
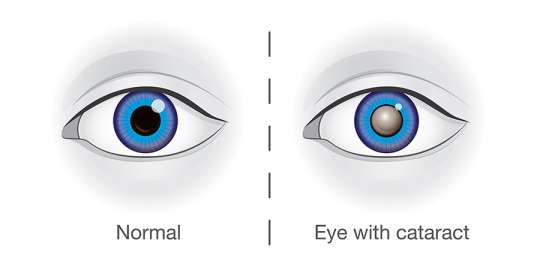

Classifications of Cataracts
Age-Related Cataract Classification
A. Morphological Classification

Nuclear Cataract: Occurs in the central nucleus of the lens, often leading to a yellowing or browning of the lens. This type can progress slowly over years. Most common.
CORTICAL CATARACT

Cortical Cataract: Occur on the outer edge/layer of the lens (cortex). Begins on the outer edge of the lens, characterized by white, wedge-shaped opacities that spread towards the center. This type often causes issues with glare.
SUBCAPSULAR CATARACT
- Occur just under the capsule of the lens.
- Starts as a small, opaque area.
- It usually forms near the back of the lens, right in the path of light on its way to the retina.
- It’s interferes with reading vision
- Reduces vision in bright light
- Causes glare or halos around lights at night.
POSTERIOR SUBCAPSULAR CATARACTS

- Posterior Subcapsular Cataracts: Begins at the back of the lens (posterior pole) and spreads to the periphery or edges of the lens. It can be developed when: Part of the eye is chronically inflamed or Heavy use of some medications (steroids).
- Affects vision more than other types of cataracts because the light converges at the back of the lens. Dilating drops are useful in this type by keeping the pupils large and thus allow more light into the eye.
IMMATURE CATARACT

- Immature Cataract: The lens is partially opaque, with some areas remaining clear. Vision is still possible but may be significantly impaired.
MATURE CATARACT
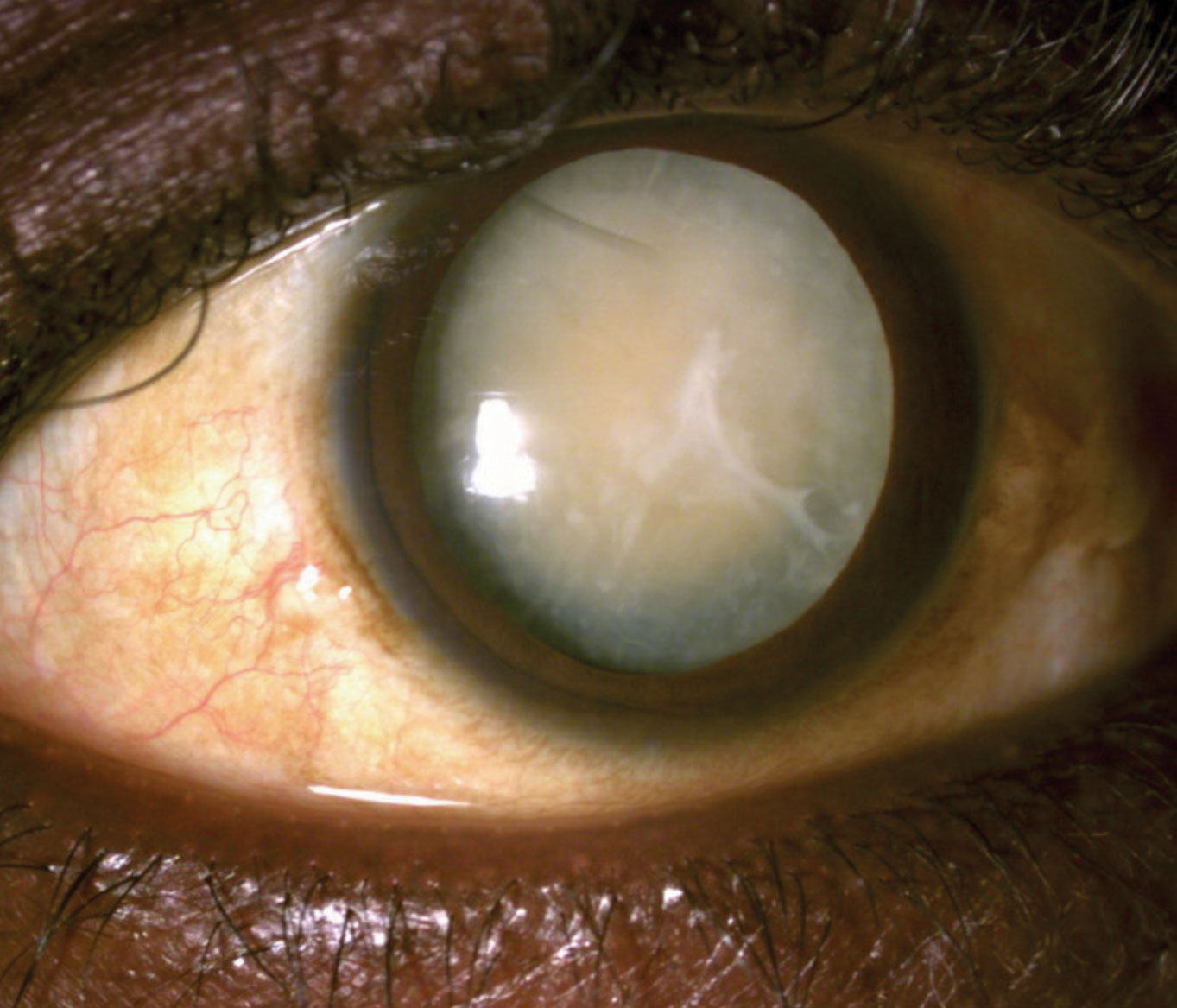
- Mature Cataract: The lens is completely opaque, leading to a significant reduction in vision. The lens may appear pearly white.
- Lens appears pearly white
- Mature cataract, with obvious white opacity at the Centre of pupil.
HYPERMATURE CATARACT ( Morgagnian)
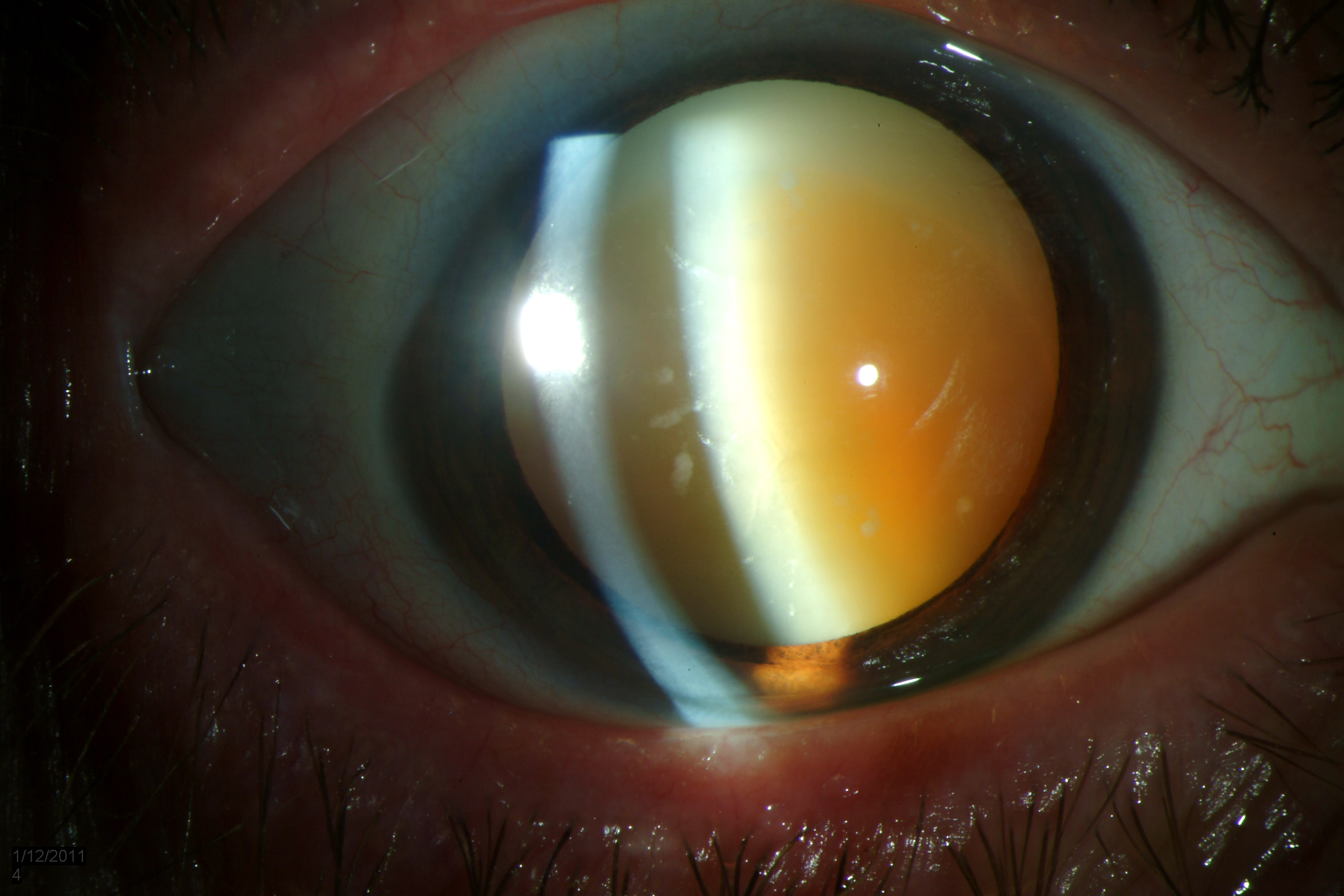
Hypermature Cataract (Morgagnian): The lens cortex becomes liquefied, and the lens nucleus may sink within the capsule. This can lead to a wrinkled anterior capsule and potentially severe complications.
- Intumescent: The proteins in the lens break down and the lens absorbs water and becomes swollen, appearing milky white.
- Liquefactive/Morgagnian Type: Cortex undergoes auto-lytic liquefaction and turns uniformly milky white. The nucleus loses support and settles to the bottom.
CONGENITAL CATARACT

Congenital Cataract Classification
- Occur in about 3:10000 live births.
- 2/3 of case are bilateral (half of the cause can be identified)
- The most common cause is genetic mutation usually.
- It can cause amblyopia(lazy eye) in infants.
It is divided to:
1. Systemic Association
- Metabolic Disorders: Conditions like galactosemia and galactokinase deficiency can cause cataracts in infants.
- Prenatal Infections: Infections like congenital rubella can lead to cataract formation in newborns.
- Chromosomal Abnormalities: Genetic syndromes such as Down syndrome, Patau syndrome, and Edward syndrome are associated with a higher risk of congenital cataracts.
2. Non-Systemic Association
- Idiopathic Cases: In some cases, the cause of congenital cataracts is unknown.
Clinical Findings / Investigations
• The most common objective finding associated with cataracts is decreased visual acuity.
• This is measured with an office wall chart or near-vision card.
- VISUAL ACUITY

Acuity refers to the sharpness of vision or how clearly you see an object.
• In this test, the doctor checks to see how well you read letters from across the room
• Eyes are tested one at a time, while the other eye is covered.
• Using the chart with progressively smaller letters from top to bottom, to determine the level of vision.
2. SLIT LAMP EXAM (SLE)
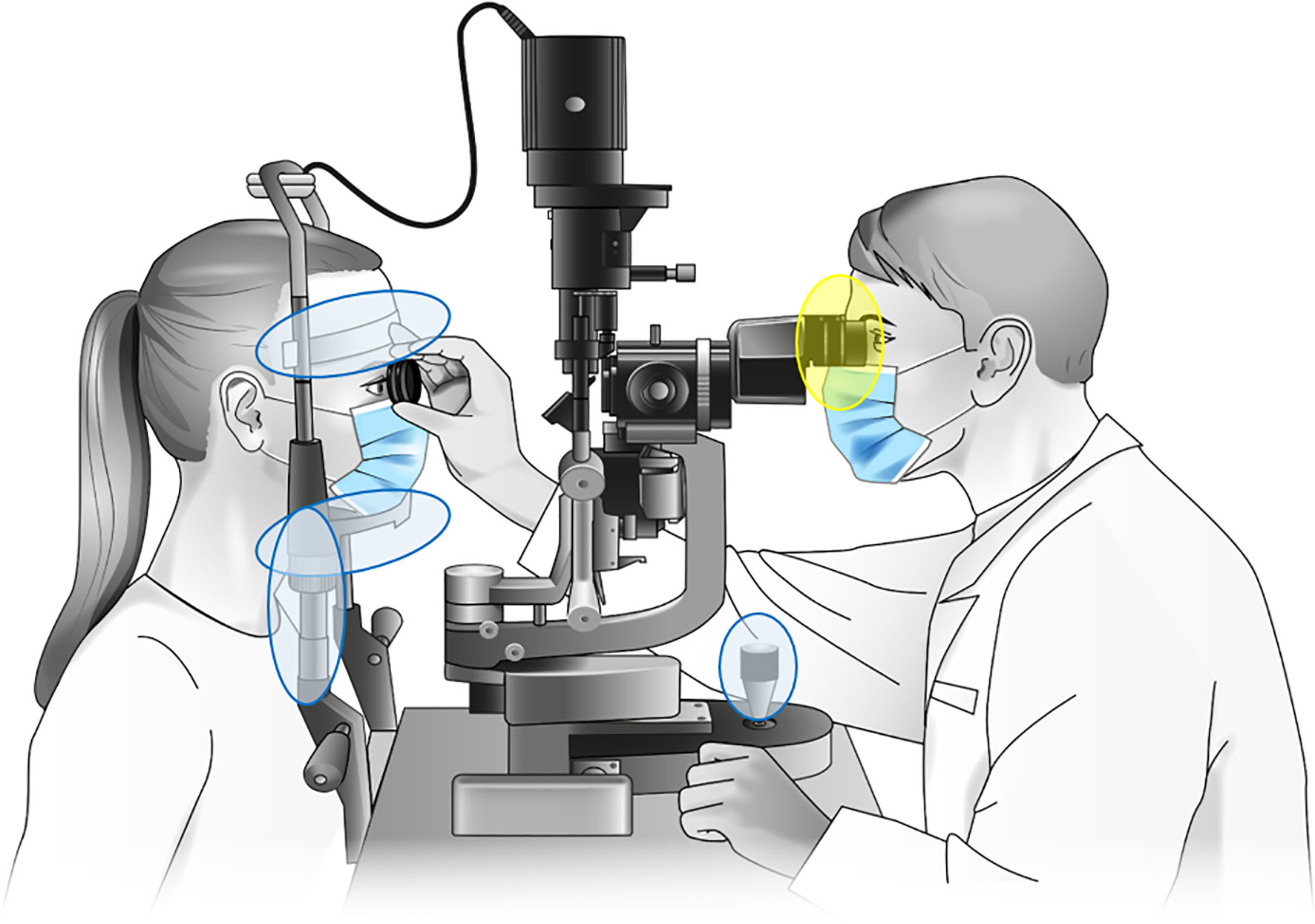
• SLE allows the ophthalmologist to see the structures of the eye under
magnification.
• The microscope is called a slit lamp because it uses an intense slit of light to illuminate your cornea, iris, and lens.
• These structures are viewed in small sections to detect any small
abnormalities.
3. DILATED EXAM

• Dilating drops are placed in the eyes to dilate the pupils wide and provide a better view to the back of the eyes.
• It allows the ophthalmologist to examine the lens for signs of a cataract and, if needed, determine how dense the clouding is.
• It also allows for examination of the retina and the optic nerve.
• Dilating drops usually keep your pupils open for a few hours before
their effect gradually wears off.
4. REFRACTION

• This is performed by your doctor to see if the decrease in vision is simply
due for need for new glasses, or if there is another process at work that accounts for the decrease in visual acuity.
Treatment/Management of Cataracts
1. Non-Surgical Management.
- Glasses: Cataracts alter the refractive power of the natural lens, so glasses can help maintain good vision.
- Make sure that eyeglasses or contact lenses are the most accurate prescription possible.
- Patient Advice:
- Lighting: Improve home lighting with more or brighter lamps.
- Sunglasses: Wear sunglasses outdoors to reduce glare.
- Night Driving: Limit night driving.
2. Surgical Management.
Indications:
- Changes in eyeglasses no longer improve vision.
- Quality of life is significantly impacted.
- Cataract removal is likely to improve vision (when visual acuity cannot be improved with glasses).
Surgical Techniques:
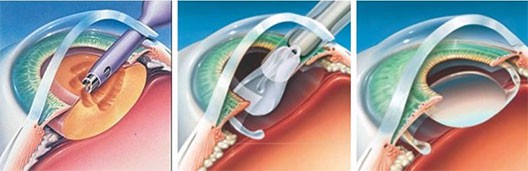
Phacoemulsification:
- Procedure: A tiny, hollowed tip uses high-frequency (ultrasonic) vibrations to break up the cloudy lens (cataract). The same tip is used to suction out the lens.
- Advantages: Minimally invasive, precise, and generally results in faster recovery.
Extracapsular Cataract Extraction (ECCE):
- Procedure: The nucleus and cortex are removed from the capsule, leaving behind the intact posterior capsule, peripheral anterior capsule, and zonules.
- Advantages: Preserves the capsular bag, reducing the risk of complications like vitreous prolapse.
Intracapsular Cataract Extraction:
- Procedure: The entire lens (nucleus, cortex, and capsule) is removed as a single piece after breaking the zonules.
- Advantages: Eliminates the risk of posterior capsular opacification (after-cataract).
- Disadvantages: Increased risk of complications like vitreous prolapse and retinal detachment.
3. Pre-Operative Assessment:
- General Health Evaluation:
Blood pressure check.
Assessment of patient’s ability to cooperate with the procedure and lie flat during surgery.
Eye Drop Instillation Instruction: Teach patients how to instill eye drops correctly.
Reassurance and Consenting: Provide reassurance and obtain informed consent.
Intraocular Pressure: Ensure normal intraocular pressure or adequate control of pre-existing glaucoma.
4. Post-Operative Care:
- Discharge: Patients are usually discharged home the same day.
Follow-Up: Patients are seen in the office the next day, the following week, and then again after a month to monitor healing progress.
Patient Advice:
Discomfort: Mild discomfort is normal for a couple of days after surgery.
Eye Patch/Shield: Wear an eye patch or protective shield the day of surgery.
Exertion: Avoid strenuous exertion to prevent increased pressure in the eyeball.
Trauma: Avoid ocular trauma.
Medications: The doctor may prescribe medications to prevent infection and control eye pressure:
Steroid drops: To reduce inflammation.
Antibiotic drops: To prevent infection.
Complications of Cataract Surgery
- Infective Endophthalmitis: A rare but severe infection that can lead to vision loss.
- Suprachoroidal Hemorrhage: Severe intraoperative bleeding that can cause permanent vision loss.
- Uveitis: Inflammation of the uvea, more common in patients with diabetes or a history of ocular inflammation.
- Ocular Perforation: A rare but serious complication.
- Refractive Error: Incorrect intraocular lens power can lead to residual vision problems.
- Posterior Capsular Rupture and Vitreous Loss: Can increase the risk of retinal detachment.
Very intrestive
Permite use of offline
Thx alot for the good work
It was concise and precised notes
Congratulations 👏👏
thsnks so much sir