


PUBERTY
Puberty is the developmental stage during which a child becomes a young adult, characterized by the maturation of gametogenesis, secretion of gonadal hormones, and development of secondary sexual characteristics and reproductive functions.
Tanner Staging in Puberty:
Tanner Staging, invented by James Tanner, is a widely used system to assess the progression of puberty based on physical changes.
- Thelarche denotes the onset of breast development, an estrogen effect.
- Pubarche denotes the onset of sexual hair growth, an androgen effect.
- Menarche indicates the onset of menses.
- Spermarche the appearance of spermatozoa in seminal fluid.
- Gonadarche refers to the earliest gonadal changes of puberty.
Tanner Stages in Females:
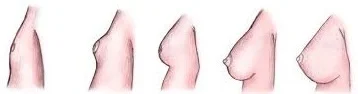
Breast Development (Thelarche):
- Stage 1 (Preadolescent): No glandular tissue; only the papilla elevated.
- Stage 2: Breast buds appear, along with a small mound of breast and papilla enlargement.
- Stage 3: Further enlargement, with the breast mound elevating, and areola enlargement.
- Stage 4: Continued enlargement, areola forms a secondary mound above the breast.
- Stage 5 (Adult): Mature breast; areola returns to general breast contour.

Pubic Hair Development (Pubarche):
- Stage 1 (Preadolescent): No pubic hair.
- Stage 2: Sparse, long, downy hair, mostly along the labia.
- Stage 3: Darker, coarser, curlier hair spreading over the mons pubis.
- Stage 4: Hair resembles that of an adult, but less in quantity.
- Stage 5 (Adult): Adult distribution; extends to inner thighs.
Tanner Stages in Males:

Genital Development (Gonadarche):
- Stage 1 (Preadolescent): Testes, scrotum, and penis are at childhood size.
- Stage 2: Testes and scrotum enlarge; reddening of scrotum.
- Stage 3: Penis lengthens; continued testicular and scrotal growth.
- Stage 4: Increased penis size; scrotum darkens.
- Stage 5 (Adult): Mature genitalia; adult size and shape.

Pubic Hair Development (Pubarche):
- Stage 1 (Preadolescent): No pubic hair.
- Stage 2: Sparse, long, downy hair at the base of the penis.
- Stage 3: Darker, coarser, curlier hair spreading over the pubic symphysis.
- Stage 4: Hair resembles an adult, but less in quantity.
- Stage 5 (Adult): Adult distribution; extends to inner thighs.




This topic is so teaching ,thanks julius
👍🆗
EDUCATIVE