

Palliative care emergencies refer to any sudden change in a patient's condition that necessitates immediate and urgent intervention.
These are not the dramatic emergencies of a trauma ward (like a car accident), but they are equally serious in their impact on a dying patient's comfort and dignity.
In palliative care, an emergency is defined by what the patient and family experience, not just by medical severity.
A sudden increase in pain, a terrifying bleed, or a patient who suddenly cannot move their legs, these are emergencies because they cause sudden suffering, fear, and potential rapid deterioration of quality of life.
| Feature | General Emergency | Palliative Care Emergency |
|---|---|---|
| Goal | Save life, cure disease | Relieve suffering, maintain dignity, respect wishes |
| Timeframe | Act immediately to prevent death | Act promptly to prevent suffering |
| Patient condition | Usually stable enough for aggressive treatment | Often frail, near end of life (cachectic, immunosuppressed) |
| Treatment options | All available | Limited by prognosis, patient wishes, resources |
| Outcome hoped for | Recovery | Comfort, peace, quality of life |
| Family involvement | Often excluded during crisis | Central to decision-making |
In palliative care emergencies, we do not always aim to "save life" — we aim to save quality of life, to prevent unnecessary suffering, and to honor the patient's wishes. Aggressive interventions that prolong the dying process without adding comfort are considered medically inappropriate.
Before acting, the nurse and team must pause and think. Every emergency in palliative care requires careful consideration of multiple factors:
- What exactly is happening? Is it pain, bleeding, paralysis, confusion?
- How sudden is it? Did it develop over hours or minutes?
- Is it truly new, or an escalation of an existing problem?
Why this matters: A sudden collapse from a pulmonary embolism needs different thinking than a gradual increase in pain. The nurse must identify the problem accurately before treating.
- How strong is the patient? Are they alert, weak, bedridden, or unconscious?
- What other symptoms do they have? Are they already struggling with breathlessness, nausea, or confusion?
- Can they swallow? This determines whether oral medicines are possible.
Why this matters: A frail, cachexic patient with advanced cancer cannot tolerate aggressive interventions the way a stronger patient might. The nurse must match the intervention to the patient's capacity.
- How far has the disease progressed? Is the patient expected to live days, weeks, or months?
- Is this emergency likely to be the "final event"? For example, a massive hemorrhage in a patient with advanced head and neck cancer (carotid blowout) may be the terminal event.
- What has the patient already been through? Multiple hospital admissions, failed treatments, exhaustion?
Why this matters: If a patient is in their final days, subjecting them to a traumatic transfer to hospital, invasive tests, or painful procedures may cause more harm than good. The nurse must ask: "Will this help them live better, or just prolong dying?"
- What treatments exist for this emergency? Radiotherapy for spinal cord compression? Surgery for a blocked bowel? Blood transfusion for severe anemia?
- Are these treatments available in this setting? In rural Uganda, a CT scan, an MRI, or an operating theater may be hours or days away.
- Can the patient reach the treatment? Transport costs, road conditions, family capacity to travel.
Why this matters: In Uganda, availability is often the deciding factor. The nurse must know what is realistically possible and not promise what cannot be delivered.
- How much will treatment cost? Surgery, radiotherapy, blood transfusions, and some medicines are expensive.
- Can the family afford it? In Uganda, many families sell land, borrow money, or go without food to pay for treatment.
- Is the cost justified by the benefit? Will expensive treatment add days of suffering or days of quality life?
Why this matters: Palliative care in Uganda must be affordable and appropriate. The nurse must advocate for treatments that are effective and accessible, and help families make informed decisions without guilt.
- Will the treatment work? What is the chance of success?
- What are the side effects? Will the treatment cause more nausea, pain, confusion, or weakness?
- Is the burden worth the benefit? For example, emergency radiotherapy for spinal cord compression may prevent paralysis but cause severe fatigue.
Why this matters: In palliative care, "first, do no harm" is paramount. A treatment that causes more suffering than relief is not appropriate.
- What has the patient said they want? Have they expressed a wish to die at home? To avoid hospitals? To "not be a burden"?
- Have they made an advance directive or living will? (Rare in Uganda, but increasingly important).
- Are they able to express wishes now? If confused or unconscious, what did they say before?
Why this matters: The patient's autonomy (right to make decisions about their own body and life) is central to palliative care. Even in an emergency, we must respect their wishes unless they are unconscious and we must act in their best interest.
- What does the family want? Do they want everything possible done? Or do they want the patient to be comfortable at home?
- Is there family conflict? Different family members may disagree about treatment.
- What are the cultural expectations? In some Ugandan cultures, "doing everything" is seen as love; in others, allowing natural death is respected.
Why this matters: Families in Uganda are often the primary caregivers and decision-makers. The nurse must listen to them, educate them, and help them reach consensus. However, the patient's wishes come first if they are known.
When a palliative care emergency occurs, the nurse must assess systematically and quickly:
Establish an accurate diagnosis. What is actually happening? Do not assume. A patient who suddenly cannot walk may have spinal cord compression, a stroke, severe weakness from anemia, or a fractured bone. Ask questions, examine, review the history.
Can this problem be reversed? Or is it part of the natural progression toward death? Example: A blocked bowel from tumor may be reversed with surgery in some cases, but not in others. Example: Severe pain from a pathological fracture can be relieved with morphine and radiotherapy, but the fracture itself may not heal. Why this matters: If irreversible, the focus shifts entirely to comfort.
How will resolving (or not resolving) this problem affect the patient? Will treating it improve their quality of life for days or weeks? Will leaving it untreated cause unbearable suffering? Will aggressive treatment cause more suffering than the problem itself?
Will active intervention enhance the patient's quality of life? This is the central question in palliative care emergencies. A blood transfusion may give a patient energy to say goodbye to their children. Emergency surgery may give a patient weeks of comfortable life at home. But intensive care admission may only prolong dying in a patient who wishes to die at home.
Can we actually do what we are considering? Is the treatment available in this hospital, this district, this country? Can the family pay? If not, are there alternatives?
What does the patient want? (If able to express). What does the family want? Is there consensus? If not, the nurse may need to facilitate discussion.
There are circumstances in the care of patients with life-limiting conditions that require urgent assessment and treatment. Although not a daily occurrence, rapid intervention can prevent more serious consequences. While it is important to focus on the common medical emergencies, it is important to remember that emergencies in palliative care include a wider range of issues:
- Hypercalcaemia: (High calcium in the blood). Expansion: Tumors (especially breast, lung, multiple myeloma) release Parathyroid Hormone-related Protein (PTHrP), which forces osteoclasts to destroy bone, dumping massive amounts of calcium into the blood. Symptoms: "Stones, bones, groans, and psychiatric overtones" (confusion, severe constipation, thirst).
- Spinal cord compression: Expansion: Tumor metastasizes to the vertebral body, expands, and collapses the bone backward into the spinal canal, crushing the spinal cord. It causes sudden back pain followed by paralysis and loss of bowel/bladder control. Irreversible if not treated with high-dose steroids (Dexamethasone) within 24-48 hours.
- Superior Vena Cava Obstruction (SVCO): Expansion: A lung tumor or lymphoma physically pinches the main vein returning blood from the head to the heart. Blood backs up, causing massive swelling of the face/neck, prominent chest veins, and severe breathlessness.
- Massive haemorrhage: (Severe bleeding, e.g., a tumor eroding into a major artery).
- Severe uncontrolled pain
- Pathological fractures: Bones hollowed out by cancer breaking under normal weight.
- Acute bowel obstruction: Tumors physically blocking the intestines.
- Sepsis and infections: Common due to neutropenia (low white blood cells) from chemotherapy.
These are equally important and often overlooked:
| Emergency Type | Description | Example |
|---|---|---|
| Emergency discharge | A patient wants to go home to die immediately. | "I want to die in my village. Please help me leave today." |
| Emotional emergencies | High levels of expressed anxiety, panic, or despair. | A patient screaming, "I cannot bear this anymore!" |
| Spiritual/existential emergencies | Pressure to "sort things out" before death. | A patient who needs to reconcile with an estranged child urgently. |
| Social emergencies | Sudden family crisis, eviction, or loss of caregiver. | A caregiver dies suddenly, leaving the patient alone. |
Why these matter: A patient who is terrified, who has unfinished business, or who is about to be evicted is in a true emergency — their suffering is as real as physical pain. The nurse must recognize and respond. This relates to Dame Cicely Saunders' concept of "Total Pain".
- Are they early in the illness (months to live, still relatively strong)?
- Are they mid-course (weeks to months, declining but still active)?
- Are they near the end (days to weeks, very weak, bedbound)?
- Are they actively dying (hours to days)?
Why this matters: The answer determines what is appropriate. A patient early in their illness may benefit from aggressive intervention for spinal cord compression. A patient in their final hours needs comfort, not a hospital transfer.
- Is this a new problem (e.g., a new fracture, a new infection)?
- Is this a progression of the disease (e.g., tumor growing, nerves being compressed)?
- Is this a treatment side effect (e.g., chemotherapy causing severe mucositis)?
- Is this a complication of immobility (e.g., pressure sore, DVT)?
- Is this psychological/spiritual (e.g., panic attack manifesting as chest pain)?
Why this matters: The cause determines the treatment. A panic attack needs reassurance and anxiolytics, not morphine. A pathological fracture needs immobilization and radiotherapy, not just painkillers.
- Ideas: What do they think is happening? (They may think a headache means "the cancer has gone to the brain" when it is actually tension).
- Concerns: What are they most afraid of? (They may fear paralysis more than death).
- Expectations: What do they hope will happen? (They may expect a cure, or comfort).
Why this matters: If they expect a cure when cure is impossible, they will be devastated. Align expectations with reality gently.
As a nurse, you are often the first to recognize an emergency and the first to respond.
| Role | Action |
|---|---|
| Early recognition | Know the signs of common emergencies. Monitor patients closely. |
| Rapid assessment | Use the assessment framework above. Ask the three critical questions. |
| Immediate comfort measures | Give pain relief, reassurance, position the patient, call for help. |
| Communication | Explain to the patient and family what is happening and what you are doing. |
| Coordination | Contact the doctor, arrange transport if needed, mobilize family support. |
| Documentation | Record the emergency, actions taken, and patient/family response. |
| Advocacy | Speak for the patient's wishes. Prevent unnecessary suffering from futile treatment. |
| Emotional support | Stay calm. Your calmness reassures the patient and family. |
| Follow-up | After the crisis, review what happened. Support the patient and family in processing. |
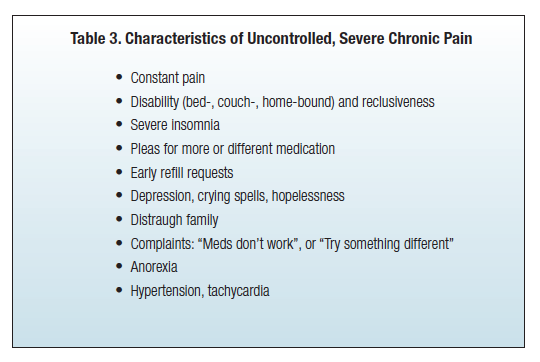
Severe uncontrolled pain is a palliative care emergency because it causes immediate and intense suffering that overwhelms the patient and family. It demands urgent, constant attention until the pain is brought under control. Pain is not "just a symptom" in this context — it is a crisis that:
- Prevents the patient from thinking, sleeping, eating, or communicating.
- Causes terror and despair in the patient and family.
- May lead to suicidal thoughts or requests for euthanasia.
- Indicates a serious underlying problem (fracture, obstruction, nerve compression) that may need specific treatment.
| Type | Description | Example |
|---|---|---|
| Anticipatory pain | Pain expected before a procedure or event | Fear of the pain of a wound dressing |
| Procedural pain | Pain caused by a medical procedure | Pain during insertion of a urinary catheter |
| Acute-on-chronic pain | Sudden severe pain in a patient with existing chronic pain | A patient with stable cancer pain who suddenly develops a pathological fracture |
| Breakthrough pain | Transitory flare of pain "breaking through" regular analgesia | A patient on regular morphine who suddenly screams with severe back pain |
Important: Acute pain that is left uncontrolled can evolve into chronic pain (present for >3 months). Physiologically, continuous severe pain signals bombard the spinal cord, activating NMDA receptors. The nervous system undergoes a "wind-up" phenomenon, becoming chemically "sensitized" — it learns to feel pain even when the original cause is gone, and normal touches begin to feel painful (Allodynia). Preventing this permanent nervous system rewiring is exactly why we treat acute pain as an absolute emergency.
| Source | Description | Example |
|---|---|---|
| Bone metastases | Cancer spread to bones (activates osteoclasts to dissolve bone) | Severe back pain from collapsed vertebrae |
| Visceral cancer | Tumors in internal organs causing pressure/stretching | Liver capsule pain from enlarged liver; bowel obstruction |
| Thoracic cancer | Cancers in the chest (lung, esophagus, pleura) | Chest wall pain from rib invasion; pleuritic pain |
| Soft tissue/bone cancer | Primary or secondary tumors in muscles, skin, or bones | Pain from a fungating breast tumor; pain from a sarcoma |
| Nervous system | Tumors or infections affecting nerves or spinal cord | Sciatica from nerve compression; burning HIV neuropathy |
| Procedure/treatment | Pain caused by surgery, radiotherapy, chemotherapy | Mucositis from chemotherapy; radiation burns; post-surgical |
| Cancer complications | Infections, bleeding, or other complications | Severe pain from infected wound; pain from abscess |
In an emergency, there is no time for a leisurely assessment. The nurse must rapidly identify the underlying cause to give the most appropriate treatment. Ask yourself: Is this a new pain or an escalation? Is there a clear trigger? Are there signs of a specific cause?
| Possible Cause | Clues on Assessment |
|---|---|
| Pathological fracture | Sudden severe bone pain after minor movement; deformity; inability to bear weight |
| Spinal cord compression | Back pain with weakness, numbness, or paralysis in legs; loss of bladder/bowel control |
| Bowel obstruction | Colicky abdominal pain, vomiting, constipation, distended abdomen |
| Infection | Fever, localized tenderness, redness, pus |
| Bleeding into tumor | Sudden increase in pain with swelling, bruising, or signs of blood loss |
| Nerve compression | Shooting, burning pain with numbness or weakness in a specific area |
- P — Position/Precipitating: "Where is the pain? What makes it worse? Did anything trigger it?"
- Q — Quality: "What does it feel like? (Burning = nerve; crushing = bone; cramping = bowel)"
- R — Radiation: "Does it spread anywhere? (To the leg = sciatica; to the shoulder = diaphragm irritation)"
- S — Severity & Site: "How bad is it? 0-10? Point to where it hurts."
- T — Timing & Treatment: "When did it start? What have you taken? Did it help?"
- Numerical Rating Scale (NRS): Adults who can count ("Rate your pain 0-10").
- Visual Analogue Scale (VAS): A 10cm line; patient marks their pain level.
- Faces Scale (Wong-Baker): Children under 8, or low literacy. Six faces from smiling to crying.
- Hand Scale: African settings. Clenched fist = 0; 5 extended fingers = worst pain.
Important: Assess pain at rest AND during movement. Incident pain needs pre-emptive analgesia before moving.
- General appearance: Distress, sweating, pallor, guarding (Indicates sympathetic NS activity).
- Vital signs: Tachycardia and hypertension suggest severe pain; fever suggests infection.
- Site of pain: Inspect for swelling, redness, deformity, wounds.
- Neurological: Check sensation, strength, reflexes (numbness = nerve/spinal cord involvement).
- Abdomen: Distension, tenderness, bowel sounds (obstruction or peritonitis).
- Mobility: Can the patient move/bear weight? (Immobility suggests fracture or spinal compression).
"To reduce the pain and allow the patient to rest. The patient will settle enough to facilitate further assessment." The first priority is not to find the exact cause — it is to relieve the suffering. Once the patient is comfortable, a more thorough assessment can follow.
- Act immediately — do not wait for the doctor to arrive if you have standing orders.
- Stay with the patient — your presence is calming and allows rapid reassessment.
- Reassure the patient and family — explain what you are doing and why.
- Give analgesia first, investigate second — comfort takes priority.
- Reassess frequently — check pain score every 15-30 minutes until controlled.
- Patient NOT already on morphine: Give stat (immediate) dose of oral morphine 5-10mg orally.
- Patient ALREADY on regular morphine: Give breakthrough/rescue dose immediately. Equivalent to their 4-hourly regular dose (e.g., if taking 10mg every 4 hours, give 10mg as breakthrough).
Why oral first? Oral morphine is effective, safe, fast-acting, and requires no needles. However, when taking morphine orally, the blood travels through the Portal Vein straight to the Liver where a massive amount of the drug is destroyed before reaching the brain (First-Pass Metabolism).
If oral is impossible, use these ratios based on circumventing the liver:
- Subcutaneous (SC): Dose is HALF the oral dose (Oral:SC ratio is 2:1) because it avoids first-pass metabolism.
- Intravenous (IV): For very rapid relief. Dose is 1/3 to 1/2 of oral dose (Oral:IV ratio is 2-3:1).
- Sublingual/Buccal/Rectal: Alternatives if vomiting or unconscious.
Wait 30 minutes after oral morphine (15 minutes after SC/IV). Reassess pain score. Ask the patient: "Has the pain changed? How bad is it now?"
- Pain relieved (score drops to ≤3/10): Continue monitoring. Document. Plan regular dosing.
- Partial relief (score improved but still 5-6/10): Repeat the same dose. Reassess in another 30 minutes.
- No relief (score unchanged/worsened to 8-10/10): Repeat the dose. Consider increasing by 50%. Call doctor for review.
Once the acute crisis is controlled, adjust the regular morphine dose:
- Calculate total morphine used in 24 hours (regular doses + breakthrough doses).
- Increase the regular 4-hourly dose based on this total. Be prepared to increase by 100% or more if the patient needed many breakthrough doses.
- Example: Patient was on 10mg every 4 hours = 60mg/day. During the emergency, needed 6 breakthrough doses of 10mg = 60mg extra. Total in 24 hours = 120mg. New regular dose = 120mg ÷ 6 = 20mg every 4 hours. This is a 100% increase — appropriate because the pain was severely uncontrolled.
Reassess pain score every 1-2 hours until stable. Review the management plan if pain is not controlled after 2-3 dose adjustments. Consider alternative causes if morphine is not working (neuropathic pain). Consider adjuvant medications.
| Cause | Specific Treatment & Physiological Rationale |
|---|---|
| Bone metastases / fracture | Radiotherapy, immobilization, surgery, NSAIDs (blocks prostaglandins), Bisphosphonates (kills bone-destroying osteoclasts) + morphine. |
| Spinal cord compression | Urgent Dexamethasone (high dose steroids massively reduce peritumoral edema taking pressure off the cord), urgent radiotherapy/surgery, morphine. |
| Visceral pain (liver, bowel) | Morphine, steroids for inflammation, antispasmodics for colic, treatment of obstruction. |
| Nerve compression / Neuropathic | Morphine (may only help partially). Adjuvants: Amitriptyline (boosts descending pain inhibition), Gabapentin/Carbamazepine (calms hyperactive nerve firing), steroids. |
| Infection / Bleeding into tumor | Antibiotics, drainage / Pressure, tranexamic acid (promotes clotting), morphine. |
- Calm environment: Reduces anxiety that chemically amplifies pain perception.
- Reassurance and explanation: "We are giving you strong medicine. The pain will get better."
- Positioning: Find the position of least pain; use pillows for support.
- Gentle touch & Cool cloth: Holding hands releases endogenous opioids (endorphins) and oxytocin, reducing fear.
- Family presence: Loved ones provide comfort; but manage them if their distress increases the patient's anxiety.
- Relaxation breathing: Once pain begins to ease, guide slow deep breathing.
- 0 min: Recognize emergency. Stay with patient. Call for help if needed. (Nurse)
- 0-5 min: Rapid PQRST assessment. Check vital signs. (Nurse)
- 5-10 min: Give stat oral morphine (5-10mg if not on morphine; breakthrough dose if on morphine). (Nurse per standing orders)
- 10-15 min: Reassure patient and family. Position for comfort. Document. (Nurse)
- 15-30 min: Reassess pain score.
- 30 min: If pain persists, repeat dose or increase by 50%.
- 30-60 min: Continue reassessment every 15-30 minutes until pain ≤3/10.
- 60 min: Once controlled, calculate total 24-hour morphine used. Adjust regular dose. Assess for cause of sudden pain escalation.
- Regular monitoring: Check pain score every 1-2 hours initially, then every 4 hours.
- Prevent constipation: Start or increase laxatives with EVERY opioid dose (Opioids paralyze the gut).
- Treat nausea: Give antiemetics if morphine causes vomiting (Stimulates the Chemoreceptor Trigger Zone - CTZ).
- Address cause: Arrange radiotherapy, surgery, antibiotics.
- Psychosocial support, Documentation, Education: Talk with family, record doses, teach family about breakthrough doses.
| Challenge | Nursing Response |
|---|---|
| Morphine availability: Not all facilities have it. | Use what is available (tramadol, pethidine short-term). Advocate urgently with pharmacy and management. |
| Transport delays: Patients in rural areas take hours to reach help. | Train family members to give oral morphine at home (Task Shifting). Provide clear written instructions and phone support. |
| Family fear of morphine: Belief that it kills. | Explain that morphine relieves pain and does not hasten death. Share success stories. Involve a respected elder or religious leader. |
| Cost of specific treatments: Radiotherapy/surgery unaffordable. | Focus on what CAN be done: morphine, positioning, family support, comfort care. Do NOT make the family feel guilty. |
| Limited diagnostic tools: No X-rays or CT scans. | Use clinical judgment. If a patient has sudden back pain with leg weakness, treat as possible spinal cord compression with steroids + morphine immediately while arranging transfer. |
| Multiple patients, few nurses: Cannot stay constantly. | Prioritize the patient in severe pain. Delegate other tasks. Ask family members to help with non-clinical care. |
Accurate documentation is essential for continuity, legal protection, and quality improvement. You must record:
- Date and time: When emergency began and when each action was taken.
- Initial assessment: PQRST findings, pain score, vital signs, physical findings.
- Actions taken: Doses given, route, time; non-pharmacological measures.
- Patient response: Pain scores after each intervention; side effects observed.
- Family communication: What was explained; their understanding and consent.
- Medical review: Doctor contacted; orders received; further plan.
- Outcome & Follow-up: Was pain controlled? Final regular dose? Monitoring schedule; education given.
"Where? What? Why?"
- Where is the patient on their disease trajectory?
- What is causing this problem at this time?
- Why (what ideas, concerns, expectations) do the patient and family have?
"RAPID-CARE"
- Reversibility — can it be reversed?
- Availability — is treatment available?
- Prognosis — where is the patient in their illness?
- Impact — how will this affect quality life?
- Diagnosis — what is the exact problem?
- Condition — how strong is the patient?
- Affordability — can the family pay?
- Requests — what do patient/family want?
- Effectiveness — will treatment help or harm?
"MORPHINE-STAT"
- Morphine immediately (stat dose)
- Oral route preferred
- Reassess every 30 minutes
- Pain score check
- Help family stay calm
- Increase dose if needed (50-100%)
- Non-pharmacological comfort measures
- Explain everything to patient and family
- Specific cause treatment once pain controlled
- Titrate regular dose based on total 24-hour use
- Adjuvants for nerve pain, bone pain, inflammation
- Teach family about breakthrough doses
"Please Question Robert Swiftly Today"
- Position / Precipitating factors
- Quality
- Radiation
- Severity & Site
- Timing & Treatment tried
- Define palliative care emergency and explain how it differs from general medical emergencies.
- List the 8 considerations for managing palliative care emergencies.
- Name the 3 critical questions to ask in any emergency and explain why each matters.
- Explain why severe uncontrolled pain is a palliative care emergency (Mention Central Sensitization/Chronic rewiring!).
- Describe the types of acute pain in palliative care (anticipatory, procedural, acute-on-chronic, breakthrough).
- List common causes of severe uncontrolled pain in palliative patients.
- Describe the rapid PQRST assessment for pain emergency.
- Explain the pharmacological management step-by-step: stat dose → assess response → repeat → titrate regular dose.
- Calculation Practice: Calculate a morphine dose increase based on breakthrough use.
- Discuss specific management for bone metastases, spinal cord compression, and neuropathic pain as causes of severe pain.
- Address the challenges of managing pain emergencies in rural Uganda and nursing responses.
- Explain the importance of non-pharmacological measures during a pain emergency.
- World Health Organization (WHO). (2014). Global atlas of palliative care at the end of life.
- African Palliative Care Association (APCA). (2010). Guidelines for Providing Palliative Care to People Living with HIV/AIDS and Cancer in Sub-Saharan Africa.
- Ferrell, B. R., & Coyle, N. (Eds.). (2010). Oxford Textbook of Palliative Nursing. Oxford University Press.
- Ministry of Health, Republic of Uganda. (2021). National Palliative Care Guidelines.
- Twycross, R., & Wilcock, A. (2011). Introducing Palliative Care. Radcliffe Publishing.
Thanks papa