Mechanics of Breathing (Pulmonary Ventilation)
Mechanics of Breathing (Pulmonary Ventilation)
By the conclusion of this comprehensive master guide, you will be deeply conversant with:
- The precise pressure changes in the thoracic cavity (Intrapleural, Intrapulmonary, Transpulmonary) that drive pulmonary ventilation.
- The application of Boyle's Law to the mechanics of active inspiration and passive/active expiration.
- The diagnostic definitions and clinical significance of all Lung Volumes and Capacities (including FEV1/FVC ratios).
- The pathophysiological impact of Airway Resistance (Poiseuille's Law) and Pulmonary Compliance (Surfactant and the Law of Laplace).
- The distinction between Dead Spaces (Anatomical vs. Alveolar) and the calculation of true Alveolar Ventilation (VA).
- The neurophysiological basis of Pulmonary Reflexes (Hering-Breuer, Cough, Sneeze, J-receptors).
I. Introduction to Pulmonary Mechanics
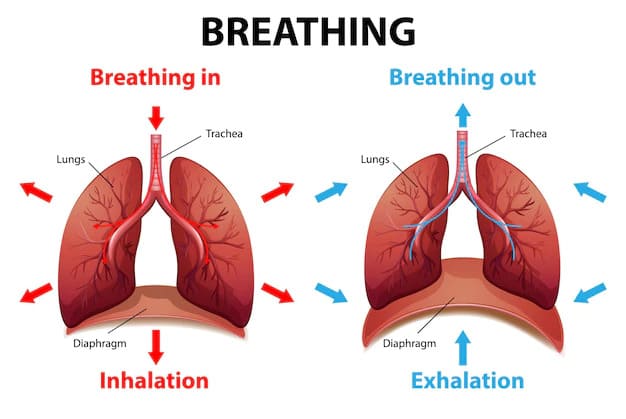
The mechanics of breathing, technically termed pulmonary ventilation, involve creating highly orchestrated pressure changes within the sealed thoracic cavity. These pressure changes act as a biological pump, moving air from the atmosphere into the lungs (inspiration) and pushing it back out (expiration). This continuous bulk flow of air is driven entirely by the contraction of skeletal muscles acting against the natural elastic recoil properties of the lung tissues.
Precisely, pulmonary ventilation is not just "sucking in air." It is a volumetric manipulation of a sealed container (the chest) that forces air to move down a pressure gradient. To master this, we must first understand the specific physiological pressures at play.
II. Objective 1: The Key Pressures of the Respiratory Cycle
To understand exactly how air is forced into and out of the lungs, it is crucial to master the various pressure gradients that drive the process. In respiratory physiology, these pressures are always described relative to each other, and most importantly, relative to the atmospheric pressure.
1. Atmospheric Pressure (Patm)
- Definition: Atmospheric pressure is the pressure exerted by the massive column of air surrounding the Earth's surface. It is the literal "weight" of the atmosphere pushing down on your body.
- Typical Value: At sea level, Patm is universally recognized as exactly 760 millimeters of mercury (mmHg) or 1 atmosphere (atm). This is also equivalent to approximately 1033 cm H2O.
- Reference Point: In clinical respiratory physiology, atmospheric pressure is set as the baseline reference point of 0 mmHg (or 0 cm H2O). This brilliant simplification allows us to discuss all other internal body pressures easily as either positive values (higher than atmosphere) or negative values (lower than atmosphere).
- Significance: Air, acting as a fluid, will always obey the laws of physics and move from an area of high pressure to an area of low pressure. Therefore, manipulating internal respiratory pressures to be above or below this baseline Patm is what drives the bulk flow of breathing. (Extra Example: If you travel to the top of Mount Everest, Patm drops drastically to around 250 mmHg, making the pressure gradient extremely weak, which is why it is incredibly difficult to ventilate your lungs effectively at high altitudes without supplemental oxygen.)
2. Intrapulmonary Pressure (Ppul) / Alveolar Pressure (Palv)
Definition: This is the precise pressure contained within the alveoli—the millions of microscopic air sacs deep within the lung parenchyma where actual gas exchange with the blood occurs. It directly represents the pressure of the air deep inside the lungs.
Characteristics and Dynamic Changes during Breathing:
- Between Breaths (End-Expiration or End-Inspiration): At the very end of a normal breath, there is a split second where airflow momentarily ceases. Because the airway is open to the outside world, Ppul perfectly equilibrates with Patm. Therefore, Ppul = 0 mmHg.
- During Inspiration: For air to flow from the outside world into the lungs, Ppul MUST become lower than Patm.
- As the thoracic cavity physically expands (due to diaphragm and intercostal muscle contraction), the lung volume increases.
- According to Boyle's Law, this massive increase in volume causes the pressure within the alveoli to drop slightly below atmospheric pressure (e.g., Ppul drops to -1 or -3 mmHg).
- This resulting negative pressure gradient (Patm > Ppul) acts as a vacuum, drawing air rushing into the lungs.
- During Expiration: For air to flow out of the lungs and back into the atmosphere, Ppul MUST become higher than Patm.
- As the thoracic cavity decreases in volume (due to the passive elastic recoil of the lungs and relaxation of muscles), the lung volume violently shrinks.
- This sudden decrease in volume compresses the trapped air, causing the pressure within the alveoli to rise slightly above atmospheric pressure (e.g., Ppul rises to +1 or +3 mmHg).
- This positive pressure gradient (Ppul > Patm) pushes the air out of the lungs.
3. Intrapleural Pressure (Pip)
Definition: This is the pressure within the pleural cavity—the microscopically narrow, serous fluid-filled potential space existing between the visceral pleura (the membrane shrink-wrapped around the lungs) and the parietal pleura (the membrane lining the inside of the ribcage/thoracic wall).
Key Characteristic: It is ALWAYS Negative
During normal breathing in a healthy human, Pip is absolutely always negative relative to both Patm and Ppul.
- At rest (between breaths), Pip is typically around -4 mmHg (-5 cm H2O).
- During active inspiration, as the chest aggressively expands outward, the pleural space is pulled wider, making the pressure even more profoundly negative (e.g., dropping to -6 to -8 mmHg).
- During expiration, as the chest collapses back inward, it becomes less negative, returning to the baseline of -4 mmHg.
Why is Pip always negative? This is a critical foundational concept. It results from a permanent "tug-of-war" between two massive opposing elastic forces:
- The Lungs' Natural Tendency to Recoil Inward: The lung parenchyma is packed with highly elastic connective tissue (elastin). It constantly wants to shrink and collapse down to the size of a fist. This creates a permanent, relentless inward-pulling force on the visceral pleura.
- The Chest Wall's Natural Tendency to Expand Outward: The structural anatomy of the ribcage (ribs, sternum, cartilage) has its own natural spring-like elasticity. If left alone, the ribcage wants to spring outward and expand. This creates a permanent outward-pulling force on the parietal pleura.
Because the lungs pull completely inward while the chest pulls completely outward, they create a permanent "suction" effect on the microscopic layer of pleural fluid between them, generating sub-atmospheric (negative) pressure. The surface tension of this pleural fluid acts like superglue between two wet panes of glass—allowing them to slide, but preventing them from being pulled apart.
Pneumothorax (Collapsed Lung)
The persistent negative intrapleural pressure is the only thing keeping the lungs inflated against their will. If a patient suffers a stab wound to the chest, or a weakened alveolar blister (bleb) ruptures inside the lung, atmospheric air rushes into the pleural cavity. The Pip instantly equalizes with Patm (going from -4 mmHg to 0 mmHg). The suction is broken. Without the negative suction holding it open, the lung instantly obeys its natural elastic recoil and collapses entirely into a tiny ball. This life-threatening condition is a Pneumothorax, and it requires a chest tube hooked to a vacuum pump to artificially recreate the negative pressure and re-inflate the lung.
4. Transpulmonary Pressure (Ptp)
Definition: Transpulmonary pressure is the exact pressure difference measured across the wall of the lung. It is the mathematical difference between the intrapulmonary pressure (Ppul) and the intrapleural pressure (Pip).
- Key Characteristic - Always Positive: Because Pip is always a negative number, subtracting a negative number yields a positive result. (Example: If Ppul is 0 mmHg and Pip is -4 mmHg, then Ptp = 0 - (-4) = +4 mmHg).
- Significance: Transpulmonary pressure represents the distending pressure across the lung wall. This is the exact force that keeps the microscopic air spaces of the lungs open. A greater transpulmonary pressure dictates a more deeply stretched and expanded lung. It is the direct physiological antagonist to the lung's inward elastic recoil.
| Phase | Patm (relative) | Ppul (relative) | Pip (relative) | Ptp (Ppul - Pip) | Airflow Direction |
|---|---|---|---|---|---|
| Start of Insp. | 0 | 0 | -4 | +4 | None |
| Mid-Inspiration | 0 | -1 to -3 | -6 to -8 | +5 to +8 | Into lungs |
| End of Insp. | 0 | 0 | -6 to -8 | +6 to +8 | None |
| Mid-Expiration | 0 | +1 to +3 | -4 to -6 | +5 to +7 | Out of lungs |
| End of Exp. | 0 | 0 | -4 | +4 | None |
III. Objective 2: Inspiration, Expiration, and Boyle's Law
Pulmonary ventilation is fundamentally a mechanical engineering process driven by changes in thoracic volume. The physical law that governs this entire relationship is Boyle's Law.
Boyle's Law
States: At a constant temperature, the pressure of a gas is inversely proportional to the volume of its container.
P ∝ 1/V
- If container Volume INCREASES, internal Pressure DECREASES.
- If container Volume DECREASES, internal Pressure INCREASES.
A. Inspiration (Inhalation)
Inspiration is ALWAYS an active process. It requires the expenditure of cellular energy (ATP) to fire motor neurons and contract skeletal muscles.
1. Muscular Contraction
Primary Muscles of Quiet Breathing:
- The Diaphragm: The supreme muscle of respiration. It is a large, dome-shaped parachute of muscle forming the floor of the thoracic cavity (innervated by the Phrenic nerve: C3, C4, C5). When it contracts, its central tendon is pulled rigidly downward. It flattens out, massively increasing the vertical (top-to-bottom) dimension of the chest.
- External Intercostal Muscles: Located between the ribs. Upon contraction, they pull the rib cage upwards and outwards. This acts like lifting a "bucket handle," drastically increasing the lateral (side-to-side) and anteroposterior (front-to-back) dimensions of the chest.
Accessory Muscles (Forced/Deep Inspiration):
When running from a lion or fighting for air, the body recruits heavy backup muscles to rip the chest open even further:
- Sternocleidomastoid: Violently elevates the sternum.
- Scalenes: Elevate the first and second ribs.
- Pectoralis Minor: Elevates ribs 3 through 5.
2. The Sequence of Events (Applying Boyle's Law)
- Thoracic Volume Increases: The muscles contract, ripping the ribcage outward and downward.
- Lung Volume Increases (via Ptp): Because the parietal pleura is glued to the visceral pleura by pleural fluid, the expanding chest wall pulls the lungs entirely open with it. The transpulmonary pressure increases, distending the lung tissue.
- Intrapulmonary Pressure Drops: The alveoli are now much larger. Following Boyle's Law, this massive volume increase causes the internal Ppul to drop to roughly -2 mmHg.
- Airflow: The Patm (0) is now heavier than Ppul (-2). A gradient is established. Air violently rushes down the trachea into the lungs until the pressure fills the space and equilibrates back to 0.
B. Expiration (Exhalation)
Unlike inspiration, normal resting expiration is a completely passive process requiring zero muscle contraction and zero energy.
1. Quiet Expiration (Passive Process)
- Muscular Relaxation: The phrenic nerve stops firing. The diaphragm and external intercostals simply relax. The diaphragm balloons back upward into its dome shape.
- Thoracic Volume Decreases: Gravity pulls the ribcage down.
- Lung Volume Decreases (Elastic Recoil): The millions of elastin fibers in the lungs, which were stretched tight like rubber bands during inspiration, now snap back to their resting size.
- Intrapulmonary Pressure Rises: The alveolar volume shrinks. Following Boyle's Law, compressing the trapped gas forces the Ppul to spike to +2 mmHg.
- Airflow Out: Ppul (+2) is now higher than Patm (0). Air is forcibly pushed out of the mouth until pressure equilibrates.
2. Forced Expiration (Active Process)
Occurs during singing, shouting, blowing out candles, exercising, or in severe lung diseases like COPD where passive recoil is destroyed.
- Internal Intercostal Muscles: Contract aggressively to rip the rib cage further downward and inward.
- Abdominal Muscles (Rectus Abdominis, Obliques): Contract powerfully. This turns the abdomen into a hydraulic press, shoving the liver and intestines violently upward into the diaphragm, forcing the diaphragm high into the thoracic cavity.
- Effect: This causes a rapid, massive compression of thoracic volume, spiking Ppul to +30 or +40 mmHg, creating a hurricane-force pressure gradient to expel air rapidly.
IV. Objective 3: Lung Volumes and Capacities
To diagnose respiratory diseases, pulmonologists measure the exact quantities of air a patient can move using a technique called spirometry. These are strictly categorized as Volumes (single measurements) and Capacities (the mathematical addition of two or more volumes).
- 1. Tidal Volume (VT or TV): The volume of air inhaled or exhaled with each normal, quiet, resting breath. Typical value is exactly 500 mL.
- 2. Inspiratory Reserve Volume (IRV): The absolute maximum volume of air that can be forcibly, desperately inhaled AFTER a normal tidal inspiration is finished. Typical value: 3000 mL. Reduced IRV indicates weak diaphragm or stiff lungs.
- 3. Expiratory Reserve Volume (ERV): The maximum volume of air that can be forcibly pushed out AFTER a normal passive tidal exhale. Typical value: 1200 mL.
- 4. Residual Volume (RV): The volume of air permanently trapped in the lungs even after blowing out as hard as physically possible. Typical value: 1200 mL.
Clinical Note: RV prevents the wet alveoli from collapsing and sticking closed between breaths. RV cannot be measured by a spirometer because you can never blow it out; it requires helium dilution tests. Massively increased RV is the hallmark of Emphysema due to chronic "air trapping."
- 1. Inspiratory Capacity (IC): (TV + IRV). The absolute total amount of air you can breathe in starting from the bottom of a normal exhale. (Approx. 3500 mL).
- 2. Functional Residual Capacity (FRC): (ERV + RV). The total air resting in your lungs during the pause between breaths. This is the crucial functional reserve where continuous gas exchange happens while you are between breaths.
- 3. Vital Capacity (VC): (TV + IRV + ERV). The absolute maximum amount of usable, exchangeable air you can manipulate. Take the deepest breath possible, then blow out every ounce of air you can. (Approx. 4800 mL).
- 4. Total Lung Capacity (TLC): (VC + RV). The absolute maximum volume the lungs can physically hold fully inflated. (Approx. 6000 mL or 6 Liters).
C. Dynamic Tests: FEV1 and the FEV1/FVC Ratio
The most important diagnostic numbers in pulmonology. These are measured by having the patient take a maximal breath and blast it out as fast and hard as humanly possible.
- FEV1 (Forced Expiratory Volume in 1 Second): The exact volume of air blasted out during the very first second of the test.
- FVC (Forced Vital Capacity): The total volume of air pushed out during the entire maximal expiration test.
- The FEV1/FVC Ratio: Healthy adults can effortlessly blow out 70% to 80% of their total lung capacity in just 1 second. (Normal ratio = 0.8).
Diagnostic Mastery: Obstructive vs. Restrictive Diseases
Obstructive Diseases (Asthma, COPD, Emphysema, Bronchitis):
The airway pipes are narrowed, filled with mucus, or collapsing. It is incredibly difficult to push air OUT. Therefore, it takes them forever to empty their lungs. FEV1 drops massively (e.g., they only blow out 1.5 L in the first second). Their total FVC also drops slightly, but FEV1 drops so severely that the FEV1/FVC Ratio plummets below 70%. Due to air getting trapped behind floppy airways, their Residual Volume (RV) and Total Lung Capacity (TLC) skyrocket (Hyperinflation / Barrel Chest).
Restrictive Diseases (Pulmonary Fibrosis, Severe Scoliosis, Asbestosis):
The airways are perfectly wide open and clear, but the lung tissue itself has turned into stiff, rigid scar tissue (or the rib cage is crushed). The lungs simply cannot inflate. They hold very little air. Their FVC is tiny (e.g., 2.0 L total capacity). However, because the pipes are wide open, they can easily blast out 90% of that tiny volume in the first second. Therefore, FEV1 and FVC drop equally, leaving the FEV1/FVC Ratio normal or beautifully HIGH (>80%). All lung volumes (TLC, RV, VC) are universally shrunken.
V. Objective 4: Factors Affecting Pulmonary Ventilation
The efficiency of air flowing into the lungs is fiercely governed by two major physical barricades: Airway Resistance and Pulmonary Compliance.
A. Airway Resistance (The Friction of Flow)
Definition: The aerodynamic drag and friction encountered by air molecules scraping against the walls of the respiratory tree.
Poiseuille's Law of Fluid Dynamics:
This law proves that resistance to flow is universally governed by the radius of the tube. Specifically, Resistance is inversely proportional to the radius raised to the 4th power (R ∝ 1/r4).
Clinical Translation: If a patient suffers an asthma attack and their airway radius shrinks by just half (1/2), the resistance to breathing doesn't double—it mathematically skyrockets by 16 times (24 = 16)! This is why asthma is so rapidly deadly. A microscopic change in airway diameter requires immense, exhausting muscular effort to overcome.
Sites of Resistance:
- Upper Airway: The nose, pharynx, and larynx naturally account for the highest baseline resistance due to turbulent flow around nasal conchae.
- Medium Bronchi: The most heavily regulated site of resistance.
- Terminal Bronchioles: Counterintuitively, resistance here is practically zero! Although each bronchiole is microscopic, there are hundreds of millions of them. Their combined, massive cross-sectional area brings resistance to near zero, allowing smooth, laminar flow into the alveoli.
Neurological Control of Airway Radius:
- Sympathetic Nervous System (Bronchodilation): During stress, the adrenal glands dump Epinephrine into the blood. It binds to Beta-2 (β2) receptors on the bronchial smooth muscle, causing profound relaxation and opening the pipes wide to maximize oxygen for running. (This is how Albuterol inhalers work).
- Parasympathetic Nervous System (Bronchoconstriction): Vagus nerve releases Acetylcholine onto Muscarinic (M3) receptors, causing the muscle to squeeze shut during rest. Inflammatory chemicals like Histamine and Leukotrienes also cause severe, pathological bronchoconstriction.
B. Pulmonary Compliance (The Stretchability)
Definition: Compliance is the exact mathematical measure of how easily the lungs stretch and distend. Formula: C = ΔV / ΔP. High compliance means the lungs inflate effortlessly like a thin plastic grocery bag. Low compliance means they are incredibly stiff and hard to inflate, like a thick rubber tire.
Factors Dictating Compliance:
- Tissue Elasticity: The balance of collagen (stiff) and elastin (stretchy). Pulmonary Fibrosis deposits massive amounts of stiff collagen scar tissue, dropping compliance drastically. Emphysema destroys elastin completely; compliance becomes pathologically high (easy to fill, impossible to empty because recoil is gone).
- Alveolar Surface Tension & Surfactant: This is the most crucial factor. The inside of an alveolus is coated with a microscopic layer of water. Water molecules are intensely attracted to each other (hydrogen bonding). This surface tension creates a violent inward force that constantly tries to crush and collapse the spherical alveolus.
The Miracle of Surfactant: To prevent the lungs from crushing themselves, specialized Type II Pneumocyte cells secrete Surfactant (a complex detergent made mostly of the phospholipid DPPC). Surfactant molecules insert themselves between the water molecules, breaking their hydrogen bonds, and vastly lowering the surface tension.
Law of Laplace (P = 2T/r): This law states that smaller spheres have a higher collapsing pressure. Therefore, smaller alveoli should theoretically collapse and empty their air into larger ones. Surfactant uniquely concentrates heavily in small alveoli, lowering their tension dramatically more than in large ones, perfectly stabilizing the entire lung architecture.
Infant Respiratory Distress Syndrome (IRDS)
Human fetuses do not begin producing adequate amounts of surfactant until roughly the 28th to 32nd week of gestation. If a baby is born highly premature, they lack surfactant. Their alveolar surface tension is catastrophic. Every time they exhale, their alveoli glue themselves completely shut. The baby must expend superhuman muscular effort to rip the alveoli open for every single breath. The infant rapidly exhausts to death. We treat this today by intubating the baby, instilling artificial bovine/porcine surfactant directly down their trachea, and placing them on CPAP machines to force the airways open.
VI. Objective 5: Dead Space and Alveolar Ventilation (VA)
Breathing 6 Liters of air into your face does not mean 6 Liters reaches your blood. To survive, air must reach the alveolar capillaries. Any air that fails to reach the blood is called Dead Space.
1. The Types of Dead Space
- Anatomical Dead Space (Vdanat): The physical volume of the conducting pipes (nose, pharynx, trachea, bronchi). No gas exchange can physically occur through the thick cartilage walls of the trachea. The volume of this space is a constant: roughly 1 mL per pound of ideal body weight (e.g., 150 lbs = 150 mL of dead space). This air is essentially wasted.
- Alveolar Dead Space (Vdalv): This is deeply pathological. These are perfectly healthy alveoli that are full of fresh oxygen, but there is absolutely no blood flowing past them to pick the oxygen up! (Example: A massive blood clot in the lung—a Pulmonary Embolism—cuts off blood flow. The alveoli are ventilated, but unperfused. This is a severe V/Q mismatch).
- Physiological Dead Space (Vdphys): The total mathematical sum of Anatomical + Alveolar dead space. In a healthy human, Alveolar dead space is zero, so Physiological Dead space perfectly equals Anatomical dead space.
The Train Analogy
Imagine the respiratory system is a massive train moving people (Oxygen).
- Tidal Volume: Every single person who boards the train.
- Anatomical Dead Space: People who sat in the engine and the baggage car; there are no doors to exit (no gas exchange).
- Alveolar Dead Space: People who successfully sat in the passenger cars, but the train stopped at a broken station with no platform (no blood flow).
- Alveolar Ventilation: The only people who actually stepped off the train at a working station and reached the city (the blood).
2. Alveolar Ventilation (VA) - The True Measure of Breathing
Definition: The exact volume of fresh atmospheric air that actually reaches the functional, perfused alveoli per minute. It represents the true life-saving efficiency of your breathing.
The Formula:
VA = (Tidal Volume - Physiological Dead Space) × Respiratory Rate
Clinical Implication: Shallow vs. Deep Breathing
If two patients both breathe a total of 6 Liters per minute, they are not equally healthy. Consider:
- Patient A (Yoga breathing): Breathes deeply (1000 mL) and slowly (6 times/min). Dead space is 150 mL.
VA = (1000 - 150) x 6 = 5100 mL/min of fresh oxygen hitting the blood. Highly efficient! - Patient B (Broken ribs / Panting): Breathes shallowly (200 mL) and rapidly (30 times/min). Dead space is 150 mL.
VA = (200 - 150) x 30 = 1500 mL/min of fresh oxygen hitting the blood. Lethally inefficient!
Because dead space is a fixed tax of 150 mL per breath, taking shallow 200 mL breaths means almost nothing but dead space air is being sloshed back and forth. This patient will rapidly suffer from Hypercapnia (toxic buildup of CO2 in the blood, leading to severe respiratory acidosis) despite breathing 30 times a minute!
VII. Objective 6: Pulmonary Reflexes and Neural Protection
The respiratory system is continuously guarded by unconscious neurological reflexes processed in the medulla oblongata to prevent mechanical destruction and chemical poisoning.
Mechanism: Mechanosensitive stretch receptors embedded deep within the visceral pleura and bronchiole smooth muscle monitor lung volume. If you take a massive, dangerously deep breath, these receptors fire. Signals rip up the Vagus Nerve (CN X) to the medulla, violently slamming the brakes on the Dorsal Respiratory Group (DRG).
Purpose: It instantly terminates inspiration to physically prevent the lungs from popping or over-inflating like a cheap balloon. It is highly active in infants regulating rhythm, but in adults, it only activates during extreme exercise or mechanical ventilation.
Mechanism: Irritant receptors heavily concentrated at the Carina (the split of the trachea) sense dust, acid, or mucous. Signals travel via the Vagus and Glossopharyngeal nerves to the medullary cough center. The body takes a deep 2.5 L breath. The vocal cords (glottis) slam tightly shut. The abdominal muscles violently contract, driving intrathoracic pressure to an insane 100+ mmHg. The glottis suddenly rips open, and air blasts out at over 100 mph.
Purpose: To act as a ballistic cannon, forcibly clearing the lower respiratory tract of lethal obstructions, aspiration, and bacterial mucus.
Mechanism: Almost identical to the cough reflex, but triggered by irritant receptors specifically in the nasal mucosa. The afferent signal travels via the Trigeminal Nerve (CN V). During the ballistic blast, the uvula and soft palate violently depress, blocking the mouth and forcing the 100 mph blast of air exclusively out through the nose.
Purpose: To clear the upper respiratory tract of foreign pollens, dust, and viral particles.
- J-Receptors (Juxtacapillary): Located in the alveolar walls right next to the blood vessels. They sense fluid backing up in the lungs (Pulmonary Edema from Left Heart Failure). When they sense drowning fluid, they trigger rapid, shallow panting (tachypnea) and the horrible feeling of shortness of breath (dyspnea).
- Proprioceptors: Located in your skeletal joints. The absolute millisecond you start running, joint movement signals the brain to increase breathing instantly, even before blood oxygen levels drop.
VIII. References
- Guyton and Hall: Textbook of Medical Physiology. (Chapters strictly focusing on Pulmonary Ventilation, Mechanics, and Circulation).
- John B. West: Respiratory Physiology: The Essentials. (The globally recognized gold standard for V/Q mismatching and dead space ventilation).
- Linda S. Costanzo: Physiology. (For integrated application of Boyle's Law, Poiseuille's Law, and Laplace's relationships).
- Bates' Guide: To Physical Examination and History Taking. (For clinical correlations of obstructive vs. restrictive spirometry findings).
Quick Quiz
Mechanism of Breathing Quiz
Physiology - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
Mechanism of Breathing Quiz
Physiology
Preparing questions...
Choose your answer and keep your streak alive.
Great effort.
Here is your quick performance summary.
Mechanics of Breathing (Pulmonary Ventilation) Read More »