
Hypercalcaemia is a life-threatening metabolic disorder characterized by an abnormally high level of calcium ions circulating in the blood. It is one of the most common metabolic emergencies in patients with advanced cancer and is considered a palliative care emergency because it can cause severe symptoms, rapid deterioration, and death if not recognized and treated promptly.
In the context of palliative care, hypercalcaemia is particularly important because:
- It often occurs in patients who are already frail and near the end of life.
- Its symptoms (confusion, drowsiness, nausea, constipation) are easily mistaken for "normal" progression of advanced disease.
- It is potentially reversible — treatment can restore quality of life even in terminal illness.
- Untreated, it leads to coma and death.
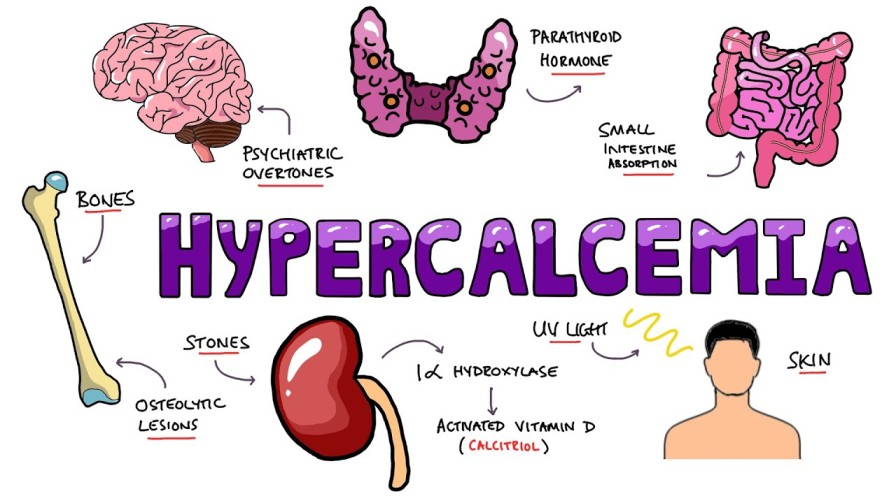
Normally, blood calcium is tightly regulated between 2.20 and 2.60 mmol/L by three things: Parathyroid Hormone (PTH) (which pulls calcium from bones into blood), Vitamin D (which absorbs calcium from the gut), and Calcitonin (which pushes calcium back into bones). In cancer, this delicate balance is completely hijacked, flooding the blood with toxic levels of calcium.
A diagnosis of hypercalcaemia is made when:
- Serum calcium level is greater than 2.60 mmol/L (or >10.4 mg/dL)
In Uganda, where laboratory facilities may be limited, nurses must maintain a high index of suspicion based on clinical symptoms, especially in patients with cancers known to cause hypercalcaemia.
| Reason | Explanation |
|---|---|
| Rapid onset and progression | Can develop over days to weeks, worsening quickly. |
| Severe, multi-system symptoms | Affects the brain, gut, kidneys, heart, and bones simultaneously. |
| Potentially reversible | Unlike many terminal complications, hypercalcaemia often responds well to treatment, giving the patient valuable extra time. |
| Easily missed | Symptoms mimic other problems (dehydration, opioid side effects, disease progression). |
| Poor prognosis indicator | Its development signals advanced disease; 80% of cancer patients with hypercalcaemia survive less than one year. |
| Fatal if untreated | Progresses to unconsciousness, cardiac arrest, and death. |
Hypercalcaemia associated with cancer is referred to as Hypercalcaemia of Malignancy (HCM). It is usually secondary to a paraneoplastic process (substances released by the tumor that act distantly) rather than simply from direct bone metastases.
Cancers Commonly Associated with Hypercalcaemia:
| Cancer Type | Notes |
|---|---|
| Squamous cell carcinoma | Very common cause; tumors produce parathyroid hormone-related peptide (PTHrP). |
| Head and neck cancer | Often squamous cell type; PTHrP production. |
| Cancer of the breast | Both paraneoplastic and bone metastases contribute. |
| Cancer of the bronchus (lung) | Especially squamous cell lung cancer; PTHrP is major cause. |
| Renal cell carcinoma (kidney cancer) | Produces substances that raise calcium. |
| Cervical cancer | Can cause HCM, especially advanced stages. |
| Oesophageal carcinoma | Squamous cell type commonly associated. |
| Haematological malignancies | Multiple myeloma, lymphoma, leukemia. |
| Melanoma | Less common but documented. |
Important Note: Hypercalcaemia is relatively rare in adenocarcinomas (gland-forming cancers like some breast and lung cancers) compared to squamous cell cancers.
| Mechanism | Explanation & Physiological Detail |
|---|---|
| Paraneoplastic hormone production | Tumors release PTHrP (parathyroid hormone-related peptide), which mimics normal PTH at the receptor level and causes:
|
| Lytic bone metastases | Tumors embedded in bones (especially breast, myeloma, lung) physically destroy bone tissue, releasing trapped calcium into the blood. |
| Decreased urinary calcium excretion | Some tumors or hormones reduce the kidneys' ability to filter and excrete calcium into the urine. |
| Osteoclast activation | Tumor factors stimulate osteoclasts (the macrophage-like cells that break down bone via the RANK/RANKL pathway), massively increasing bone resorption. |
Key point: In many cases, bone metastases are NOT the main cause — the tumor itself secretes hormones that raise calcium. This means hypercalcaemia can occur even without visible bone disease.
In palliative care patients, non-malignant factors can contribute to or worsen hypercalcaemia:
| Factor | How It Contributes |
|---|---|
| Immobility | Lack of weight-bearing mechanical stress on bones causes rapid bone resorption (calcium release). Bedridden patients are at high risk. |
| Dehydration | Low blood volume concentrates existing calcium and reduces kidney excretion. Very common in terminally ill patients. |
| Excessive calcium intake | Overuse of calcium supplements or antacids containing calcium. |
| Excessive Vitamin D intake | Vitamin D increases calcium absorption from the gut. |
| Decreased parathyroid hormone (PTH) | Paradoxically, low PTH can occur in some malignancies as the body tries to shut down natural calcium production. |
| Vitamin A intoxication | Excess vitamin A increases bone resorption. |
| Thiazide diuretics | Some blood pressure medicines reduce calcium excretion by the kidneys. |
In Uganda: Dehydration and immobility are extremely common in palliative care patients and may be the triggering factors that convert "borderline high calcium" into severe, symptomatic hypercalcaemia.
The symptoms of hypercalcaemia are multi-system and often non-specific. Many are common in patients with advanced disease anyway, which is why hypercalcaemia is so easily missed.
Calcium stabilizes the sodium channels on cell membranes. When calcium is abnormally HIGH, it raises the threshold for an action potential. This means nerves and muscles become less excitable and sluggish. This perfectly explains the severe muscle weakness, the slowing down of the gut (constipation), and the slowing down of the brain (drowsiness and coma).
| Symptom | Description | Why It Occurs |
|---|---|---|
| General malaise | Feeling unwell, tired, "not right" | High calcium affects multiple body systems. |
| Fatigue | Overwhelming tiredness, weakness | Muscle weakness from decreased nerve excitability; dehydration. |
| Anorexia | Loss of appetite, refusing food | Gut slowdown; nausea; metabolic disturbance. |
| Symptom | Description | Why It Occurs |
|---|---|---|
| Nausea and vomiting | Feeling sick, throwing up | High calcium directly stimulates the chemoreceptor trigger zone (vomiting center) in the brain; gut stasis. |
| Constipation | Severe, persistent constipation | Calcium slows smooth muscle contraction (peristalsis) in the gut; dehydration worsens it. |
| Abdominal pain | Cramping, discomfort | Constipation, gut distension, possible peptic ulceration (calcium increases gastrin secretion). |
Nursing implication: A patient on morphine who develops worsening constipation despite regular laxatives should raise suspicion for hypercalcaemia — it may not be "just the morphine."
| Symptom | Description | Why It Occurs |
|---|---|---|
| Thirst (polydipsia) | Intense, unquenchable thirst | The body tries to dilute high calcium by increasing fluid intake. |
| Polyuria | Passing large amounts of urine | High calcium interferes with ADH in the kidneys (nephrogenic diabetes insipidus), causing massive water loss. |
| Severe dehydration | Dry mouth, sunken eyes, poor skin turgor, hypotension | Excessive urine output + vomiting + poor oral intake = severe volume depletion. |
| Kidney stones | Flank pain, haematuria | Calcium precipitates in kidneys (rare in terminal illness but possible). |
The vicious cycle: High calcium → excessive urination (polyuria) → dehydration → concentrated blood calcium → even higher calcium levels → worse symptoms.
These are often the most frightening and are frequently mistaken for "the patient is dying."
| Symptom | Description | Severity |
|---|---|---|
| Drowsiness | Increasing sleepiness, hard to wake | Early sign |
| Confusion | Disoriented, doesn't recognize family, agitated | Moderate |
| Mental state changes | Poor concentration, memory loss, irritability, mood changes | Moderate |
| Depression | Sadness, hopelessness, withdrawal | Can be misdiagnosed as psychological |
| Hallucinations | Seeing or hearing things that aren't there | Severe |
| Jumbled/slurred speech | Difficulty finding words, incoherent speech | Severe |
| Visual changes | Blurred vision, double vision, light sensitivity | Severe |
| Unconsciousness (coma) | Cannot be aroused | Life-threatening |
| Death | Cardiac arrest from severe hypercalcaemia | Fatal if untreated |
Critical nursing point: When a patient with advanced cancer suddenly becomes confused or very drowsy, do not automatically assume "they are near death." Check for hypercalcaemia. It may be easily reversible.
| Symptom | Description | Why It Occurs |
|---|---|---|
| Bone pain | Deep, aching pain in bones | Underlying bone metastases; increased bone turnover and destruction by osteoclasts. |
| Symptom | Description | Why It Occurs |
|---|---|---|
| Cardiac arrhythmias | Irregular heartbeat, palpitations, fainting | Calcium alters the action potential in cardiac muscle (specifically, it drastically shortens the QT interval on an ECG). |
| Hypertension | High blood pressure | Vascular smooth muscle spasm caused by calcium. |
| Bradycardia or tachycardia | Slow or fast heart rate | Depends on severity and individual response. |
🧠 MOANS, GROANS, STONES, BONES, and PSYCHIATRIC OVERTONES
- M - Moans/Muscular: Weakness, fatigue, malaise.
- G - Groans: Abdominal groaning from pain, severe constipation, nausea, vomiting.
- S - Stones: Kidney stones, polyuria, polydipsia, dehydration (Renal).
- B - Bones: Bone pain from metastases.
- O - Overtones (Psychiatric): Drowsiness, confusion, depression, hallucinations, coma.
- Additional E's & S's: Electrocardiac arrhythmias, Stupor/coma.
In a resource-limited setting like Uganda, clinical suspicion is the most important diagnostic tool. Many of the symptoms above, occurring together in a patient with known cancer, should immediately trigger suspicion of hypercalcaemia.
Key clinical clues:
- Confusion or drowsiness in a patient who was previously alert.
- Severe constipation "out of proportion" to expected side effects of opioids.
- Intense thirst with excessive urination.
- Worsening nausea and vomiting.
- Known cancer associated with hypercalcaemia (Squamous, Breast, Renal, Myeloma).
| Test | Purpose | Finding in Hypercalcaemia |
|---|---|---|
| Serum calcium | Primary diagnostic test | >2.60 mmol/L (or >10.4 mg/dL) |
| Corrected calcium | Adjusts for low albumin (common in cancer patients) | More accurate than total calcium if albumin is low. (Formula: Measured Ca + 0.02 * (40 - patient albumin)) |
| Ionized calcium | Measures "free" calcium (biologically active) | More precise; not always available. |
| Parathyroid hormone (PTH) | Differentiates causes | Suppressed/low in malignancy (because the tumor makes PTHrP, not actual PTH). |
| PTHrP | Confirms paraneoplastic cause | Elevated in many malignancies. |
| Kidney function tests (BUN, creatinine) | Assess renal impact | May show acute kidney injury (AKI) from profound dehydration. |
| Serum phosphate | Often low in hypercalcaemia | Low phosphate supports diagnosis. |
| Serum magnesium | May be low | Needs correction for effective treatment. |
| 24-hour urine calcium | Assesses urinary excretion | May be high or low depending on cause. |
| Complete blood count (CBC) | Baseline assessment | May show anaemia of chronic disease. |
| Liver function tests | Assess organ function | Baseline before some treatments. |
Nursing implication: If laboratory facilities are available, prioritize serum calcium and kidney function tests. These guide immediate fluid treatment decisions.
| Test | Purpose |
|---|---|
| X-rays | Look for lytic bone lesions, pathological fractures. |
| Bone scan | Identifies areas of increased bone turnover/metastases. |
| CT scan | Assess overall tumor burden, bone involvement. |
| MRI | Detailed imaging of bones and soft tissues. |
In Uganda: Advanced imaging is often unavailable. Do not delay treatment while waiting for imaging if clinical suspicion is high.
"The development of hypercalcaemia is a poor prognostic sign. 80% of cancer patients with hypercalcaemia will survive less than one year."
This does NOT mean treatment is futile. It means:
- The underlying cancer is highly advanced.
- However, treating hypercalcaemia can restore weeks or months of quality life.
- The patient may be able to go home, see family, settle affairs, and die peacefully rather than in a state of confused agony.
The management of hypercalcaemia follows a stepwise approach, from simple measures to more intensive interventions.
Hydration is the first and most important treatment. Most patients with hypercalcaemia are severely dehydrated due to polyuria, vomiting, and poor oral intake.
Mild Hypercalcaemia
| Intervention | Detail |
|---|---|
| Normal saline | 100–120 ml/hour intravenously. |
| Oral fluids | Encourage 1–2 liters per day if the patient can tolerate oral intake. |
| Monitoring | Watch for fluid overload in frail or heart failure patients. |
Outcome: Rehydration alone is sufficient in a small number of cases, especially if hypercalcaemia is mild and mainly due to dehydration.
Moderate to Severe Hypercalcaemia
| Intervention | Detail |
|---|---|
| Aggressive IV rehydration | 5–10 liters of fluid over 24–48 hours (in hospital setting). |
| Normal saline (0.9% NaCl) | Preferred; restores extracellular volume and promotes calcium excretion. (Physiology note: Sodium and Calcium share a transporter in the kidneys. Flooding the kidney with Sodium forces it to dump Calcium into the urine!) |
| Close monitoring | Vital signs, fluid balance, weight, signs of fluid overload. |
Nursing responsibilities during rehydration:
- Monitor fluid intake and output meticulously.
- Check vital signs regularly (dehydration causes hypotension; over-hydration causes heart failure).
- Watch for signs of fluid overload: breathlessness, lung crackles, peripheral edema, raised jugular venous pressure.
- In frail patients, use lower infusion rates and monitor more closely.
- Keep accurate fluid balance charts.
Bisphosphonates are the mainstay of definitive treatment for moderate to severe hypercalcaemia of malignancy. They work by inducing apoptosis (cell death) in osteoclasts (the cells that break down bone), thereby shutting off the release of calcium from bones.
| Drug | Dose | Administration | Notes |
|---|---|---|---|
| Pamidronate | 60–90 mg | Intravenous infusion over 24 hours | Most commonly used in palliative care. |
| Zoledronic acid | 4 mg | IV infusion over 15 minutes | Faster but more nephrotoxic. |
| Ibandronate | 2–6 mg | IV | Alternative option. |
Important considerations for Bisphosphonates:
| Consideration | Detail |
|---|---|
| Hydration first | Ensure the patient is fully rehydrated BEFORE giving bisphosphonates. Dehydration severely increases kidney damage risk. |
| Slow infusion | Rapid infusion causes kidney damage and other side effects. |
| Onset of action | Calcium levels begin to fall within 24–48 hours; nadir (lowest point) is reached at 3–7 days. |
| Duration of effect | Usually lasts 3–4 weeks; may need repeating. |
| Side effects | Fever, flu-like symptoms (first dose), hypocalcaemia (dropping calcium too low), kidney damage, osteonecrosis of jaw (rare, with repeated use). |
| Availability in Uganda | Often not available in resource-poor settings due to high cost. |
Nursing implication: If bisphosphonates are unavailable (common in Uganda), focus strictly on aggressive rehydration, mobilization, and symptom control. Do not give up — these measures alone can help significantly.
| Use | Detail |
|---|---|
| Indication | Haematological malignancies (multiple myeloma, lymphoma, leukemia) and some solid tumors. |
| Effectiveness | Less effective in solid tumors compared to bisphosphonates. |
| Mechanism | Reduce tumor production of calcium-raising substances (like Vitamin D analogs in lymphomas); may have a direct anti-tumor effect. |
| Example | Dexamethasone 4–8 mg daily. |
| Caution | Side effects: gastric irritation, hyperglycaemia, immunosuppression, mood changes. |
Where appropriate and available:
- Chemotherapy: for responsive tumors (myeloma, lymphoma, breast cancer).
- Radiotherapy: for painful bone metastases causing calcium release.
- Hormonal therapy: for hormone-sensitive cancers (breast, prostate).
In Uganda: These treatments may be limited. The nurse's role is to advocate for referral where possible and to focus on what can be done when they are not available.
| Measure | Purpose | Application |
|---|---|---|
| Mobilization | Weight-bearing physical activity reduces bone resorption. | Encourage sitting, standing, walking if possible. |
| Stop calcium supplements | Remove unnecessary external calcium intake. | Review all medications and supplements. |
| Stop thiazide diuretics | These specific diuretics reduce calcium excretion by the kidney. | Consult doctor about alternative blood pressure medicines (like Loop diuretics, which actually help excrete calcium). |
| Treat constipation aggressively | Comfort measure; also reduces gut calcium absorption. | Regular laxatives, enemas if needed. |
In some cases, bisphosphonates are not available (common in rural Uganda), the patient is in the active terminal phase of disease, or the burden of hospitalization and IV fluids outweighs the benefit. In these situations, the focus shifts entirely to comfort, dignity, and symptom control:
| Intervention | How It Helps |
|---|---|
| Regular mouth care | Relieves dry mouth from dehydration; prevents infections. |
| Bowel care | Treats constipation aggressively; prevents obstruction and severe discomfort. |
| Regular turning | Prevents pressure sores in bedridden, immobile patients. |
| Effective pain control | Morphine for bone pain and abdominal discomfort. |
| Anti-emetics | Control nausea and vomiting. |
| Reassurance and presence | Confused patients need calm, familiar faces; gentle reorientation. |
| Family support | Prepare family for the dying process; explain exactly what is happening (e.g., "The confusion is from the disease affecting the blood, not because they are going crazy"). |
| Spiritual care | Address fear, guilt, and existential distress. |
| Parameter | What to Assess | Frequency |
|---|---|---|
| Consciousness level | Alert? Drowsy? Confused? Comatose? | Every 1–2 hours during acute phase |
| Vital signs | BP, pulse, respiratory rate, temperature | Every 1–2 hours |
| Fluid balance | Intake (oral + IV) vs. output (urine + vomit + stool) | Hourly during IV rehydration |
| Hydration status | Skin turgor, mucous membranes, eye sunkenness | Every 4 hours |
| Gut function | Nausea, vomiting, bowel movements, abdominal distension | Every shift |
| Neurological signs | Orientation, speech, mood, hallucinations | Every 1–2 hours |
| Pain | Bone pain, abdominal pain | Every 1–2 hours |
| Cardiac monitoring | Heart rhythm, rate | Continuous if arrhythmias suspected |
| Nursing Diagnosis | Rationale |
|---|---|
| Risk for injury related to confusion and drowsiness | High calcium causes severe neurological impairment. |
| Deficient fluid volume related to polyuria and vomiting | Dehydration is central to the pathophysiology of hypercalcaemia. |
| Constipation related to high calcium and dehydration | Gut smooth muscle paralysis due to altered action potentials. |
| Inadequate protein energey intake | Anorexia, nausea, vomiting prevent intake. |
| Acute pain related to bone metastases and gut distension | Bone destruction and severe constipation pain. |
| Excessive Anxiety/fear related to confusion and prognosis | Patient and family distress regarding rapid cognitive decline. |
| Risk for impaired skin integrity | Immobility, severe dehydration, incontinence. |
| Intervention | Rationale | Nursing Action |
|---|---|---|
| Administer IV fluids as prescribed | Rehydration is the foundation of treatment. | Monitor infusion rate; record strict fluid balance; watch for fluid overload (crackles in lungs). |
| Monitor serum calcium | Guides treatment response. | Arrange blood tests; communicate results immediately to team. |
| Administer bisphosphonates safely | Definitive treatment to stop bone breakdown. | Ensure hydration first; give slow infusion; monitor for fever and kidney function. |
| Give anti-emetics | Control nausea. | Metoclopramide, haloperidol, or ondansetron as prescribed. |
| Aggressive bowel care | Relieve constipation. | Regular laxatives; enemas; manual evacuation if strictly needed. |
| Reorient confused patients | Safety and comfort. | Use calm voice, familiar faces, clocks, daylight. |
| Protect from injury | Confusion causes falls and harm. | Side rails, close observation, family at bedside. |
| Mouth care | Comfort and infection prevention. | Every 2 hours; soft toothbrush; lip balm; oral antifungals if needed. |
| Skin care | Prevent pressure sores. | Turn every 2 hours; inspect skin; keep clean and dry. |
| Family education | Reduce anxiety; enable home care. | Explain hypercalcaemia, treatment, prognosis, and what to expect. |
| Psychosocial support | Address fear and grief. | Listen, counsel, pray, link with support services. |
Challenges and Nursing Responses
| Challenge | Nursing Response / Impact |
|---|---|
| Limited laboratory access | Serum calcium may not be available. Response: Maintain high clinical suspicion. Treat based on classic symptoms and known cancer type. |
| Bisphosphonates unavailable or unaffordable | Definitive treatment often not possible. Response: Maximize rehydration (oral if IV impossible). Mobilize if possible. Aggressive symptom control. |
| IV rehydration requires hospitalization | Patients may prefer home; families cannot afford hospital stay. Response: Teach family oral rehydration (ORS, water). Arrange community nurse follow-up. Provide clear "when to call" instructions. |
| Multiple patients, limited staff | Close monitoring is difficult. Response: Prioritize the sickest patients. Train family members in basic monitoring (consciousness, fluid intake, urine output). |
| Symptoms mistaken for "normal dying" | Hypercalcaemia is missed; patient dies unnecessarily confused and uncomfortable. Response: Educate all staff: confusion + thirst + constipation + known cancer = think hypercalcaemia! |
| Topic | What to Teach |
|---|---|
| What hypercalcaemia is | "The calcium in your blood is too high. This is making you confused, thirsty, and constipated." |
| Why treatment helps | "Fluids and medicine can lower the calcium and make you feel much better." |
| What to expect | "You should start feeling clearer and more comfortable within 1–2 days." |
| Home care if discharged | "Drink as much as you can. Take your laxatives. Call us if you become very sleepy or confused again." |
| When to seek help | Worsening drowsiness, new confusion, severe constipation, vomiting, inability to urinate. |
| Prognosis | Be honest: "This shows the cancer is advanced. Treatment can help you feel better, but it is not a cure." |
| Element | What to Record |
|---|---|
| Baseline assessment | Symptoms, consciousness level, pain score, hydration status. |
| Investigations | Serum calcium, kidney function, other labs; imaging if done. |
| Treatment given | IV fluids (type, rate, total volume); bisphosphonate (drug, dose, time); other medications. |
| Patient response | Changes in consciousness, pain, bowel function, hydration. |
| Fluid balance | Detailed intake and output chart. |
| Family communication | What was explained; their understanding; concerns. |
| Plan | Continue/discontinue treatments; discharge plan; follow-up. |
🧠 The "CALCIUM" Emergency Checklist
- C - Check calcium level (or suspect clinically)
- A - Assess hydration status
- L - Load with IV fluids (rehydrate)
- C - Consider bisphosphonates
- I - Investigate underlying cause
- U - Urge mobilization if possible
- M - Manage symptoms (pain, nausea, constipation, confusion)
🧠 Cancers Causing Hypercalcaemia: "My Skin Burns Like Crazy"
- Myeloma
- Squamous cell (lung, head, neck, esophagus, cervix)
- Breast
- Lung (bronchus)
- Cancer of Kidney (renal cell) & Cervix
🧠 Nursing Priorities: "FLUID-CARE"
- Fluids (rehydration is first!)
- Labs (check calcium if available)
- Urge family to encourage oral fluids
- Investigate cause (cancer type, medications)
- Drug treatment (bisphosphonates, steroids)
- Constipation management (aggressive)
- Alertness monitoring (consciousness level)
- Reassurance and reorientation
- Educate family
📝 Must-Know For Your Exam
- Define hypercalcaemia and state the diagnostic threshold (>2.60 mmol/L).
- Explain why it is a palliative care emergency (reversible, fatal if untreated, easily missed).
- Distinguish between paraneoplastic hypercalcaemia (tumor secretes PTHrP) and bone metastasis hypercalcaemia (tumor physically destroys bone).
- List at least 8 cancers commonly associated with hypercalcaemia (Use the My Skin Burns Like Crazy mnemonic).
- Describe the mechanism by which tumors cause hypercalcaemia (PTHrP, osteoclast activation).
- List non-cancer causes of hypercalcaemia (immobility, severe dehydration, excess calcium/Vitamin D, Thiazide diuretics).
- Use the "stones, bones, groans, moans, psychiatric overtones" mnemonic to describe symptoms.
- Explain why confusion in a cancer patient should trigger suspicion of hypercalcaemia (don't assume they are just dying!).
- Describe the stepwise management: Rehydration → Bisphosphonates → Steroids → Treat underlying cancer.
- Discuss rehydration protocols for mild vs. moderate-severe hypercalcaemia (Normal Saline is king).
- Explain nursing responsibilities during IV rehydration (monitoring for fluid overload, strict fluid balance charts).
- Discuss the challenges of managing hypercalcaemia in Uganda and nursing responses (advocating for hydration and symptom control when bisphosphonates are absent).
- Describe end-of-life care when definitive treatment is unavailable (focus strictly on comfort, mouth care, and family education).
- World Health Organization (WHO) Guidelines on Palliative Care.
- Oxford Textbook of Palliative Medicine.
- National guidelines for the management of hypercalcaemia of malignancy.
- Core curriculum for nursing management of metabolic emergencies in advanced cancer.
Quick Quiz
Hypercalcemia Quiz
Palliative Care - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
Hypercalcemia Quiz
Palliative Care
Preparing questions...
Choose your answer and keep your streak alive.
Great effort.
Here is your quick performance summary.
Thanks alot for supporting us
The Almighty always bless you for the work