used to break the bond.
- Limitation: The enzyme stops when it reaches approximately four glucose residues away from an
α(1,6)branch point, leaving a "limit dextrin."
Step 2: Remodeling of the Glycogen Molecule at Branch Points
- Enzyme: Debranching Enzyme
- Action: The debranching enzyme resolves the limit dextrin structure:
- Transferase Activity (Oligo-α(1,4)-α(1,4)-glucantransferase): Transfers a block of three glucose residues from the branch and reattaches them to a nearby non-reducing end via an
α(1,4)bond. - Glucosidase Activity (Amylo-α(1,6)-glucosidase): Hydrolyzes the single remaining
α(1,6)bond, releasing the glucose residue as free glucose.
- Transferase Activity (Oligo-α(1,4)-α(1,4)-glucantransferase): Transfers a block of three glucose residues from the branch and reattaches them to a nearby non-reducing end via an
- Result: Once the branch point is removed, glycogen phosphorylase can resume its action on the now-longer unbranched chain.
Step 3: Isomerization of Glucose-1-Phosphate to Glucose-6-Phosphate
- Enzyme: Phosphoglucomutase
- Action: The vast majority of glucose units released are in the form of G1P. For this to be used, it must be converted to glucose-6-phosphate (G6P). Phosphoglucomutase catalyzes this reversible isomerization.
- Significance:
- In Muscle: G6P directly enters the glycolysis pathway to produce ATP.
- In Liver: G6P can enter glycolysis or be dephosphorylated to free glucose for release into the bloodstream.
Step 4: Dephosphorylation of Glucose-6-Phosphate (Liver Specific)
- Enzyme: Glucose-6-phosphatase
- Location: Primarily found in the liver, but absent in muscle.
- Action: Removes the phosphate group from G6P, producing free glucose.
- Significance: This free glucose can then be transported out of the liver cell and into the bloodstream, raising blood glucose levels.
Simplified Flow:
Glycogen (n residues)
↓ (Glycogen Phosphorylase)
Glucose-1-Phosphate (G1P) + Glycogen (n-1 residues)
(Repeat for α(1,4) bonds)
At branch points:
Limit Dextrin
↓ (Debranching Enzyme - Transferase)
Lengthened α(1,4) chain + single α(1,6) linked glucose
↓ (Debranching Enzyme - Glucosidase)
Free Glucose
Back to G1P:
Glucose-1-Phosphate (G1P)
↓ (Phosphoglucomutase)
Glucose-6-Phosphate (G6P)
In Liver Only:
Glucose-6-Phosphate (G6P)
↓ (Glucose-6-phosphatase)
Free Glucose → Bloodstream
Products
The primary products of glycogenolysis depend on where the process is occurring (liver vs. muscle) and the specific enzymes involved.
Glucose-1-Phosphate (G1P)
- This is the main product of the action of glycogen phosphorylase, which cleaves the
α(1,4)glycosidic bonds. - It represents the vast majority (about 90-92%) of the glucose units released from glycogen.
Glucose-6-Phosphate (G6P)
- G1P is readily converted to G6P by phosphoglucomutase.
- In Muscle: G6P is the final form of glucose released from muscle glycogen and immediately enters glycolysis to produce ATP for muscle contraction. It cannot be converted to free glucose in muscle.
- In Liver: G6P is an intermediate that can either enter glycolysis or be further processed to free glucose for release into the bloodstream.
Free Glucose
- From Debranching Enzyme: A small amount of free glucose (about 8-10%) is produced directly by the amylo-α(1,6)-glucosidase activity of the debranching enzyme, which hydrolyzes the
α(1,6)branch points. - From Glucose-6-phosphatase (Liver-Specific): In the liver, the enzyme glucose-6-phosphatase dephosphorylates G6P to produce free glucose. This free glucose is then released into the bloodstream to maintain blood glucose homeostasis.
Summary of Products by Location:
- In Muscles: The primary product usable by the muscle cell is Glucose-6-Phosphate (G6P), which directly feeds into glycolysis. A small amount of free glucose is also produced, which then needs to be phosphorylated to G6P to enter glycolysis.
- In Liver: The primary product released into the bloodstream is Free Glucose. This is generated both directly by the debranching enzyme and, more significantly, by the dephosphorylation of G6P by glucose-6-phosphatase. The liver also produces G6P for its own energy needs.
In essence, glycogenolysis provides either glucose-6-phosphate for immediate energy use within the cell (muscle) or free glucose for systemic distribution (liver).
Glycogenolysis: Regulation
The breakdown of glycogen is under precise control, ensuring that glucose is mobilized only when needed. This regulation involves a combination of hormonal signaling and allosteric control, primarily targeting the key enzyme: Glycogen Phosphorylase.
A central concept is that Glycogen Phosphorylase exists in two forms:
- Glycogen Phosphorylase a (Active Form): The phosphorylated form, highly active.
- Glycogen Phosphorylase b (Less Active Form): The dephosphorylated form, less active and more sensitive to allosteric effectors.
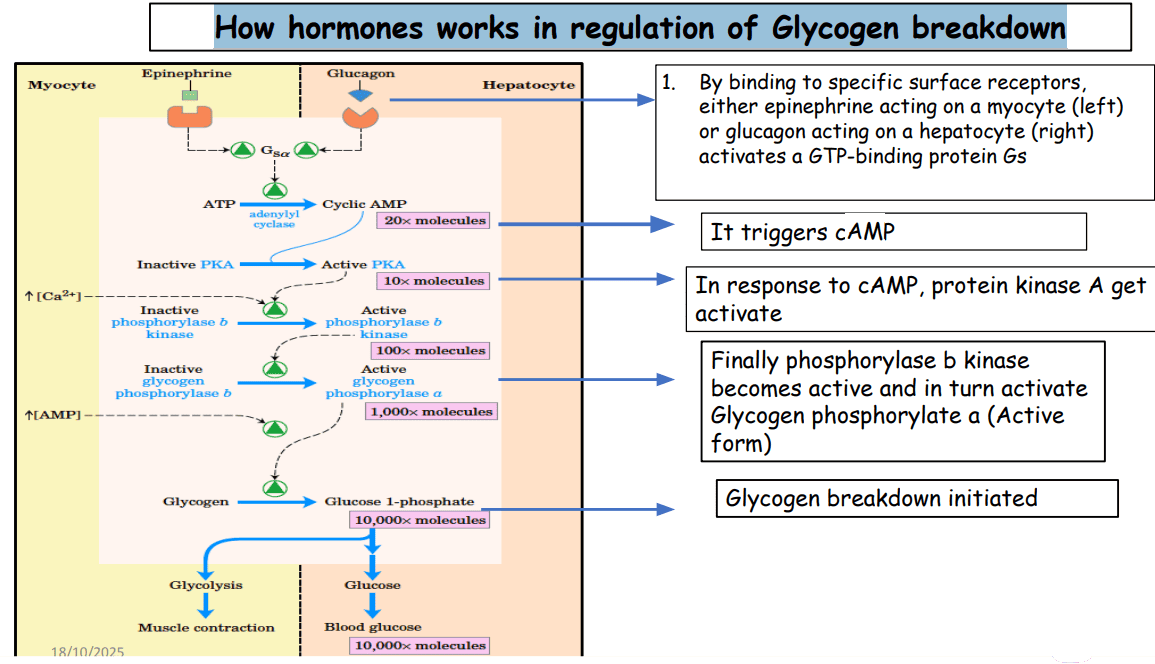
I. Hormonal Control (Covalent Modification via Phosphorylation/Dephosphorylation)
Hormones primarily regulate glycogenolysis by influencing the phosphorylation state of Glycogen Phosphorylase, converting it from the less active 'b' form to the active 'a' form.
Glucagon (Signals Low Blood Glucose)
- Trigger: Released from pancreatic α-cells in response to low blood glucose.
- Action: Primarily targets the liver.
- Mechanism: Glucagon binds to its receptor, activating a pathway that increases cyclic AMP (cAMP). cAMP activates Protein Kinase A (PKA), which in turn activates Phosphorylase Kinase. Finally, Phosphorylase Kinase phosphorylates Glycogen Phosphorylase b, converting it to the active 'a' form.
- Result: Enhanced glycogen breakdown in the liver and release of glucose into the bloodstream.
Epinephrine (Adrenaline - Signals Stress/Energy Demand)
- Trigger: Released from the adrenal medulla in response to stress or intense exercise.
- Action: Targets both the liver and skeletal muscles.
- Mechanism: Similar to glucagon, epinephrine binds to β-adrenergic receptors, increasing cAMP and activating the PKA cascade to convert phosphorylase 'b' to 'a'. In the liver, it can also act via α-adrenergic receptors to increase intracellular Ca²⁺, which also activates Phosphorylase Kinase.
- Result: In the liver, increased glucose release. In muscle, rapid provision of glucose-6-phosphate for immediate ATP production to support contraction.
Insulin (Signals High Blood Glucose)
- Trigger: Released from pancreatic β-cells in response to high blood glucose.
- Action: Promotes glucose storage and inhibits glucose mobilization.
- Mechanism: Insulin primarily counteracts glucagon and epinephrine by activating Protein Phosphatase 1 (PP1). PP1 dephosphorylates Glycogen Phosphorylase 'a', converting it back to the less active 'b' form, effectively turning off glycogenolysis.
II. Allosteric Control (Direct Ligand Binding)
Allosteric regulators bind directly to Glycogen Phosphorylase, rapidly altering its activity to meet immediate cellular needs.
In Skeletal Muscles (Responding to Energy Demand)
- AMP (Adenosine Monophosphate): A potent positive allosteric activator. High AMP signals low energy and activates Glycogen Phosphorylase 'b' even without phosphorylation, providing a rapid "on" switch during intense activity.
- ATP and Glucose-6-Phosphate (G6P): Both are negative allosteric inhibitors. High levels signal sufficient energy, inhibiting Glycogen Phosphorylase 'b' to conserve glycogen.
- Ca²⁺ (Calcium Ions): Released during muscle contraction. Ca²⁺ directly activates Phosphorylase Kinase, leading to the activation of Glycogen Phosphorylase. This directly couples glycogen breakdown to muscle activity.
In Liver (Responding to Blood Glucose Levels)
- Glucose: Acts as a negative allosteric inhibitor of Glycogen Phosphorylase 'a'. When glucose is abundant, it binds to the enzyme, making it a better substrate for dephosphorylation by PP1, effectively turning off glycogenolysis.
Summary of Regulatory Principles:
- Hormonal control (glucagon, epinephrine, insulin) initiates slower, broader responses by modulating the phosphorylation state of Glycogen Phosphorylase.
- Allosteric control (AMP, ATP, Ca²⁺, glucose) provides rapid, fine-tuning adjustments based on the immediate metabolic state of the cell.
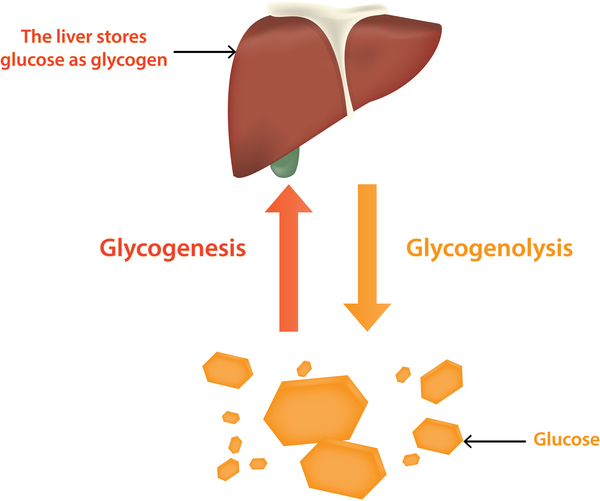
Glycogenesis
Glycogenesis is the metabolic pathway responsible for the synthesis of glycogen from glucose. It is the anabolic counterpart to glycogenolysis.
Purpose:
- To store excess glucose when supply is high (e.g., after a meal).
- To maintain blood glucose homeostasis by providing a readily mobilizable glucose reserve in the liver.
- To provide an immediately available energy source for muscle contraction in skeletal muscle.
- To store glucose efficiently without causing osmotic stress, as glycogen is a large polymer.
Location
Glycogenesis occurs primarily in two main tissues, each with a distinct physiological role for the stored glycogen:
Liver:
- Quantity: The liver stores the largest percentage of glycogen by weight (up to 6-8% of its fresh weight).
- Role: Liver glycogen serves as the body's primary glucose reservoir for maintaining blood glucose homeostasis. When blood glucose levels drop, the liver breaks down its glycogen and releases free glucose into the bloodstream to supply other tissues, especially the brain and red blood cells.
Skeletal Muscles:
- Quantity: Skeletal muscles store a lower percentage of glycogen by weight (typically 1-2%), but due to the much larger total mass of muscle, the total amount of glycogen stored often exceeds that in the liver.
- Role: Muscle glycogen serves as a private fuel reserve for the muscle cells themselves. It is primarily used to generate ATP for muscle contraction. Unlike liver glycogen, it cannot be directly released as free glucose into the bloodstream.
Cellular Location: Within both liver and muscle cells, glycogenesis occurs in the cytosol. Glycogen itself is stored in the cytosol as granules, which also contain the enzymes responsible for its synthesis and breakdown.
Key Substrates/Inputs
To synthesize glycogen, the pathway requires specific building blocks and energy sources. The primary substrates are:
Glucose:
- This is the fundamental monosaccharide unit from which glycogen is constructed.
- In the cell, glucose first needs to be phosphorylated to Glucose-6-Phosphate (G6P). This phosphorylation serves several purposes:
- It traps glucose inside the cell, as phosphorylated sugars cannot easily cross the cell membrane.
- It activates glucose for subsequent metabolic reactions.
- The phosphorylation of glucose is catalyzed by:
- Hexokinase in most tissues (including muscle).
- Glucokinase in the liver and pancreatic β-cells.
ATP (Adenosine Triphosphate):
- ATP provides the energy for the initial phosphorylation of glucose to Glucose-6-Phosphate.
- It also provides energy in a later step for the activation of glucose into a UDP-glucose molecule.
UTP (Uridine Triphosphate):
- UTP is crucial for activating glucose, forming UDP-Glucose. This "activated" form of glucose is the direct donor of glucose units for glycogen synthesis.
A Primer (Pre-existing Glycogen or Glycogenin):
- Glycogen synthesis doesn't start from scratch. It requires a pre-existing glycogen molecule (a "primer") to which new glucose units can be added.
- If no glycogen primer is available, a special protein called Glycogenin acts as both an enzyme and a primer. Glycogenin auto-glucosylates itself, forming a short chain of glucose units to which glycogen synthase can then attach further units.
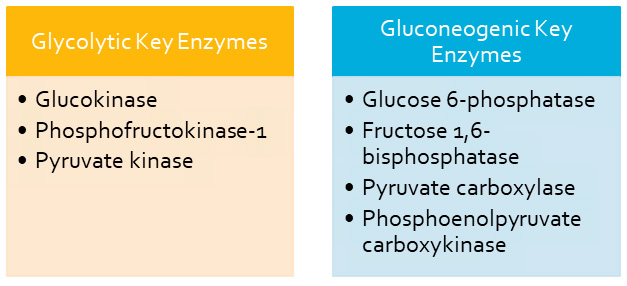
Key Enzymes
The synthesis of glycogen involves several distinct enzymatic steps. We'll highlight the most important ones here.
1. Hexokinase/Glucokinase
- Reaction:
Glucose + ATP → Glucose-6-Phosphate + ADP - Role: Catalyzes the initial phosphorylation of glucose, trapping it inside the cell.
2. Phosphoglucomutase
- Reaction:
Glucose-6-Phosphate ↔ Glucose-1-Phosphate - Role: Reversibly converts G6P to G1P, the precursor for the activated form of glucose.
3. UDP-Glucose Pyrophosphorylase
- Reaction:
Glucose-1-Phosphate + UTP ↔ UDP-Glucose + PPi - Role: Activates glucose by converting G1P into UDP-Glucose, the immediate donor of glucose units. The hydrolysis of the pyrophosphate (PPi) makes this reaction essentially irreversible.
4. Glycogen Synthase
- Reaction:
UDP-Glucose + Glycogenₙ → Glycogenₙ₊₁ + UDP - Role: This is the key regulatory enzyme. It adds glucose units from UDP-glucose to the non-reducing end of a glycogen primer via an
α(1,4)glycosidic bond.
5. Glycogen Branching Enzyme (Amylo-(1,4→1,6)-Transglucosidase)
- Reaction: Transfers a block of
α(1,4)-linked glucose residues to an interior residue via anα(1,6)bond. - Role: Introduces branches into the glycogen molecule.
- Significance: Branching increases solubility and creates numerous non-reducing ends, speeding up both synthesis and degradation.
6. Glycogenin
- Role: Essential for initiating new glycogen molecules. It acts as both a primer and an enzyme, creating a short glucose chain that Glycogen Synthase can then extend.
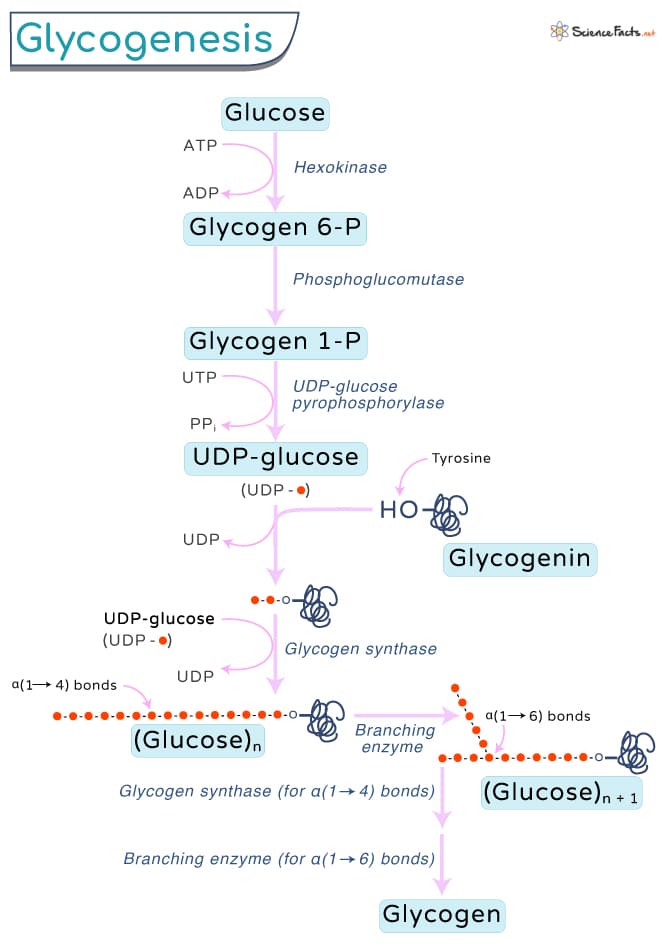
Steps of the Pathway
Glycogenesis can be broken down into a series of coordinated enzymatic reactions:
Step 1: Glucose Phosphorylation
Purpose: To trap and activate glucose inside the cell.
Enzyme: Hexokinase or Glucokinase.
Step 2: Isomerization
Purpose: To convert G6P into the isomer required for activation.
Enzyme: Phosphoglucomutase.
Step 3: Activation to UDP-Glucose
Purpose: To create an "activated" high-energy form of glucose.
Enzyme: UDP-Glucose Pyrophosphorylase.
Step 4: Initiation (Priming)
Purpose: To provide a starting point if no primer exists.
Enzyme: Glycogenin.
Glycogenin auto-glucosylates itself using UDP-Glucose to form a short α(1,4) chain.
Step 5: Elongation
Purpose: To add successive glucose units to the growing chain.
Enzyme: Glycogen Synthase.
Forms new α(1,4) glycosidic bonds.
Step 6: Branching
Purpose: To introduce branches for efficiency.
Enzyme: Glycogen Branching Enzyme.
Transfers a segment of 6-7 glucose units from an α(1,4) chain to an interior position via a new α(1,6) bond.
Products/Outputs
After traversing the steps of the pathway, the primary and most obvious product is:
Glycogen:
- This is the main polymeric carbohydrate storage molecule. It is a large, highly branched polymer of glucose units linked by
α(1,4)andα(1,6)glycosidic bonds. - Stored in the cytosol as granules, particularly abundant in the liver and skeletal muscle.
Beyond the main product, other outputs or byproducts include:
- UDP (Uridine Diphosphate): Released when Glycogen Synthase adds a glucose unit. It is then rephosphorylated back to UTP using ATP (
UDP + ATP ↔ UTP + ADP). - ADP (Adenosine Diphosphate): Released during the initial phosphorylation of glucose and when UDP is rephosphorylated.
- Inorganic Phosphate (Pi): Resulting from the hydrolysis of pyrophosphate (PPi) released during the formation of UDP-glucose.
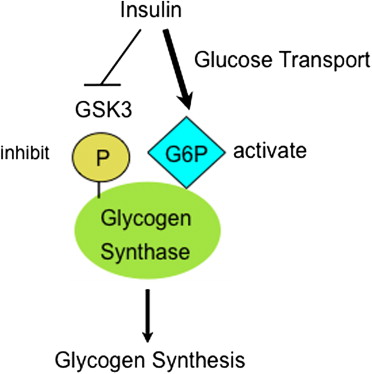
Regulation
The synthesis of glycogen is a tightly regulated process. The most important regulatory enzyme is Glycogen Synthase.
A. Hormonal Regulation (via Covalent Modification)
Hormones signal the body's metabolic state, leading to the phosphorylation or dephosphorylation of glycogen synthase to alter its activity.
Insulin (High Blood Glucose)
Effect: Promotes glycogenesis.
Mechanism: Insulin activates Protein Phosphatase 1 (PP1), which dephosphorylates Glycogen Synthase, converting it to its active 'a' form (GSa).
Glucagon (Low Blood Glucose)
Effect: Inhibits glycogenesis (in liver).
Mechanism: Glucagon activates Protein Kinase A (PKA), which phosphorylates Glycogen Synthase, converting it to its inactive 'b' form (GSb).
Epinephrine (Fight-or-Flight)
Effect: Inhibits glycogenesis (in liver & muscle).
Mechanism: Similar to glucagon, epinephrine activates PKA, which phosphorylates and inactivates Glycogen Synthase (GSb).
B. Allosteric Regulation
Allosteric regulators directly bind to enzymes in response to the cellular energy state.
- Glucose-6-Phosphate (G6P): Allosterically activates Glycogen Synthase (specifically the 'b' form). When G6P levels are high, it signals a surplus of glucose ready for storage, promoting glycogen synthesis even before hormonal signals fully kick in.
C. Other Factors
- Calcium (Ca²⁺) and AMP (Muscle Specific): During muscle contraction, Ca²⁺ is released and AMP levels rise. These signals strongly activate glycogen breakdown (glycogenolysis), which generally suppresses synthesis.
- Substrate Availability: The availability of UDP-Glucose also influences the rate of synthesis.
Summary of Regulation:
- High Glucose / Fed State: Insulin dominates. It leads to dephosphorylation of Glycogen Synthase, making it active (GSa). Result: Glycogen Synthesis.
- Low Glucose / Fasted State: Glucagon dominates (liver). It leads to phosphorylation of Glycogen Synthase, making it inactive (GSb). Result: Glycogen Breakdown.
- Stress / Exercise: Epinephrine dominates. It leads to phosphorylation and inactivation of Glycogen Synthase. Result: Glycogen Breakdown.
Glycogenolysis and Glycogenesis Read More »
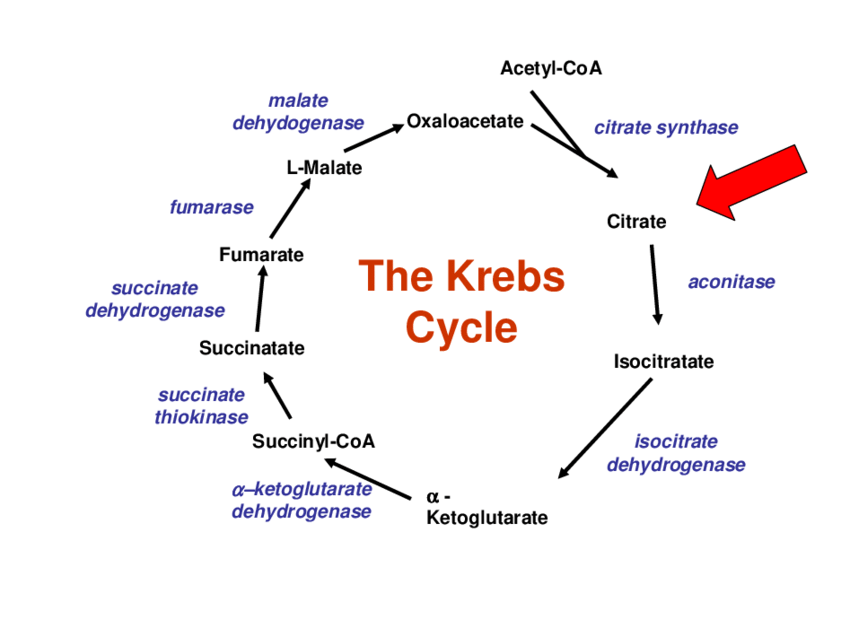
Tricarboxylic Acid (TCA) Cycle (Krebs Cycle / Citric Acid Cycle)
The Reactions of the Citric Acid Cycle
Now that Acetyl-CoA has been generated in the mitochondrial matrix, it enters the eight-step cyclical pathway. Each turn of the cycle processes one molecule of Acetyl-CoA, systematically oxidizing its two carbons to CO₂ while capturing high-energy electrons in the form of NADH and FADH₂. Let's examine each step.
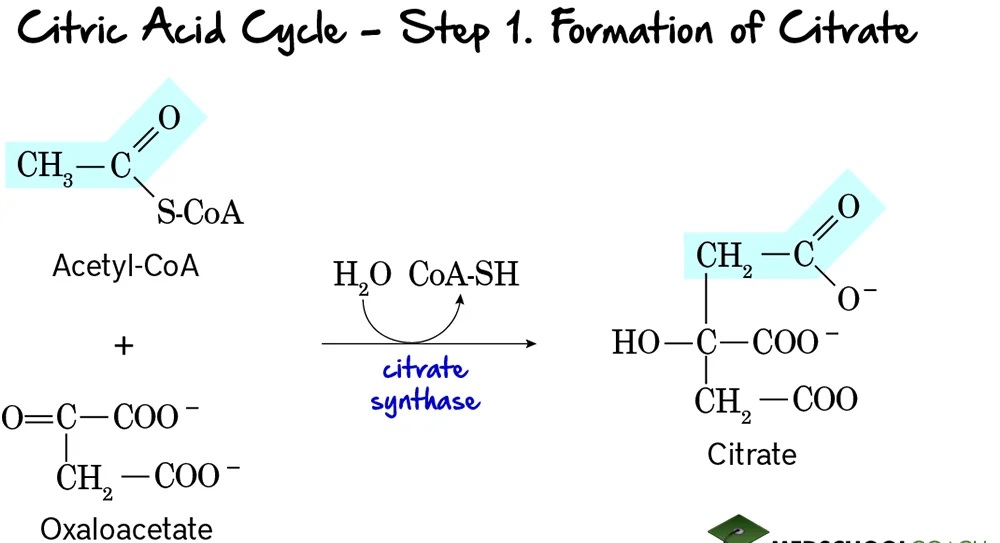
Step 1: Formation of Citrate
This is the entry point for the 2-carbon acetyl group into the citric acid cycle. It involves the condensation of a 2-carbon unit with a 4-carbon molecule to form a 6-carbon molecule.
Reaction:
Acetyl-CoA (a 2-carbon molecule) condenses with Oxaloacetate (a 4-carbon molecule). This reaction, accompanied by the hydrolysis of the thioester bond in Acetyl-CoA, forms Citrate, a 6-carbon tricarboxylic acid.
Key Features of Step 1:
- Enzyme: The reaction is catalyzed by Citrate Synthase. This is a crucial regulatory enzyme of the TCA cycle.
- Reactants: Acetyl-CoA and Oxaloacetate.
- Product: Citrate and Coenzyme A (CoA-SH).
- Type of Reaction: This is a condensation reaction.
- Irreversibility: The reaction is highly exergonic and essentially irreversible under cellular conditions, making it a key control point.
- Regulation: Citrate synthase is allosterically inhibited by high levels of ATP, NADH, succinyl-CoA, and its own product, citrate. These are all signals that the cell has a high energy charge and an abundance of metabolic intermediates.
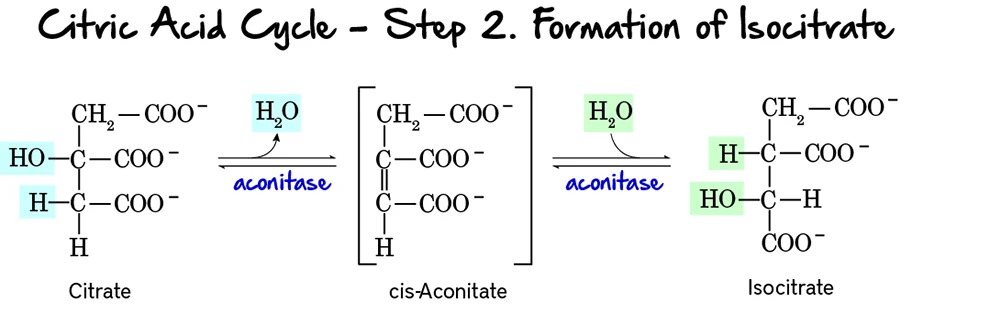
Step 2: Formation of Isocitrate
This step involves the isomerization of citrate to isocitrate. This rearrangement is crucial because the hydroxyl group of isocitrate is positioned to be oxidized in the next step.
Reaction:
Citrate, a tertiary alcohol, is isomerized to Isocitrate, a secondary alcohol. The reaction occurs in two substeps: first, a molecule of water is removed to form cis-Aconitate, and then water is re-added in a different position.
Key Features of Step 2:
- Enzyme: The enzyme catalyzing this reversible reaction is Aconitase. It contains an iron-sulfur cluster essential for its activity.
- Reactant: Citrate.
- Product: Isocitrate.
- Type of Reaction: An isomerization, specifically an intramolecular rearrangement involving dehydration and rehydration.
- Reversibility: The reaction is reversible, but the subsequent steps quickly consume isocitrate, pulling the reaction forward.
Purpose of this Step:
- Preparation for Oxidation: Citrate, being a tertiary alcohol, is not readily oxidizable. The isomerization to isocitrate, a secondary alcohol, positions the hydroxyl group at a carbon that can be easily oxidized in the next step.
- Stereospecificity: Aconitase catalyzes a stereospecific conversion, meaning it produces a specific isomer of isocitrate.
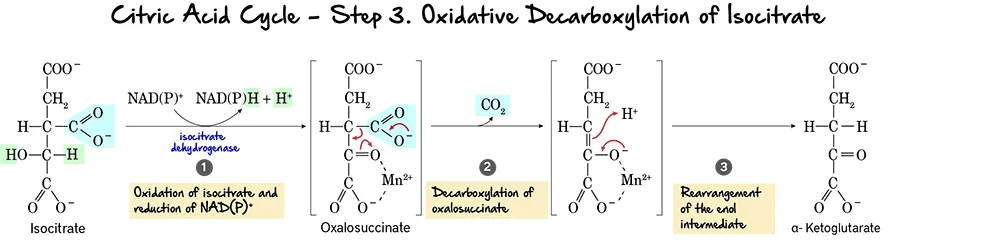
Step 3: Oxidative Decarboxylation of Isocitrate
This is the first oxidative step in the citric acid cycle, where the first molecule of carbon dioxide is released and the first NADH is produced.
Reaction:
Isocitrate undergoes an oxidative decarboxylation reaction. This involves two main parts:
- Oxidation: The hydroxyl group on isocitrate is oxidized to a keto group, reducing NAD⁺ to NADH.
- Decarboxylation: The beta-keto acid intermediate, Oxalosuccinate, immediately loses a molecule of carbon dioxide (CO₂), forming alpha-Ketoglutarate.
Key Features of Step 3:
- Enzyme: The reaction is catalyzed by Isocitrate Dehydrogenase. This enzyme requires
Mn²⁺as a cofactor. - Reactant: Isocitrate.
- Product: alpha-Ketoglutarate and CO₂.
- Electron Carriers Reduced:
NAD⁺is reduced toNADH. - ATP Change: 0 ATP directly produced.
Purpose of this Step:
- CO₂ Release: This is the first of two carbon atoms released as CO₂ from the original acetyl unit.
- NADH Production: The generation of NADH is vital for ATP production via oxidative phosphorylation.
- Regulation: Isocitrate Dehydrogenase is a crucial regulatory enzyme. It is allosterically activated by ADP (indicating low energy) and inhibited by ATP and NADH (indicating high energy).
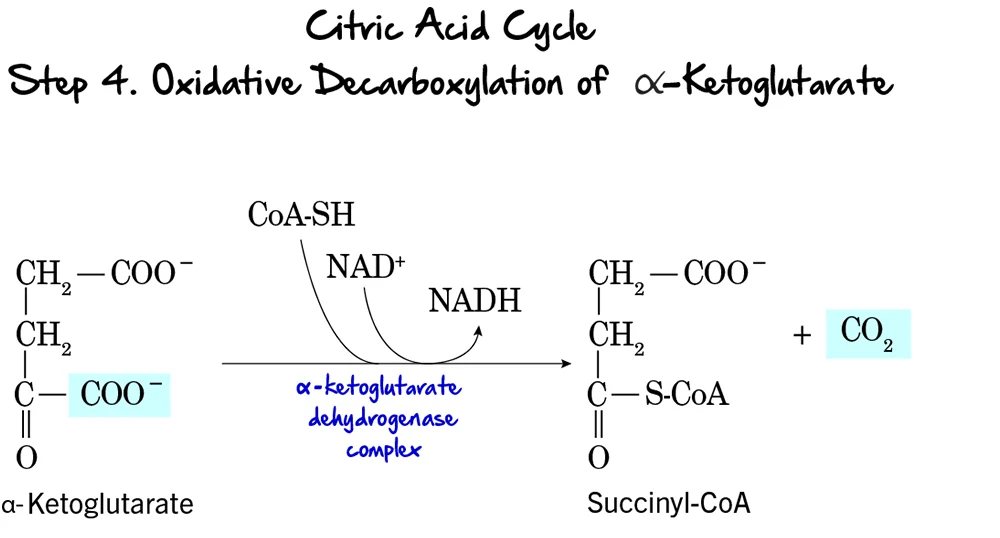
Step 4: Oxidative Decarboxylation of alpha-Ketoglutarate
This is the second and final oxidative decarboxylation step in the citric acid cycle. It is remarkably similar in mechanism to the pyruvate dehydrogenase complex reaction.
Reaction:
alpha-Ketoglutarate undergoes oxidative decarboxylation to form Succinyl-CoA. This complex reaction involves the release of another molecule of CO₂, the reduction of NAD⁺ to NADH, and the incorporation of Coenzyme A.
Key Features of Step 4:
- Enzyme: This reaction is catalyzed by the alpha-Ketoglutarate Dehydrogenase Complex. This is a multi-enzyme complex requiring several coenzymes (Thiamine pyrophosphate (TPP), Lipoamide, FAD, NAD⁺, and CoA-SH).
- Reactant: alpha-Ketoglutarate.
- Product: Succinyl-CoA, CO₂, and NADH.
- Electron Carriers Reduced:
NAD⁺is reduced toNADH. - ATP Change: 0 ATP directly produced.
Purpose of this Step:
- CO₂ Release: This is the second and last carbon atom released as CO₂. At this point, both carbons from the initial acetyl-CoA have been fully oxidized.
- NADH Production: This NADH contributes significantly to ATP production.
- Formation of a High-Energy Thioester: The formation of succinyl-CoA, with its high-energy thioester bond, primes the molecule for the substrate-level phosphorylation step that follows.
- Regulation: The alpha-Ketoglutarate Dehydrogenase Complex is another regulatory point. It is inhibited by its products, Succinyl-CoA and NADH, and also by high ATP levels.
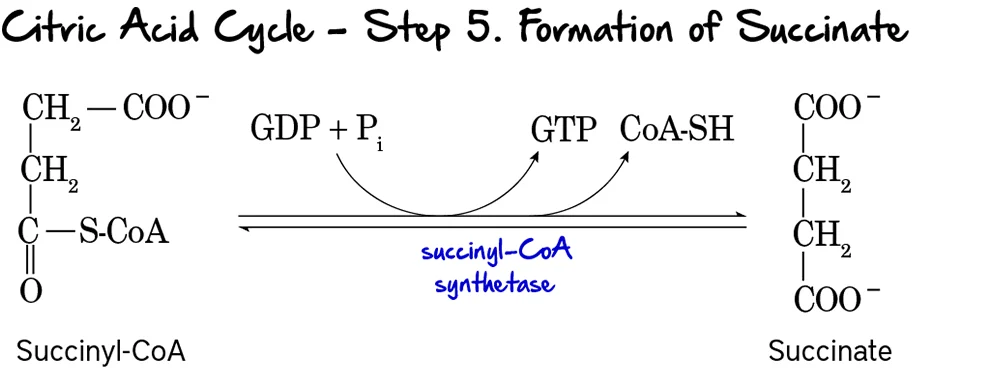
Step 5: Formation of Succinate (Substrate-Level Phosphorylation)
This is the only step in the Citric Acid Cycle that directly generates a high-energy phosphate compound (GTP or ATP) through substrate-level phosphorylation.
Reaction:
The high-energy thioester bond of Succinyl-CoA is hydrolyzed. The energy released drives the phosphorylation of GDP to GTP. Coenzyme A is released, and Succinate is formed.
Key Features of Step 5:
- Enzyme: Succinyl-CoA Synthetase (also known as Succinate Thiokinase).
- Reactant: Succinyl-CoA.
- Products: Succinate, CoA-SH, and GTP (or ATP).
- Energy Production: 1 GTP is produced per turn. GTP can be readily converted to ATP (
GTP + ADP ↔ GDP + ATP).
Purpose of this Step:
- ATP/GTP Generation: This provides a direct energy yield for the cell.
- Regeneration of Succinate: Succinate is now available for further processing.
- Removal of CoA: The release of free CoA is important for other enzyme complexes to function.
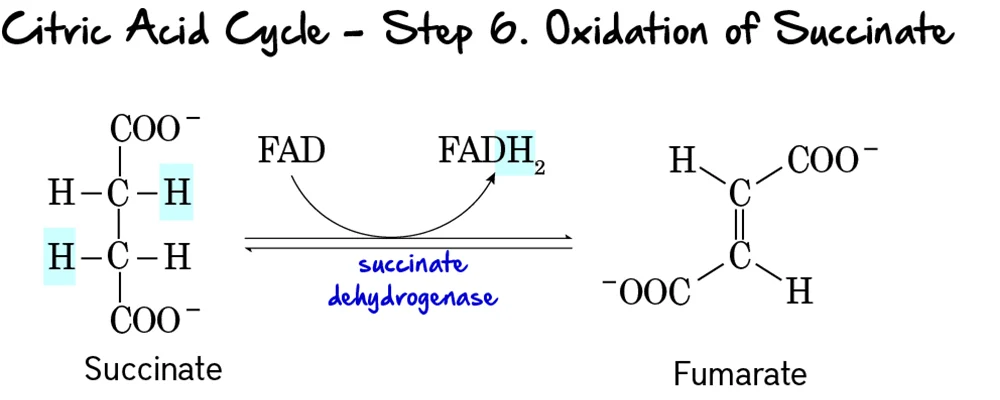
Step 6: Oxidation of Succinate
This is the second oxidative step in the cycle, where electrons are transferred to FAD, producing FADH₂.
Reaction:
Succinate is oxidized to Fumarate through the removal of two hydrogen atoms. These hydrogens are accepted by FAD, which is reduced to FADH₂. This reaction forms a double bond in fumarate.
Key Features of Step 6:
- Enzyme: Succinate Dehydrogenase. This enzyme is unique as it is an integral protein of the inner mitochondrial membrane and is directly part of the electron transport chain (Complex II).
- Reactant: Succinate.
- Products: Fumarate and FADH₂.
- Electron Carriers Reduced:
FADis reduced toFADH₂. - ATP Change: 0 ATP directly produced.
Purpose of this Step:
- FADH₂ Production: FADH₂ is another high-energy electron carrier that will donate its electrons to the ETC. It yields fewer ATP than NADH because it enters the ETC at a lower energy level.
- Connection to Electron Transport Chain: Being part of Complex II directly links the Citric Acid Cycle to the ETC, facilitating efficient electron transfer.
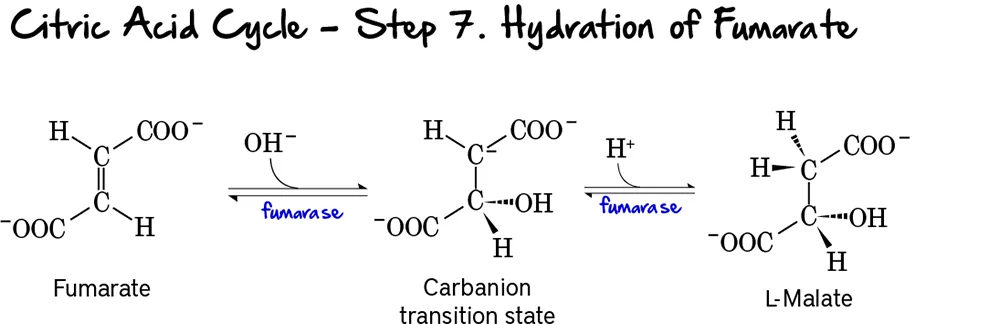
Step 7: Hydration of Fumarate
This step involves the stereospecific addition of water across the double bond of fumarate, forming L-malate.
Reaction:
Fumarate undergoes a hydration reaction, where a molecule of water is added across its double bond. This reaction forms L-Malate.
Key Features of Step 7:
- Enzyme: Fumarase (also known as Fumarate Hydratase).
- Reactant: Fumarate.
- Product: L-Malate.
- Type of Reaction: This is a hydration reaction.
- Stereospecificity: Fumarase is highly stereospecific, forming specifically L-malate (not D-malate).
- Reversibility: This reaction is reversible.
Purpose of this Step:
- Preparation for Oxidation: The addition of water creates a hydroxyl group on L-malate, which is necessary for the subsequent oxidation step.
- Regeneration of Oxaloacetate: This step is crucial for setting up the regeneration of oxaloacetate.
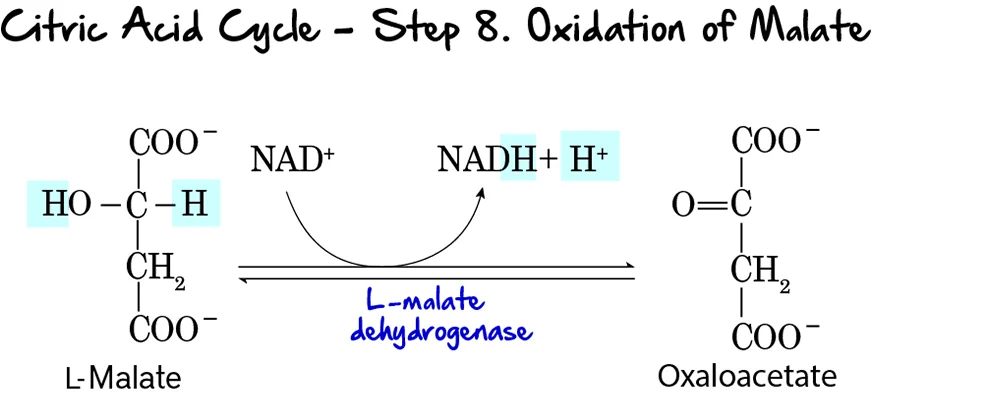
Step 8: Oxidation of Malate
This is the final step of the Citric Acid Cycle, regenerating oxaloacetate and producing the last NADH of the cycle.
Reaction:
L-Malate is oxidized to Oxaloacetate. During this oxidation, NAD⁺ is reduced to NADH and H⁺. This completes the regeneration of oxaloacetate, which is now ready to condense with another molecule of acetyl-CoA.
Key Features of Step 8:
- Enzyme: L-Malate Dehydrogenase.
- Reactant: L-Malate.
- Products: Oxaloacetate and NADH + H⁺.
- Electron Carriers Reduced:
NAD⁺is reduced toNADH. - Reversibility: This reaction has a highly positive standard free energy change (
ΔG°'), making it thermodynamically unfavorable. However, in the cell, the rapid consumption of oxaloacetate by citrate synthase (Step 1) pulls this reaction forward.
Purpose of this Step:
- Regeneration of Oxaloacetate: This is the most critical function, ensuring the cycle can continue to operate.
- NADH Production: This produces the third and final molecule of NADH generated directly within the cycle (per acetyl-CoA).
- Completion of the Cycle: With the regeneration of oxaloacetate, the cycle is complete.
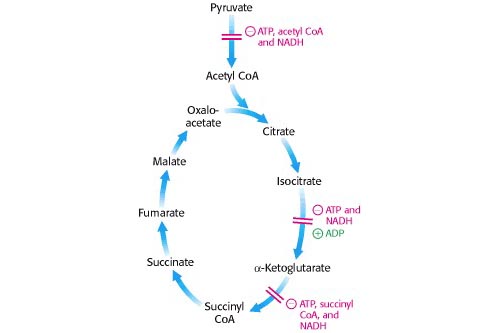
Regulation of the TCA Cycle
The TCA cycle is meticulously regulated to ensure that energy production aligns with the cell's demand. Regulation primarily occurs at the irreversible steps through allosteric control. The cycle slows down when the cell has ample ATP and speeds up when energy is needed.
Key Control Points within the Cycle:
Three main enzymes catalyze irreversible reactions and are thus primary targets for regulation:
- Citrate Synthase (Step 1)
- Isocitrate Dehydrogenase (Step 3) - Often considered a major rate-limiting step.
- α-Ketoglutarate Dehydrogenase Complex (Step 4)
Mechanisms of Regulation:
The TCA cycle's activity is finely tuned by several mechanisms, with allosteric modulation being the primary mode of control.
Allosteric Modulators:
This is the primary mode of regulation. Various molecules signal the cell's energy status, directly binding to and altering the activity of the regulatory enzymes.
Citrate Synthase (Step 1)
Activated by:
- ADP (low energy)
Inhibited by:
- ATP, NADH, Succinyl-CoA, Citrate (all are high energy signals or products).
Isocitrate Dehydrogenase (Step 3)
Activated by:
- ADP (low energy).
- Ca²⁺ (signals muscle contraction / energy demand).
Inhibited by:
- ATP, NADH (high energy signals).
α-Ketoglutarate Dehydrogenase (Step 4)
Activated by:
- Ca²⁺ (signals energy demand).
Inhibited by:
- Succinyl-CoA, NADH (product inhibition).
- ATP (high energy signal).
Other Regulatory Mechanisms:
- Covalent Modification: This is not a common regulatory mechanism for the core TCA cycle enzymes in eukaryotes. However, it is the primary control method for the Pyruvate Dehydrogenase Complex (PDC), which controls the entry of acetyl-CoA into the cycle.
- Supply of Acetyl-CoA: The activity of the PDC is a critical determinant of the flux into the TCA cycle, effectively controlling the primary fuel input.
Relating Regulation to Cellular Energy State:
The overall regulation ensures the TCA cycle's activity is finely tuned to the cell's energy demands:
- High Energy State (High ATP/ADP, High NADH/NAD⁺): When the cell has abundant energy, the products (ATP, NADH, citrate, succinyl-CoA) accumulate and act as allosteric inhibitors, slowing down the cycle to conserve fuel.
-
Low Energy State (Low ATP/ADP, Low NADH/NAD⁺): When the cell needs energy, ATP and NADH levels drop, while ADP/AMP levels rise. These conditions act as allosteric activators.
Ca²⁺also acts as a key activator, signaling increased metabolic activity, especially in contracting muscles. - Substrate Availability: The availability of acetyl-CoA and oxaloacetate also influences the flux through the cycle. The maintenance of oxaloacetate levels is crucial and involves anaplerotic reactions.
Amphibolic Nature and Anaplerotic Reactions
The TCA cycle is often presented as a purely catabolic pathway, but this is only half the story. The TCA cycle is, in fact, amphibolic, meaning it functions in both catabolic (breakdown) and anabolic (biosynthetic) processes.
1. Amphibolic Nature
The intermediates of the TCA cycle are not just steps on the way to CO₂; they are also crucial precursors for the biosynthesis of a wide variety of essential biomolecules.
- Catabolic Role: The primary catabolic role involves the complete oxidation of acetyl-CoA to CO₂, generating NADH, FADH₂, and GTP (ATP).
-
Anabolic Role (Examples of Intermediates as Precursors):
- Citrate: Can be transported out of the mitochondria to serve as a precursor for fatty acid and steroid biosynthesis.
- α-Ketoglutarate: A direct precursor for the synthesis of several non-essential amino acids (e.g., glutamate, glutamine) and purines.
- Succinyl-CoA: An intermediate used in the synthesis of porphyrins, which are components of heme (in hemoglobin).
- Fumarate & Oxaloacetate: Precursors for several non-essential amino acids. Oxaloacetate is also a starting point for gluconeogenesis (synthesis of glucose).
The diagram below illustrates some of these connections:
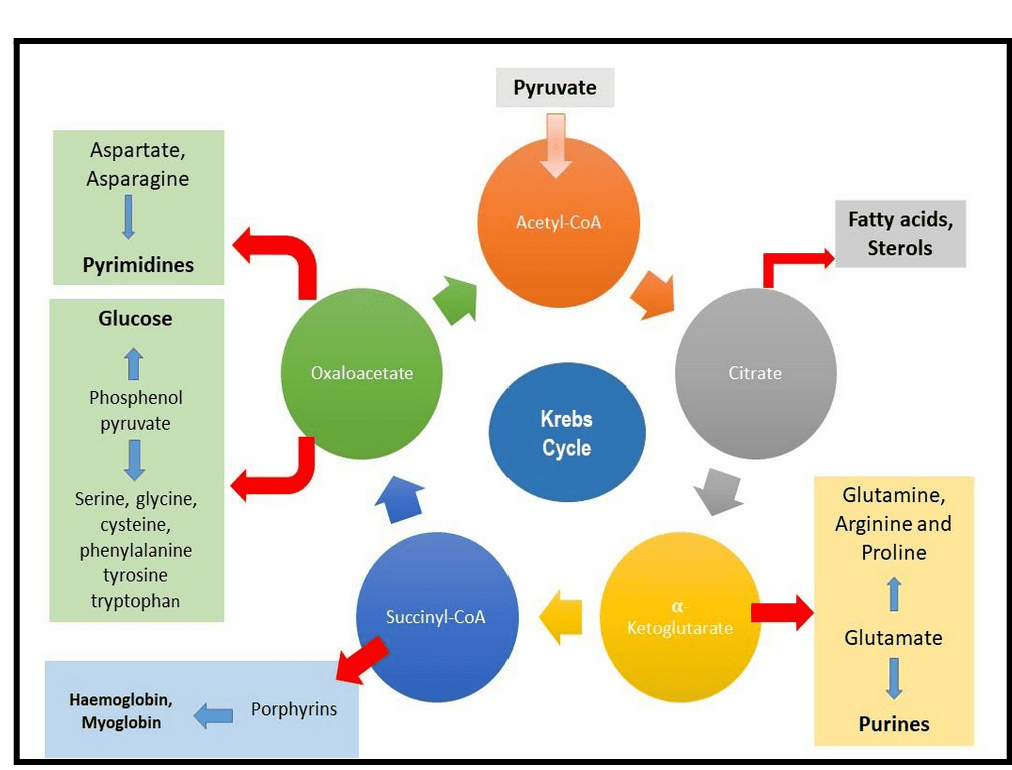
2. Anaplerotic Reactions
Because TCA cycle intermediates are frequently drawn off for biosynthesis, the cycle would quickly stop if these intermediates were not replenished. Reactions that replenish the intermediates of a metabolic pathway are called anaplerotic reactions (from Greek: "to fill up").
The most important anaplerotic reaction in mammals involves the replenishment of oxaloacetate:
-
Pyruvate Carboxylase: This enzyme catalyzes the carboxylation of pyruvate to oxaloacetate.
Pyruvate + HCO₃⁻ + ATP → Oxaloacetate + ADP + Pi
- Location: Primarily in the mitochondrial matrix of liver and kidney cells.
- Activator: This enzyme is allosterically activated by acetyl-CoA. This is a crucial regulatory link: when there's an abundance of acetyl-CoA but the cycle is low on oxaloacetate, pyruvate carboxylase steps in to produce more, ensuring the acetyl-CoA can be processed.
- Significance: This reaction is vital because if oxaloacetate is drained for anabolic processes (like gluconeogenesis), its replenishment ensures the TCA cycle can continue to operate.
Other anaplerotic reactions exist, such as replenishing intermediates from the breakdown of certain amino acids (e.g., glutamate to α-ketoglutarate). This highlights the incredible interconnectedness and flexibility of metabolism.
Tricarboxylic Acid (TCA) Cycle (Krebs Cycle / Citric Acid Cycle) Read More »
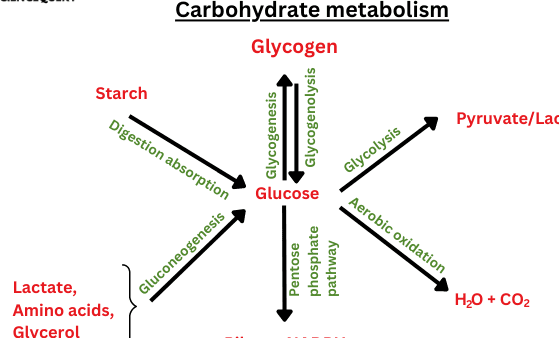
Carbohydrate Metabolism and Glycolysis
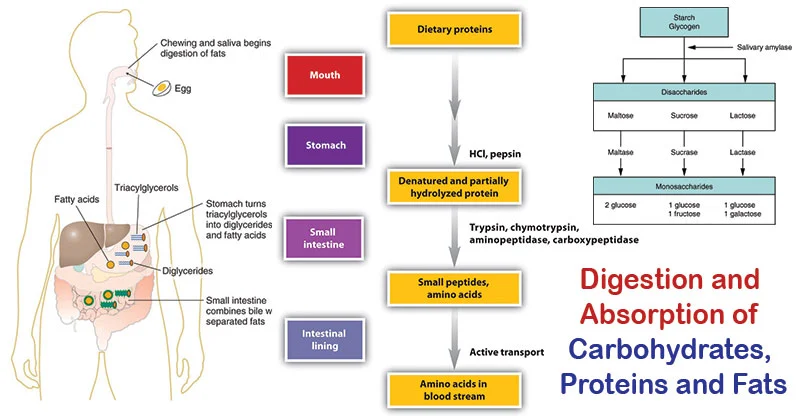
Digestion and Absorption of Dietary Carbohydrates
Before carbohydrates can be used by the body, complex forms (polysaccharides and disaccharides) must be broken down into monosaccharides for absorption. This process begins in the mouth and continues in the small intestine.
1. Digestion
Digestion involves the enzymatic hydrolysis of glycosidic bonds.
-
In the Mouth:
- Mechanical digestion (chewing).
- Salivary alpha-amylase (Ptyalin): Begins the breakdown of starch into smaller polysaccharides (dextrins) and some maltose. It's inactivated by stomach acid.
- In the Stomach: No significant carbohydrate digestion occurs here due to the acidic environment.
-
In the Small Intestine: This is where the bulk of carbohydrate digestion takes place.
- Pancreatic alpha-amylaseme: Continues breaking down starch and dextrins into maltose and other small polymers.
- Brush Border Enzymes: Located on the microvilli of intestinal cells, these are responsible for the final breakdown into monosaccharides.
- Maltase: Hydrolyzes maltose → two glucose molecules.
- Sucrase: Hydrolyzes sucrose → one glucose and one fructose.
- Lactase: Hydrolyzes lactose → one glucose and one galactose.
- Alpha-dextrinase (Isomaltase): Hydrolyzes alpha-1,6 bonds in limit dextrins, releasing glucose.
The end products are almost exclusively monosaccharides: glucose, fructose, and galactose.
2. Absorption
Monosaccharides are absorbed by intestinal epithelial cells (enterocytes) and then transported into the bloodstream.
-
Glucose and Galactose Absorption:
- Primarily absorbed by secondary active transport via the SGLT1 (Sodium-Glucose Cotransporter 1) protein. This requires energy and co-transports Na⁺ ions.
- From the enterocyte, they exit into the bloodstream via facilitated diffusion through the GLUT2 transporter.
-
Fructose Absorption:
- Absorbed solely by facilitated diffusion via the GLUT5 transporter. This does not require energy.
- From the enterocyte, it also exits into the bloodstream via the GLUT2 transporter.
3. Transport to the Liver
Once absorbed, these monosaccharides enter the hepatic portal vein, which carries them directly to the liver. The liver is the primary site for fructose and galactose metabolism, converting them into glucose or its intermediates.
Clinical Significance:
- Lactose Intolerance: A deficiency of the enzyme lactase, leading to maldigestion of lactose.
- Pancreatic Insufficiency: Conditions like cystic fibrosis can lead to maldigestion of starch.
- SGLT1 Deficiency: A rare genetic disorder where glucose and galactose cannot be absorbed.
Fates of Absorbed Monosaccharides (Especially Glucose)
After absorption, our monosaccharides (primarily glucose) enter the bloodstream. The body then has several crucial "fates" or pathways for this glucose, depending on energy needs and hormonal signals.
Visualizing the "Fates":
Imagine glucose as a central hub. From this hub, it can be directed down different "roads":
- Road 1: "Burn it for immediate power!" (Glycolysis → TCA → ETC)
- Road 2: "Store it for a quick pick-me-up!" (Glycogenesis)
- Road 3: "Pack it away for a rainy day!" (Conversion to Fat)
- Road 4: "Build other essential parts!" (Pentose Phosphate Pathway)
Energy Production (Oxidation):
- Goal: To generate ATP.
- Pathways: Glycolysis → Pyruvate Oxidation → TCA Cycle → Oxidative Phosphorylation.
- When: Continuously in most cells, especially during high energy demand.
Storage as Glycogen (Glycogenesis):
- Goal: To store excess glucose for later use.
- Where: Primarily in the liver and skeletal muscles.
- When: When blood glucose is high (e.g., after a meal), stimulated by insulin.
Conversion to Fat (Lipogenesis):
- Goal: To store excess energy in a long-term form when glycogen stores are full.
- Pathways: Glucose is converted to Acetyl-CoA, which is then used for fatty acid synthesis and stored as triglycerides in adipose tissue.
- When: When carbohydrate intake consistently exceeds energy needs.
Formation of Other Biomolecules (e.g., via Pentose Phosphate Pathway):
- Goal: To provide precursors for other essential molecules.
- Pathway: Pentose Phosphate Pathway (PPP) / Hexose Monophosphate Shunt (HMP Shunt):
- Produces NADPH: Crucial for biosynthesis (e.g., fatty acids) and protecting cells from oxidative stress.
- Produces Ribose-5-phosphate: A key component of nucleotides (DNA, RNA) and coenzymes (ATP, NADH).
- When: Continuously in cells with high demand for NADPH (e.g., liver, adipose tissue) or nucleotide synthesis.
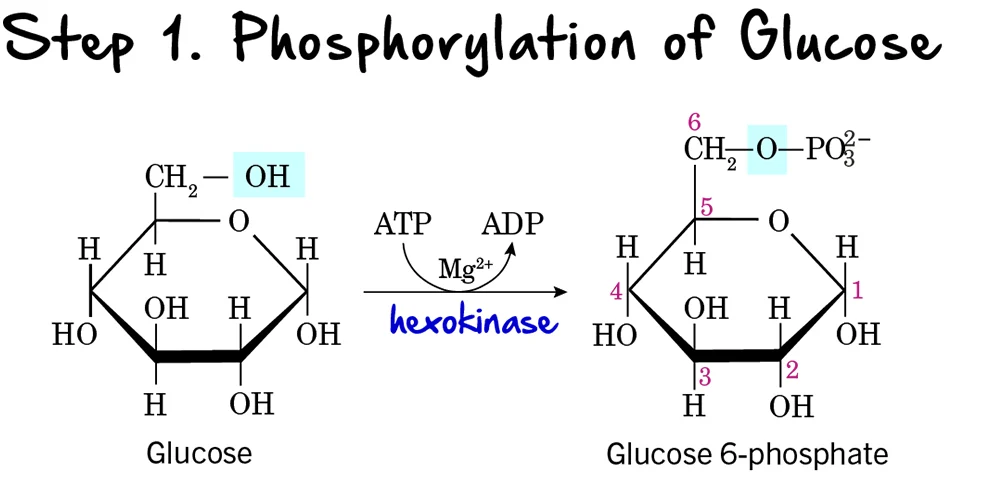
Click Here To play the Game of Glycolysis
Glycolysis: Step 1 - Phosphorylation of Glucose
The first step in glycolysis is a crucial preparatory reaction, where glucose is activated and trapped within the cell.
Reaction:
Glucose is phosphorylated on its carbon 6 (C6) hydroxyl group to form Glucose 6-phosphate (G6P). This reaction consumes one molecule of ATP.
Key Features of Step 1:
-
Enzyme: The phosphorylation is catalyzed by kinases, which are enzymes that transfer a phosphate group from ATP.
- Hexokinase: Found in most tissues. It has a high affinity for glucose, meaning it can efficiently phosphorylate glucose even at low concentrations. It is inhibited by its product, glucose-6-phosphate.
-
Glucokinase: Primarily found in the liver and pancreatic beta cells. It has a lower affinity for glucose, acting only when blood glucose levels are high. It is not inhibited by glucose-6-phosphate, allowing the liver to continue taking up glucose. Both enzymes require
Mg²⁺as a cofactor.
- Intermediate Formed: Glucose 6-phosphate
- ATP Change: -1 ATP (One ATP molecule is consumed). This is the first "investment" in the energy-investment phase.
Purpose of Phosphorylation:
- Traps Glucose in the Cell: The addition of a negatively charged phosphate group prevents glucose 6-phosphate from easily crossing the cell membrane. Once phosphorylated, glucose is effectively "locked" inside the cell.
- Activates Glucose: The phosphate group makes glucose more reactive and unstable, priming it for subsequent enzymatic reactions.
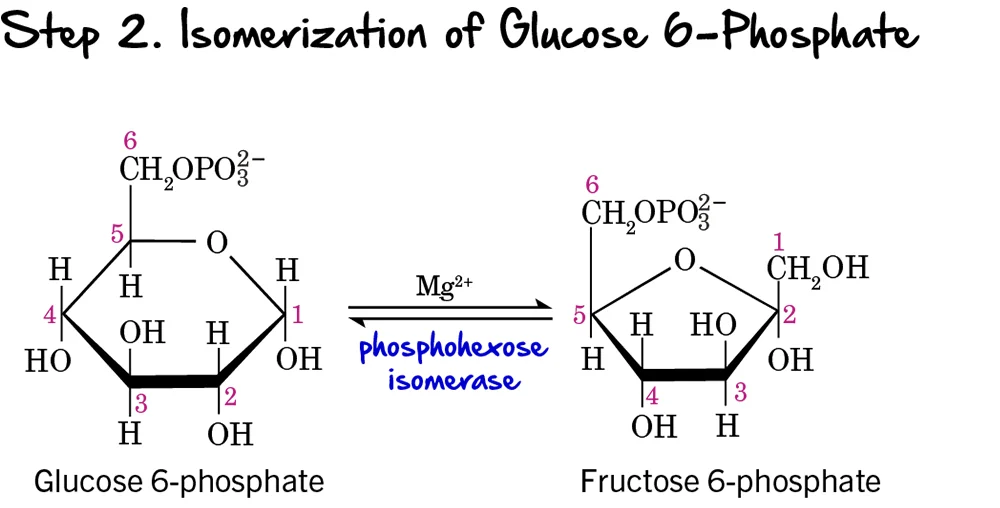
Step 2 - Isomerization of Glucose 6-Phosphate
Following the phosphorylation of glucose, the next step involves a rearrangement of the molecule from an aldose to a ketose.
Reaction:
Glucose 6-phosphate (an aldose) is isomerized (rearranged) into Fructose 6-phosphate (a ketose). This reaction is reversible.
Key Features of Step 2:
-
Enzyme: The reaction is catalyzed by Phosphohexose Isomerase (also known as Phosphoglucose Isomerase or PGI). It requires
Mg²⁺as a cofactor. - Intermediate Formed: Fructose 6-phosphate
- ATP Change: 0 ATP (No ATP is consumed or produced in this step).
Purpose of Isomerization:
This isomerization is crucial because it sets up the molecule for the next two steps in glycolysis:
- It creates a primary alcohol group at carbon 1 (C1) of fructose 6-phosphate, which can then be phosphorylated in the next step.
- It prepares the molecule for symmetric cleavage in a later step (Step 4), allowing it to be split into two 3-carbon units. If glucose 6-phosphate were cleaved directly, it would result in unequal 2-carbon and 4-carbon fragments.
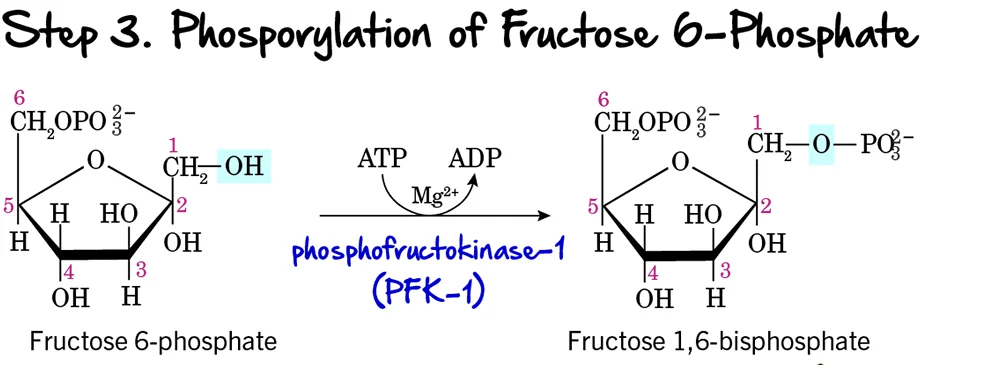
Step 3 - Phosphorylation of Fructose 6-Phosphate
This is a critical and highly regulated step in glycolysis, often considered the "committed step" of the pathway.
Reaction:
Fructose 6-phosphate undergoes a second phosphorylation, this time at its carbon 1 (C1) hydroxyl group, to form Fructose 1,6-bisphosphate. This reaction consumes another molecule of ATP.
Key Features of Step 3:
-
Enzyme: The enzyme catalyzing this reaction is Phosphofructokinase-1 (PFK-1). This is a crucial enzyme and a major regulatory point. It requires ATP as the phosphate donor and
Mg²⁺as a cofactor. - Intermediate Formed: Fructose 1,6-bisphosphate
- ATP Change: -1 ATP (Another ATP molecule is invested, bringing the total to 2 ATP).
Purpose of this Step:
- Commitment to Glycolysis: The formation of Fructose 1,6-bisphosphate is the committed step. Once formed, this molecule is generally destined to proceed through the rest of the glycolytic pathway.
- Preparation for Cleavage: Having phosphate groups on both ends (C1 and C6) is essential for the symmetrical cleavage that occurs in the next step.
Regulation of PFK-1:
PFK-1 is a key control point because its activity dictates the overall rate of glycolysis. It is allosterically regulated:
-
Activation:
- High AMP (Adenosine Monophosphate): Indicates low cellular energy, so PFK-1 is activated to increase ATP production.
- Fructose 2,6-bisphosphate: A potent allosteric activator, signaling high levels of available glucose.
-
Inhibition:
- High ATP: Indicates ample cellular energy. ATP binds to an allosteric site on PFK-1, reducing its activity.
- High Citrate: An intermediate of the Krebs Cycle, indicating that energy precursors are abundant, thus signaling to slow glycolysis.
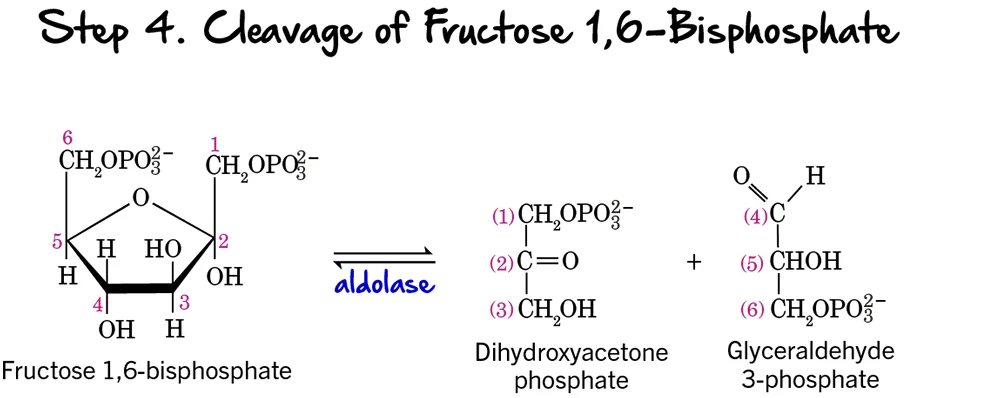
Step 4 - Cleavage of Fructose 1,6-bisphosphate
After two phosphorylation steps and an isomerization, the 6-carbon sugar is now ready to be split into two 3-carbon molecules, marking the true "lysis" of glycolysis.
Reaction:
Fructose 1,6-bisphosphate (a 6-carbon sugar) is cleaved into two distinct 3-carbon phosphorylated sugars:
- Glyceraldehyde 3-phosphate (GAP), an aldose sugar.
- Dihydroxyacetone phosphate (DHAP), a ketose sugar.
Key Features of Step 4:
- Enzyme: The enzyme catalyzing this reversible cleavage is Aldolase. The name refers to its ability to catalyze an aldol cleavage reaction.
- Intermediates Formed: Glyceraldehyde 3-phosphate (GAP) and Dihydroxyacetone phosphate (DHAP).
- ATP Change: 0 ATP (No ATP is consumed or produced).
Purpose of the Cleavage:
This step is crucial because it takes the single 6-carbon sugar and converts it into two 3-carbon molecules. These two molecules will then proceed through the second, "energy payoff" stage. The previous isomerization to fructose 6-phosphate (Step 2) was essential to enable this symmetrical cleavage into two triose phosphates, making the rest of the pathway more efficient.
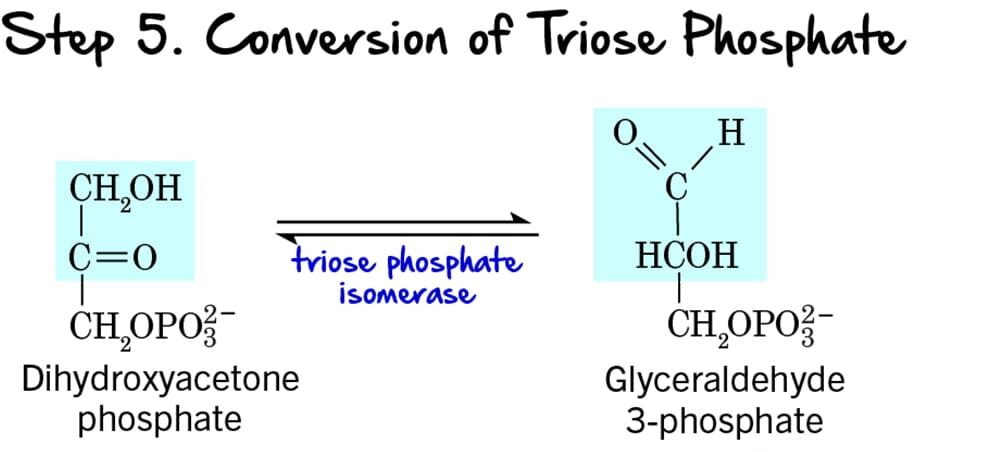
Step 5 - Interconversion of Triose Phosphates
Following the cleavage of Fructose 1,6-bisphosphate (Step 4), two different 3-carbon sugars are produced: Dihydroxyacetone phosphate (DHAP) and Glyceraldehyde 3-phosphate (GAP). However, only GAP can directly proceed into the next steps of glycolysis. This step ensures that both molecules can be utilized.
Reaction:
Dihydroxyacetone phosphate (DHAP), a ketose, is reversibly isomerized into Glyceraldehyde 3-phosphate (GAP), an aldose.
Key Features of Step 5:
- Enzyme: The enzyme catalyzing this reversible isomerization is Triose Phosphate Isomerase (TPI). This enzyme is remarkably efficient, catalyzing the reaction at a rate close to the diffusion limit.
- Intermediate Formed: Through this reaction, all the carbon atoms from the initial glucose molecule are now in the form of Glyceraldehyde 3-phosphate (GAP). From one glucose molecule, we now have two molecules of GAP ready to enter the energy payoff phase.
- ATP Change: 0 ATP (No ATP is consumed or produced).
Purpose of the Interconversion:
This isomerization is crucial because:
- Ensures Efficient Pathway Progression: Only Glyceraldehyde 3-phosphate can move forward. By converting DHAP to GAP, the cell ensures that all carbon atoms from the original glucose are processed efficiently.
- Maintains Balance: The reaction is reversible, maintaining an equilibrium between DHAP and GAP, although the subsequent rapid consumption of GAP drives the equilibrium towards GAP formation.
End of Energy Investment Phase
This concludes the Energy Investment Phase (Reactions 1-5). We have now invested 2 ATP and converted one 6-carbon glucose into two 3-carbon Glyceraldehyde 3-phosphate molecules. The pathway is now ready to enter the Energy Payoff Phase.
The Energy Payoff Phase:
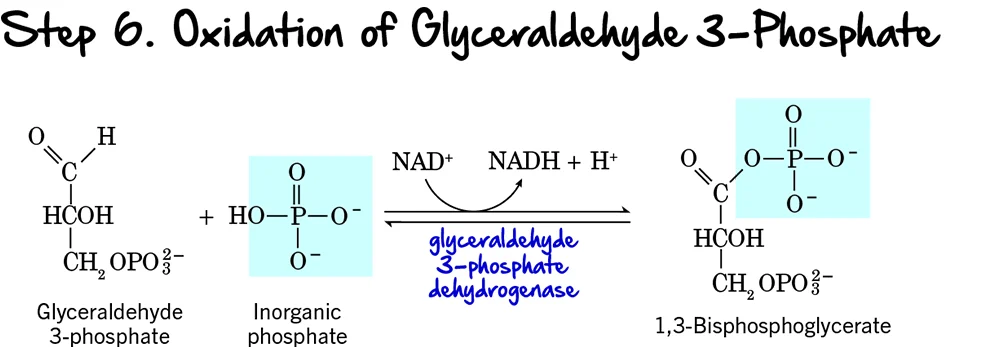
Step 6 (Oxidation and Phosphorylation of Glyceraldehyde 3-Phosphate)
We're now entering the Energy Payoff Phase of glycolysis! This is where the cell starts to recover its ATP investment and generate reducing power. Step 6 is the first reaction in this phase, and it's a crucial one as it involves both an oxidation event and the formation of a high-energy phosphate compound.
Reaction:
Each molecule of Glyceraldehyde 3-phosphate (GAP) undergoes a two-part transformation:
- Oxidation: The aldehyde group of GAP is oxidized to a carboxyl group.
- Phosphorylation: An inorganic phosphate (Pᵢ) group (not from ATP) is added to this newly formed carboxyl group, creating an acyl phosphate bond.
Key Features of Step 6:
- Enzyme: The enzyme catalyzing this reaction is Glyceraldehyde 3-phosphate Dehydrogenase.
- Intermediate Formed: 1,3-Bisphosphoglycerate (1,3-BPG).
- ATP Change: 0 ATP directly.
- NADH Production: +1 NADH is produced per molecule of GAP. Since each glucose yields two GAP molecules, this step generates a total of 2 NADH per glucose.
Purpose of this Step:
- Generation of Reducing Power (NADH): This is the only redox reaction in glycolysis. The electrons released during the oxidation of GAP are captured by NAD⁺, forming NADH. NADH is a crucial electron carrier that will later produce ATP in the electron transport chain (under aerobic conditions).
- Formation of a High-Energy Phosphate Bond: The newly formed bond at carbon 1 of 1,3-BPG is an acyl phosphate bond. This is a high-energy bond, meaning its hydrolysis releases significant free energy, which will be harnessed in the next step to synthesize ATP.
- Primer for ATP Synthesis: By creating 1,3-BPG with its high-energy phosphate, this step sets the stage for the first ATP generation in glycolysis via substrate-level phosphorylation.
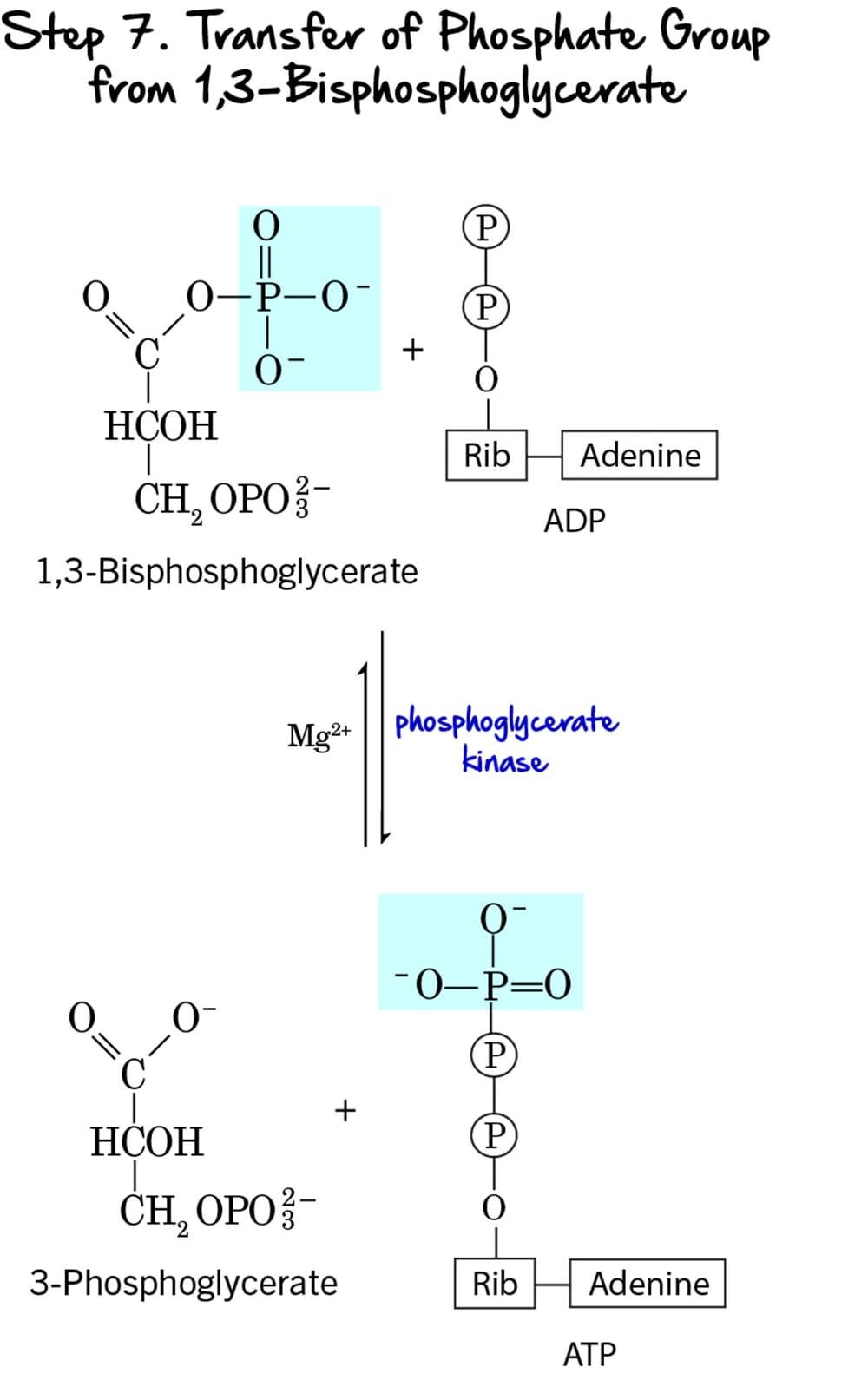
Step 7 - Substrate-Level Phosphorylation
This step marks the first direct production of ATP in glycolysis, utilizing the high-energy phosphate bond generated in the previous step.
Reaction:
The high-energy phosphate group from the C1 position of 1,3-Bisphosphoglycerate (1,3-BPG) is transferred to ADP, forming ATP. The remaining molecule is 3-Phosphoglycerate.
Key Features of Step 7:
-
Enzyme: The reaction is catalyzed by Phosphoglycerate Kinase. It requires
Mg²⁺as a cofactor. - Intermediate Formed: 3-Phosphoglycerate.
- ATP Change: +1 ATP is generated per molecule of 1,3-BPG. Since two molecules of 1,3-BPG are produced from each glucose, this step generates a total of 2 ATP per glucose.
- Mechanism: This is a classic example of substrate-level phosphorylation. ATP is formed directly from the transfer of a high-energy phosphate group from a substrate (1,3-BPG) to ADP.
Purpose of this Step:
- ATP Generation: This is the first actual ATP gain in glycolysis, partially recovering the energy invested in the preparatory phase.
- Energy Recovery: The energy released from the hydrolysis of the high-energy acyl phosphate bond in 1,3-BPG is efficiently captured to synthesize ATP.
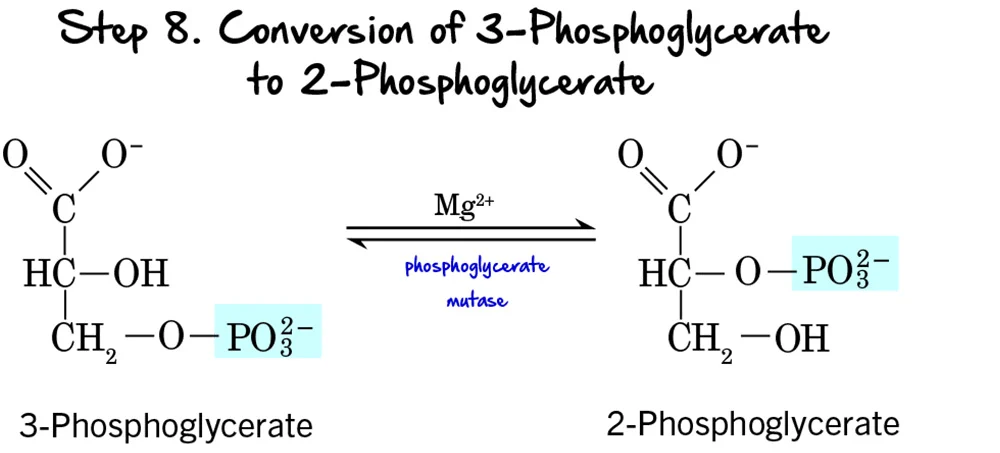
Step 8 - Migration of the Phosphate Group
After the first ATP-generating step, the molecule undergoes a structural rearrangement of its phosphate group to prepare for the next high-energy bond formation.
Reaction:
The phosphate group on 3-Phosphoglycerate moves from the carbon at position 3 to the carbon at position 2, forming 2-Phosphoglycerate. This is an intramolecular rearrangement.
Key Features of Step 8:
-
Enzyme: The reaction is catalyzed by Phosphoglycerate Mutase. Mutases are a class of isomerases that catalyze the transfer of a functional group within the same molecule. This enzyme requires
Mg²⁺as a cofactor. - Intermediate Formed: 2-Phosphoglycerate.
- ATP Change: 0 ATP (No ATP is consumed or produced).
Purpose of the Phosphate Migration:
This rearrangement is crucial for the subsequent steps:
- Positions for Dehydration: Moving the phosphate group to the C2 position places it in a strategic location to allow for the formation of a high-energy phosphate bond in the next step. It creates the necessary conditions for the dehydration reaction that follows.
- Increased Energy Potential: While 2-phosphoglycerate itself doesn't contain a high-energy bond, its structure is primed to become one through the elimination of water.
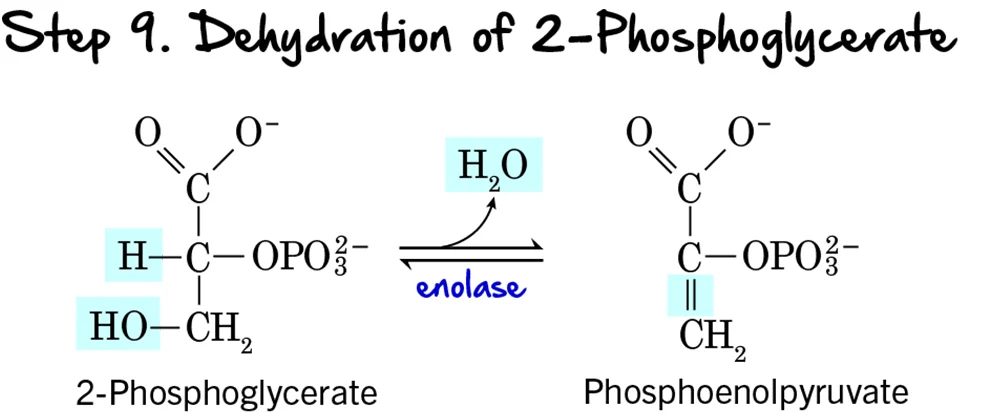
Step 9 - Dehydration of 2-Phosphoglycerate
Following the migration of the phosphate group, the molecule undergoes a dehydration reaction, which significantly raises the phosphoryl transfer potential of the phosphate group.
Reaction:
A molecule of water (H₂O) is removed from 2-Phosphoglycerate. This dehydration reaction creates a double bond within the molecule and forms the high-energy compound Phosphoenolpyruvate (PEP), which contains an "enol phosphate" bond.
Key Features of Step 9:
- Enzyme: The reaction is catalyzed by Enolase.
- Intermediate Formed: Phosphoenolpyruvate (PEP).
- ATP Change: 0 ATP (No ATP is consumed or produced).
Purpose of the Dehydration:
- Creation of a High-Energy Phosphate Bond: This is the most important outcome. The removal of water redistributes energy within the molecule, transforming a low-energy phosphate bond into a high-energy enol phosphate bond. The ΔG°' for the hydrolysis of PEP's phosphate bond is one of the highest in biochemistry.
- Preparation for ATP Synthesis: By forming PEP, the molecule is now poised to donate its phosphate group to ADP to generate ATP in the final step of glycolysis.
Clinical Relevance:
Enolase is inhibited by fluoride ions. This property is exploited in clinical settings: when blood samples are collected for glucose measurement, fluoride is often added to the collection tube to prevent glycolysis by red blood cells, ensuring the measured glucose concentration is accurate.
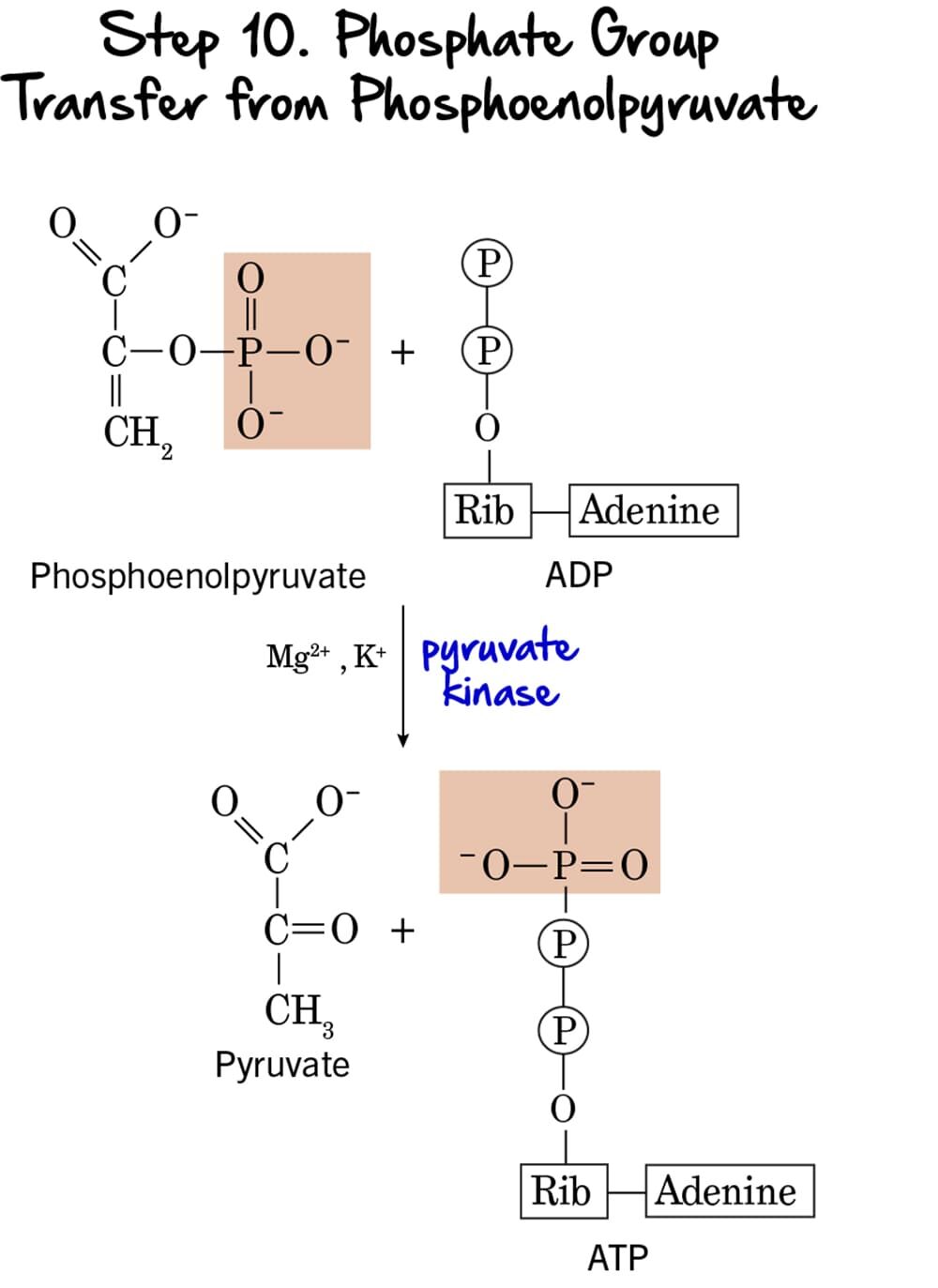
Step 10 - Phosphate Group Transfer from Phosphoenolpyruvate
This is the second and final ATP-generating step in glycolysis, again utilizing substrate-level phosphorylation to produce ATP and the ultimate end-product, pyruvate.
Reaction:
The high-energy phosphate group from Phosphoenolpyruvate (PEP) is transferred to ADP, yielding another molecule of ATP. The product remaining is Pyruvate. The initial enol form of pyruvate immediately tautomerizes to the more stable keto form.
Key Features of Step 10:
-
Enzyme: The reaction is catalyzed by Pyruvate Kinase, another key regulatory enzyme. It requires
Mg²⁺andK⁺as cofactors. - Intermediate Formed: Pyruvate.
- ATP Change: +1 ATP is generated per molecule of PEP. Since two molecules of PEP are produced from each glucose, this step generates a total of 2 ATP per glucose.
- Mechanism: This is the second instance of substrate-level phosphorylation in glycolysis.
Purpose of this Step:
- ATP Generation: This step provides the second net gain of ATP, completing the energy payoff.
- Formation of Pyruvate: Pyruvate is the end-product of glycolysis. Its fate depends on oxygen availability. Under aerobic conditions, it enters the mitochondria; under anaerobic conditions, it can be fermented.
- Irreversible Step & Regulation: This reaction is essentially irreversible, making Pyruvate Kinase a crucial regulatory enzyme.
Regulation of Pyruvate Kinase:
Pyruvate kinase is tightly regulated to control the flow of carbon through glycolysis:
-
Activation:
- Fructose 1,6-bisphosphate: This is a classic example of feed-forward activation. The product of PFK-1 (an earlier step) activates pyruvate kinase, ensuring intermediates are quickly processed.
-
Inhibition:
- High ATP: Signals abundant energy.
- Acetyl-CoA: An indicator of high energy status.
- Long-chain fatty acids: Another alternative fuel source.
Summary of Glycolysis (Net Reaction per glucose):
→
2 Pyruvate + 2 NADH + 2 H⁺ + 2 ATP
Glycolysis has now broken down one 6-carbon glucose molecule into two 3-carbon pyruvate molecules, produced a net of 2 ATP molecules, and generated 2 NADH molecules for further energy production.
Carbohydrate Metabolism and Glycolysis Read More »
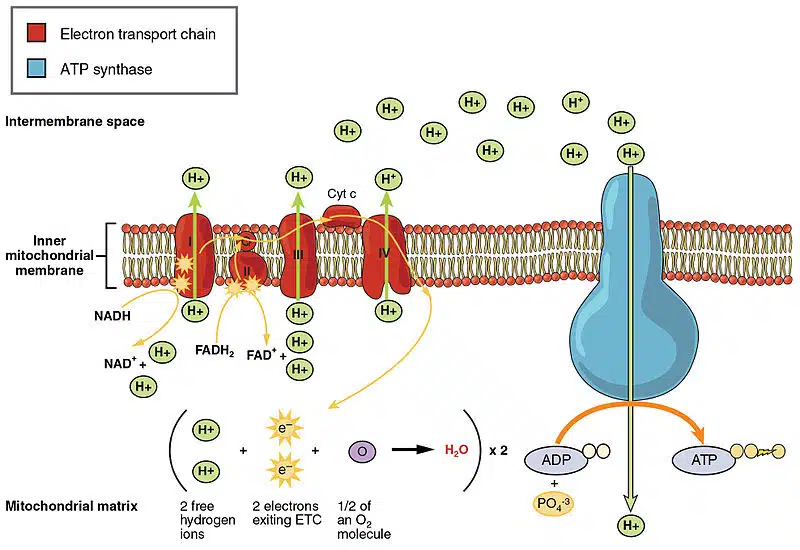
Metabolism Introduction
Metabolism
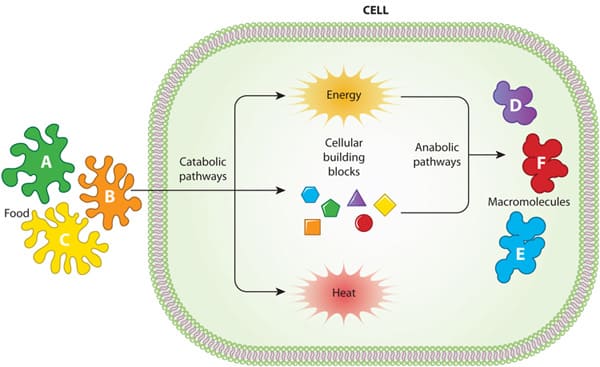
Cellular Metabolic Reactions
Metabolism refers to all the chemical reactions that occur in living organisms to maintain life. These processes allow organisms to grow, reproduce, maintain their structures, and respond to their environments. Cellular metabolism is a highly organized and interconnected network of reactions that takes place within the cell.
Types of Metabolism
There are two main types of metabolic reactions:
-
Catabolism (Breakdown): The process of breaking down complex molecules into simpler ones, usually releasing energy in the process. This energy is then captured and stored in molecules like ATP (adenosine triphosphate).
- Analogy: Demolition – taking apart a complex building to get raw materials and energy.
- Example: The breakdown of glucose into carbon dioxide and water to produce ATP.
-
Anabolism (Build-up/Synthesis): The process of building complex molecules from simpler ones, which typically requires an input of energy (often supplied by ATP).
- Analogy: Construction – using raw materials and energy to build a complex structure.
- Example: The synthesis of proteins from amino acids, or DNA from nucleotides.
These two processes are linked: the energy released during catabolism fuels anabolism, creating a continuous cycle of energy transformation and matter recycling within the cell.
Characteristics of Cellular Metabolic Reactions
- Enzyme-Catalyzed: Almost all metabolic reactions are catalyzed by specific enzymes. Enzymes allow reactions to occur quickly and efficiently at physiological temperatures and pH.
-
Highly Regulated: Metabolic pathways are tightly controlled to ensure that cells only produce what they need, when they need it. Regulation occurs at various levels:
- Enzyme activity: Allosteric regulation, feedback inhibition, covalent modification (e.g., phosphorylation).
- Enzyme synthesis: Gene expression can be turned on or off.
- Substrate availability: The presence or absence of reactants can dictate reaction rates.
-
Occur in Pathways: Metabolic reactions are rarely isolated events. Instead, they occur in a series of sequential, interconnected steps called metabolic pathways. The product of one reaction often serves as the substrate for the next.
- Linear pathways:
A → B → C → D - Branched pathways:
A → B → CandA → B → D - Cyclic pathways:
A → B → C → A(e.g., Krebs cycle)
- Linear pathways:
- Energy Transformations: A central theme of metabolism is energy transformation. Cells capture energy from their environment (from sunlight or food) and convert it into a usable form, primarily ATP.
-
Location-Specific: Many metabolic pathways are compartmentalized within specific organelles of the cell. This allows for efficient regulation and prevents conflicting reactions from occurring simultaneously.
- Cytosol: Glycolysis, pentose phosphate pathway.
- Mitochondria: Krebs cycle, oxidative phosphorylation, fatty acid oxidation.
- Endoplasmic Reticulum: Lipid synthesis, protein folding.
- Lysosomes: Degradation of macromolecules.
Biological Oxidation, the Electron Transport Chain, and Oxidative Phosphorylation
Imagine your body as a high-performance engine, and food as its fuel. Just as an engine burns fuel to produce mechanical energy, your cells "burn" food molecules to produce the chemical energy currency: ATP. This isn't a quick, explosive burn, however. It's a highly controlled process called Biological Oxidation, culminating in the Electron Transport Chain (ETC) and Oxidative Phosphorylation – the cellular equivalent of a meticulously managed power plant.
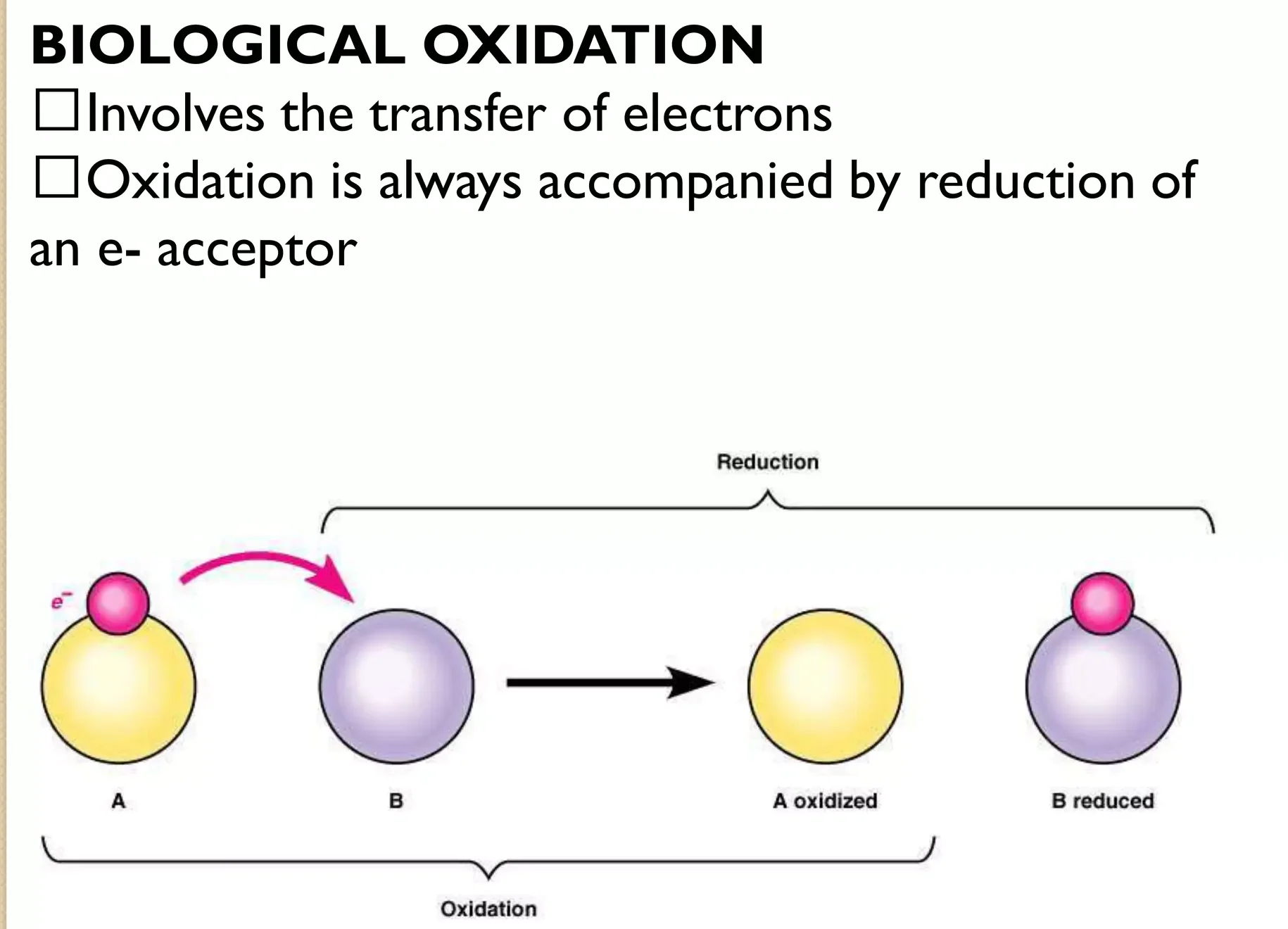
I. Biological Oxidation:
Before we get to the power plant, we need to understand the concept of "burning" food in biology. This isn't fire; it's a series of chemical reactions where molecules lose electrons.
Oxidation vs. Reduction – The Dance of Electrons:
- Oxidation: In chemistry, oxidation means a molecule loses electrons.
- Reduction: Conversely, reduction means a molecule gains electrons.
- They're Inseparable: Oxidation and reduction always happen together. If one molecule is oxidized, another must be reduced. These are called redox reactions.
- In Living Systems: Often, biological oxidation involves the removal of hydrogen atoms (a proton and an electron).
Analogy: Imagine a person (a molecule) carrying a heavy backpack (hydrogen atoms/electrons). When they "oxidize," they pass the backpack to someone else. They become lighter (oxidized), and the person who receives it becomes heavier (reduced).
The Energy Principle: Your food molecules (like glucose) are rich in electrons. By gradually removing these electrons (oxidizing the food), cells can harvest the energy stored within them.
Example: The transformation of ferrous iron (Fe²⁺) to ferric iron (Fe³⁺):
Here, Fe²⁺ is oxidized. This electron then moves on to reduce another molecule.
The Electron Shuttles: Cells use special "electron taxis" or "shuttles" like NADH (from NAD⁺) and FMNH₂ (from FMN). These molecules pick up electrons (become reduced) from the breakdown of food and deliver them to the Electron Transport Chain.
II. Overview of the Electron Transport Chain:
The ETC is where energy-rich electrons converge to generate ATP.
- Fueling the System: Carbohydrates, fats, and amino acids are first broken down.
- Making the "Electron Taxis": During this breakdown, electrons are extracted and loaded onto
NADHandFADH₂. Think of these as fully charged battery packs. - The Power Plant (ETC): These charged taxis deliver their electrons to the ETC, a series of protein complexes that act like a miniature hydroelectric dam.
- The Flow of Energy: As electrons "fall" through this chain, their energy is gradually released.
- Oxygen: The Final Acceptor: At the end of the line, the spent electrons are accepted by oxygen (O₂), combining with protons (H⁺) to form water (H₂O). This highlights why we breathe oxygen.
- ATP Generation: The energy released from this electron flow is then used to synthesize large amounts of ATP.
- Waste Products: The final "exhaust" from burning our food is carbon dioxide (CO₂) and water (H₂O).
III. Metabolic Breakdown of Energy-Yielding Molecules: Collecting the Good Stuff
How different food sources contribute to the ETC.
- Food as Raw Material: Sugar, fat, or protein are broken down through various metabolic pathways (glycolysis, Krebs cycle, beta-oxidation).
- Harvesting Electrons: The key output is not directly ATP, but rather our "energy-rich reduced coenzymes" – predominantly
NADHandFADH₂. These molecules are the direct carriers of the energy that will feed the ETC. - Heat Generation: Not all energy is captured perfectly. Some is always dissipated as heat. This "excess energy generates heat," which helps maintain our body temperature.
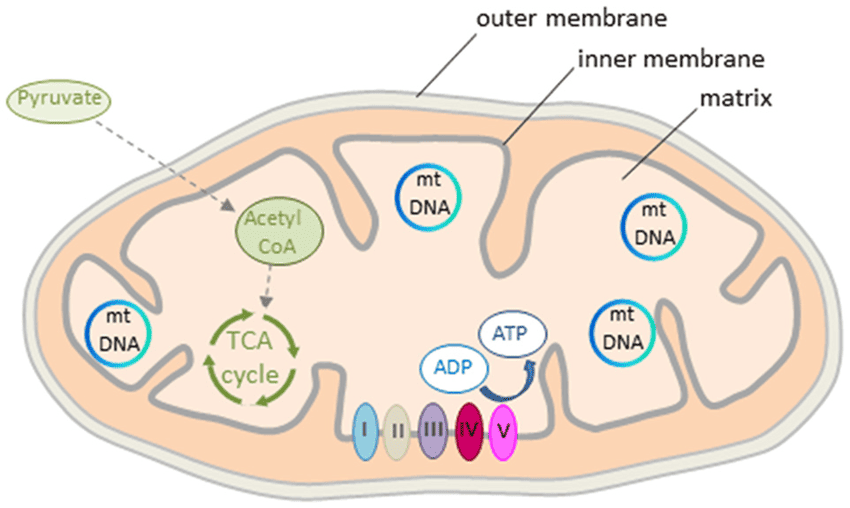
IV. The Mitochondria:
The entire process of the ETC and oxidative phosphorylation is confined to a specialized organelle: the mitochondrion.
- The "Power House" Design: Mitochondria are the "powerhouses of the cell" because they generate most of the cell's ATP.
- Mitochondrial Organization (Like a Factory Layout):
- Outer Membrane: The factory's outer wall. It's relatively porous.
- Intermembrane Space: The corridor between the outer and inner walls. This space is for building up a high concentration of protons.
- Inner Mitochondrial Membrane: The most important part for ATP production. It's highly selective and impermeable to most ions (like H⁺, K⁺, Na⁺). This impermeability is vital for maintaining the proton gradient.
- Cristae: Increasing Efficiency: The inner membrane is intricately folded into shelf-like structures called cristae.
- Analogy: Imagine building shelves in a small factory to maximize space. The cristae increase the surface area of the inner membrane, allowing more room for the ETC complexes and ATP synthase enzymes.
- Mitochondrial Matrix: The factory floor, the innermost compartment. This is a busy place, rich in enzymes that carry out:
- The citric acid cycle (Krebs cycle)
- Beta-oxidation of fatty acids
- Oxidation of amino acids
Essentially, the matrix is where much of the initial "fuel processing" happens to prepare electrons for the ETC.
V. The Electron Transport Chain (ETC):
Located entirely within the inner mitochondrial membrane.
The ETC is a precisely arranged series of protein complexes and mobile electron carriers that work together like a bucket brigade or an assembly line.
- The Goal: To take electrons from NADH and FADH₂, pass them down a chain, and use the energy released to make ATP.
- The Components (The "Workers" on the Assembly Line):
- Four Major Protein Complexes (I, II, III, IV): Large, multi-subunit proteins embedded in the inner membrane.
- Complex V (ATP Synthase): The final machine that synthesizes ATP.
- Two Mobile Carriers (Coenzyme Q and Cytochrome c): Small delivery carts ferrying electrons between the larger complexes.
- The Flow:
- Electron Acceptance: Each complex in the chain accepts electrons from the preceding component.
- Electron Donation: It then donates those electrons to the next component.
- The "Electron Affinity Gradient": The complexes are arranged in a specific order of increasing electron affinity, ensuring a downhill flow of electrons.
- Oxygen: The Ultimate Magnet: Electrons keep moving down this energy gradient until they reach the end, where they combine with oxygen (our final electron acceptor) to form water.
- Energy Harvest: The gradual release of energy as electrons move down this chain is harnessed to pump protons and ultimately make ATP.
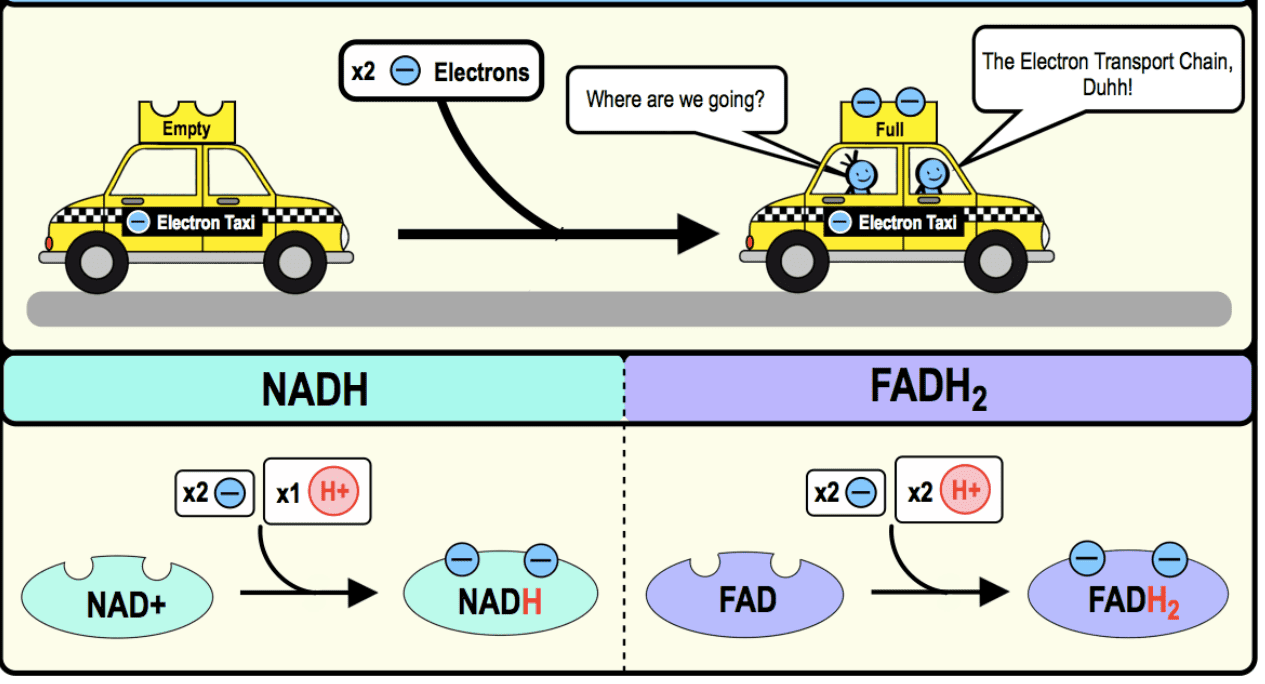
VI. The Electron Carriers: NADH, FADH₂, and More
These are the molecules that bring and pass electrons through the ETC.
-
NADH and FADH₂: The Primary Electron Taxis:
-
Nicotinamide Adenine Dinucleotide (NAD⁺/NADH):
- Derived from niacin (Vitamin B3).
- NADH is the reduced form (carrying 2 electrons) and is primarily involved in the ETC.
-
Flavin Adenine Dinucleotide (FAD/FADH₂):
- Derived from riboflavin (Vitamin B2).
- FADH₂ is the reduced form and also carries 2 electrons to the ETC.
- NADPH: Related to NADH but used for building molecules (anabolic reactions), not typically for ETC.
-
Nicotinamide Adenine Dinucleotide (NAD⁺/NADH):
-
Complex I: NADH Dehydrogenase – The First Port of Entry
- This is where NADH drops off its electrons.
- It contains the enzyme NADH dehydrogenase, a flavoprotein (contains FMN) with iron-sulfur clusters.
- The Reaction:
NADH + H⁺ + FMN → NAD⁺ + FMNH₂. Electrons are passed to Coenzyme Q (CoQ). - Crucial Action: Complex I uses the energy from these electrons to pump protons (H⁺) from the matrix into the intermembrane space.
-
Complex II: Succinate Dehydrogenase – A Unique Entry Point
- This is where FADH₂ delivers its electrons.
- It is called Succinate dehydrogenase, unique because it's both an enzyme in the Krebs cycle and a component of the ETC.
- The Reaction:
Succinate + FAD → Fumarate + FADH₂. FADH₂ is formed directly within Complex II. - Electrons are passed to Coenzyme Q (CoQ).
- Important Difference: Unlike Complex I, Complex II does NOT pump protons. This is why FADH₂ contributes less to ATP production than NADH.
-
Coenzyme Q (CoQ) / Ubiquinone – The Mobile Shuttle
- CoQ is a small, lipid-soluble molecule that acts like a ferry boat, moving within the inner mitochondrial membrane.
- It collects electrons from both Complex I and Complex II.
- It then delivers these electrons to Complex III.
-
Cytochromes – The Iron Carriers
- Cytochromes are proteins that contain an iron-containing heme group.
- The iron atom can switch between Ferric (Fe³⁺, oxidized) and Ferrous (Fe²⁺, reduced) states.
- This reversible change (
Fe³⁺ ↔ Fe²⁺) allows them to efficiently pick up and release electrons one at a time.
-
Complex III and IV: The Final Steps
- Complex III (Cytochrome bc₁ complex):
- Receives electrons from CoQ.
- Passes electrons to Cytochrome c (another mobile carrier).
- Crucially, Complex III also pumps protons.
- Complex IV (Cytochrome c oxidase):
- Receives electrons from Cytochrome c.
- This is the terminal complex. Here, electrons are finally passed to oxygen (O₂), which combines with protons to form water (H₂O).
- Crucially, Complex IV also pumps protons.
- Complex III (Cytochrome bc₁ complex):
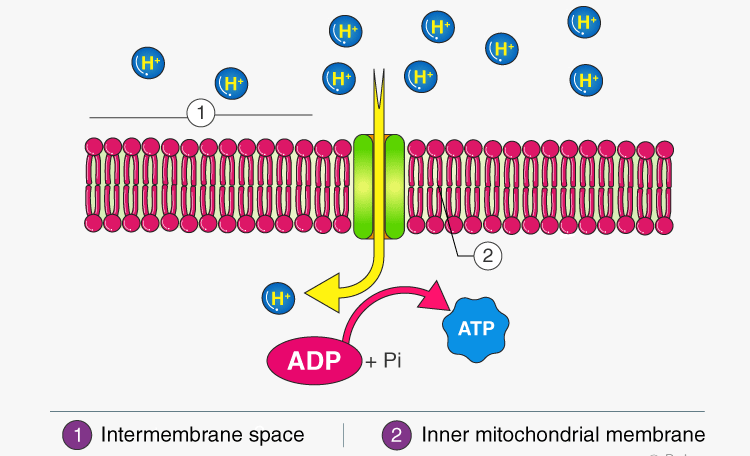
VII. Oxidative Phosphorylation: Turning the Proton Flow into ATP
The "oxidative" part (electron transport) is now coupled to the "phosphorylation" part (making ATP).
- The Link: The transport of electrons through Complexes I, III, and IV releases free energy, which is used to pump protons.
-
The Proton Gradient – A Stored Battery:
- As electrons move, Complexes I, III, and IV act as proton pumps, moving H⁺ ions from the matrix to the intermembrane space.
- Analogy: This is like using energy to pump water uphill into a reservoir. You're creating a high concentration of water (protons) on one side with potential energy. This difference in proton concentration is the electrochemical proton gradient.
- The Chemiosmotic Hypothesis: Proposed by Peter Mitchell, this explains how the proton gradient drives ATP synthesis. "Chemi" refers to the chemical gradient, and "osmotic" to movement across a membrane.
-
ATP Synthase (Complex V) – The Turbine:
- The inner membrane is impermeable to protons. The only way for protons to flow back down their gradient is through ATP synthase.
- Analogy: ATP synthase is like the turbine at the base of our dam. As the protons (water) flow back down, the turbine spins.
- ATP Synthesis: The spinning of ATP synthase uses this mechanical energy to catalyze the formation of ATP from ADP and Pi.
-
Sites of Oxidative Phosphorylation (Proton Pumping Sites):
- There are three main "power strokes" or sites where enough energy is released to pump protons:
- At Complex I, when NADH donates electrons.
- At Complex III, as electrons move from CoQ to cytochrome c.
- At Complex IV, as electrons finally reach oxygen.
The Mechanics of ATP Production:
Proton Gradients, ATP Synthase, Inhibitors, Uncouplers, and Shuttles
We've established that the Electron Transport Chain (ETC) is a sophisticated system for moving electrons and generating energy. Now, let's connect the dots to how that energy is actually converted into ATP, how the system can be sabotaged, and how electrons from outside the mitochondria get into this vital pathway.
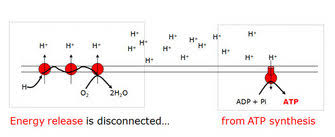
I. The Proton Gradient: The Engine's Potential Energy
Imagine a hydroelectric dam. The water held behind the dam represents potential energy. In our cellular power plant, this "potential energy" is stored in a proton gradient.
-
The Inner Mitochondrial Membrane: A Selective Barrier: The inner mitochondrial membrane is a highly specialized barrier. It's impermeable to protons (
H⁺) and hydroxyl ions (OH⁻). This impermeability is absolutely critical.
Analogy: Think of it as a perfectly sealed wall in our dam. If the wall were leaky, you couldn't build up pressure. -
Proton Pumping: Building the Pressure: As electrons move through the ETC (at Complexes I, III, and IV), energy is released. This energy is used to actively pump protons (
H⁺) from the mitochondrial matrix into the intermembrane space.
Analogy: This is like giant pumps moving water from the riverbed up into the reservoir behind the dam. -
The Result: An Electrochemical Gradient: This pumping action creates two things:
- A chemical gradient: There are now many more protons in the intermembrane space than in the matrix.
- An electrical gradient: Protons are positively charged, so the intermembrane space becomes positively charged relative to the matrix.
- The Purpose: This gradient is developed due to the electron flow in the ETC. Its sole purpose is to drive the synthesis of ATP from ADP and Pi.
II. Coupling of Electron Transport and ATP Synthesis
The core principle is how the electron flow is coupled to ATP synthesis.
- The "Coupling" Concept: Imagine two gears meshing together. One gear (electron transport) turns the other gear (ATP synthesis). They are linked. Protons (
H⁺) are pumped from the matrix into the intermembrane space, creating the proton gradient. Then, ATP synthase allows protons to flow back into the matrix, powering the enzyme to produce ATP. This is the essence of chemiosmotic coupling.
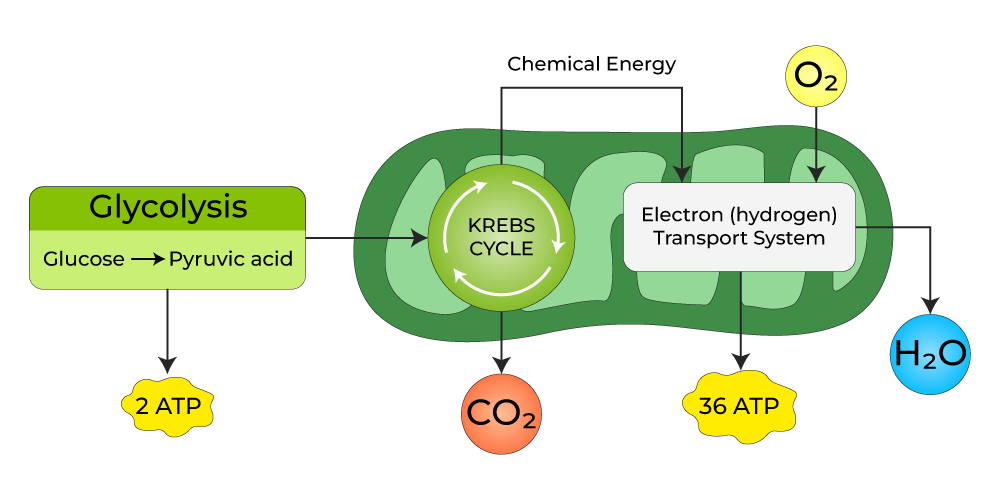
III. Outline of Chemiosmotic Hypothesis
This is the accepted model for how oxidative phosphorylation works.
- The Core Idea: Energy from the ETC (electron flow) creates a proton gradient across the inner mitochondrial membrane. The potential energy stored in this gradient is then used by ATP synthase to make ATP.
- Analogy: It's the entire hydroelectric dam in one picture. The electron "river" (ETC) powers the pumps to create the proton "reservoir" (intermembrane space), and the water flowing back through the "turbines" (ATP synthase) generates "electricity" (ATP).
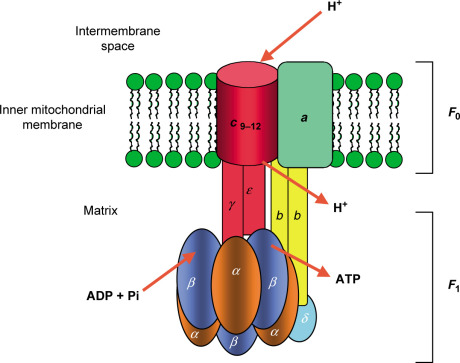
IV. Enzyme System for ATP Synthesis: ATP Synthase
The star of the show is a remarkable molecular machine called ATP synthase.
- The Master Enzyme: ATP synthase (also called Complex V) is an enzyme in the inner mitochondrial membrane that utilizes the proton gradient for the synthesis of ATP. It's also known as ATPase because it can hydrolyze ATP to ADP and Pi.
-
Structure: ATP synthase has two functional parts:
- F₀ (F-zero) component: Embedded in the membrane; it's the proton channel.
- F₁ (F-one) component: Protrudes into the matrix; this is the catalytic head where ATP is made.
- Structure of Mitochondrial ATP Synthase:
- The entire enzyme is a single F₀F₁ complex.
- The F₀ domain contains a rotating ring of 'c' subunits. A central stalk (γ subunit) is attached to this ring and extends into the F₁ head.
- The F₁ domain is the catalytic part, a sphere-like structure made of three α subunits and three β subunits. The β subunits are where ATP synthesis occurs.
- The Binding Change Model: This is the ingenious mechanism by which ATP synthase works. It's a rotating molecular motor.
- Proton Flux Drives Rotation: The flow of protons through the F₀ channel causes the 'c' subunit ring and the central γ stalk to rotate.
- Conformational Changes: This rotation causes the three β subunits in the F₁ head to change their shape sequentially. There are three conformations:
- Loose (L) conformation: Binds ADP and Pi loosely.
- Tight (T) conformation: Binds ADP and Pi tightly and catalyzes the formation of ATP.
- Open (O) conformation: Releases the newly synthesized ATP.
- The Cycle: Each β subunit cycles through L → T → O conformations. For every full rotation of the γ subunit, three ATP molecules are produced.
V. Summary of Energy Production
This integrates all the major metabolic pathways:
- Glycolysis (Cytoplasm): Breaks down glucose into pyruvate, producing a small amount of ATP and NADH.
- Krebs Cycle / Citric Acid Cycle (Mitochondrial Matrix): Further oxidizes pyruvate, producing more NADH, FADH₂, and some GTP (converted to ATP).
- Electron Transport Chain & Oxidative Phosphorylation (Inner Mitochondrial Membrane): The grand finale, where the vast majority of ATP is produced using the NADH and FADH₂ from the earlier steps.
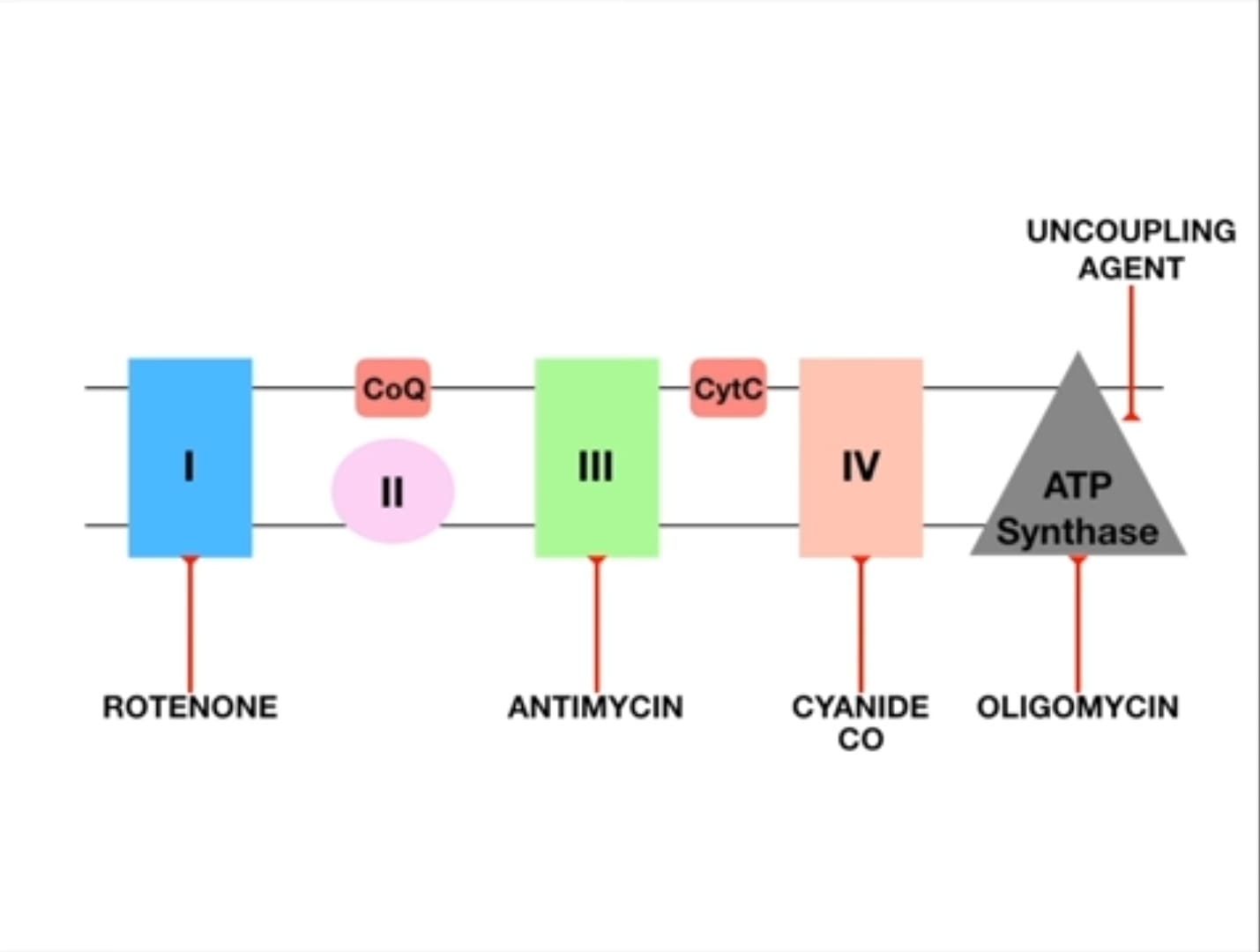
VI. Site-Specific Inhibitors of the ETC
The ETC is so critical that interfering with it can be deadly. Various compounds act as inhibitors, blocking specific points in the chain.
- Mechanism of Inhibition: Inhibitors bind to a component of the ETC, blocking electron flow.
- Upstream Accumulation: Components before the blockage accumulate electrons (become reduced).
- Downstream Oxidation: Components after the blockage become oxidized (lack electrons).
- No ATP: Blocking the ETC immediately halts ATP production.
Examples of Inhibitors:
-
Inhibitors of NADH Dehydrogenase (Complex I):
- Rotenone (pesticide), Amytal (barbiturate), Piericidin A (antibiotic).
- Effect: Blocks electron transfer from Complex I to CoQ.
-
Inhibitors of Cytochrome b-c₁ complex (Complex III):
- Antimycin A (antibiotic), BAL (British Anti-Lewisite).
- Effect: Blocks electron transfer from Complex III to cytochrome c.
-
Inhibitors of Cytochrome Oxidase (Complex IV): These are particularly dangerous.
- Carbon Monoxide (CO): Binds tightly to the Fe²⁺ in cytochrome a₃, preventing oxygen from binding.
- Cyanide (CN⁻): Binds tightly to the Fe³⁺ in cytochrome a₃.
- Azide: Also inhibits Complex IV.
- Effect: Blocks electron transfer to oxygen, effectively shutting down the entire ETC. This is why cyanide poisoning causes rapid death due to histotoxic hypoxia.
VII. Inhibitors of Oxidative Phosphorylation (Uncouplers)
Unlike inhibitors that stop electron transport, uncouplers allow electron transport to continue, but they disconnect it from ATP synthesis.
-
The Uncoupling Effect: Normally, electron transport is tightly "coupled" with ATP synthesis. Uncouplers disconnect these two processes.
Analogy: Imagine a dam where the pumps (ETC) are still moving water (protons), but the turbine (ATP synthase) is no longer connected to the generator. The water flows, but no electricity is made. -
Mechanism: Uncouplers are typically lipophilic weak acids that carry protons across the inner mitochondrial membrane, bypassing ATP synthase. They make the membrane permeable to protons.
Analogy: They poke holes in our dam wall. Protons leak back without passing through ATP synthase. -
The Result:
- Electron transport continues (often at an accelerated rate).
- No ATP is produced.
- Energy is released as heat.
Examples of Uncouplers:
- 2,4-Dinitrophenol (DNP): A notorious uncoupler once used as a weight-loss drug, leading to dangerous hyperthermia (overheating).
- Valinomycin, gramicidin, nigericin (antibiotics).
- Pentachlorophenol (PCP), FCCP, dicumarol, aspirin (at high doses).
Physiological Uncouplers:
- Some uncoupling can occur naturally in the body.
- Thermogenin (UCP1): A protein found in brown adipose tissue (BAT).
- Bilirubin: Also identified as an uncoupler.
Significance of Uncoupling:
- Heat Generation: Uncoupling is crucial for maintaining body temperature, especially in hibernating animals and newborns.
- Brown Adipose Tissue (BAT): This specialized tissue is rich in mitochondria and thermogenin. When activated, BAT uncouples oxidative phosphorylation, leading to rapid heat production without shivering.
VIII. Transport of Reducing Equivalents – Shuttle Pathways
Glycolysis happens in the cytoplasm, producing NADH. The ETC is in the mitochondria. The inner mitochondrial membrane is impermeable to NADH. So, how do these cytosolic electrons get into the ETC? Through shuttle systems!
- The Problem: NADH produced in the cytosol cannot directly cross the inner mitochondrial membrane.
- The Solution: Shuttle systems transport the "reducing equivalents" (electrons) from cytosolic NADH into the mitochondria.
Analogy: It's like having a cargo ship in a port (cytosol), but the factory (mitochondria) is inland. You need smaller trucks (shuttle systems) to deliver the goods.
1. Glycerol 3-Phosphate Shuttle:
- Mechanism:
- In the cytosol, an enzyme oxidizes NADH to NAD⁺, using the electrons to reduce dihydroxyacetone phosphate (DHAP) to glycerol 3-phosphate.
- Glycerol 3-phosphate moves to the inner mitochondrial membrane.
- Here, a different enzyme oxidizes glycerol 3-phosphate back to DHAP, transferring the electrons to FAD, forming FADH₂.
- This FADH₂ then delivers its electrons to Coenzyme Q in the ETC.
- ATP Yield: Because these electrons enter the ETC at the level of FADH₂ (bypassing Complex I), they result in the synthesis of ~2 ATPs per cytosolic NADH.
2. Malate-Aspartate Shuttle:
This shuttle is more complex but more efficient, primarily active in the heart and liver.
- Mechanism:
- In the cytosol, oxaloacetate (OAA) accepts electrons from NADH to become malate.
- Malate enters the mitochondrial matrix.
- Inside the matrix, an enzyme oxidizes malate back to OAA, regenerating NADH inside the matrix.
- This mitochondrial NADH can now directly enter Complex I of the ETC.
- (A complex cycle involving aspartate is used to return the OAA back to the cytosol).
- ATP Yield: Since the electrons are delivered to NADH within the matrix, they enter at Complex I, yielding ~3 ATPs per cytosolic NADH.
Metabolism Introduction Read More »