


Signs and Symptoms of Cerebral Palsy (CP)
I. Developmental Milestones and Motor Function:
- Delayed achievement of developmental milestones; Not reaching expected physical and cognitive milestones within typical time frames.
- Abnormal motor development and coordination; Lack of smooth, coordinated muscle movements during development.
- Unusual gait patterns; Unusual walking patterns that may indicate motor control issues.
II. Muscle Tone and Reflexes:
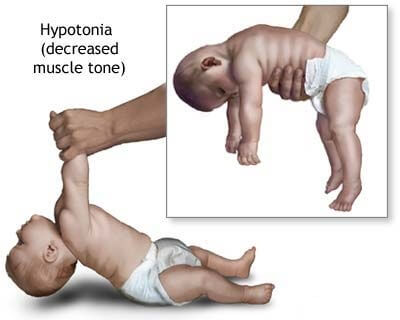
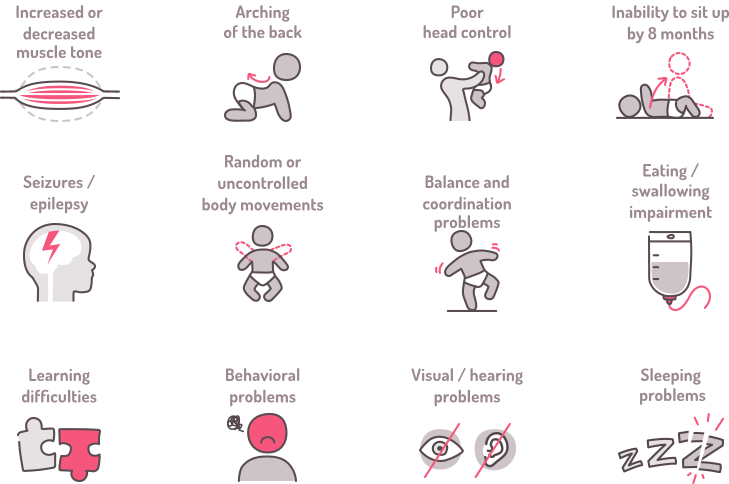
- Abnormal muscle tone; Muscles may be too tight (spasticity) or too floppy (hypotonia).
- Spasticity or hypertonia; Increased muscle stiffness, making movement challenging.
- Hypotonia in some cases; Reduced muscle tone leading to poor muscle control.
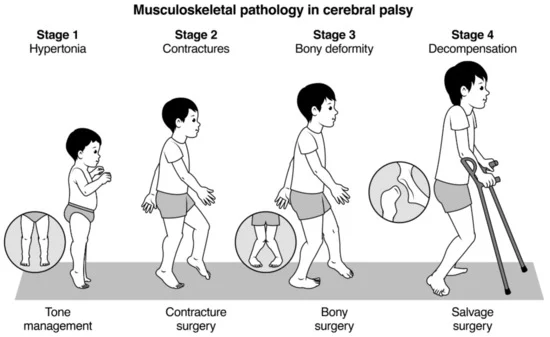
III. Joint and Skeletal Abnormalities:
- Joint contractures; Limited movement in joints due to tight muscles.
- Dynamic deformities progressing to static deformities; Irregular bone and joint development due to muscle imbalances.
- Bone and joint deformities due to unequal growth; Asymmetric bone growth caused by muscle-related stresses.
IV. Coordination and Movement Issues:
- Difficulty with precise movements; Challenges in performing accurate and controlled movements.
- Incoordination and tremors; Lack of coordination and uncontrollable shaking during movement.
- Challenges in voluntary muscle control; Difficulty in intentionally controlling muscle actions.
V. Speech and Communication:
- Speech and language disorders; Difficulty in articulating words or understanding language.
- Dysarthria (impaired speech due to muscle control); Speech difficulties resulting from poor muscle control.
- Non-verbal communication in some cases; Reliance on gestures or other non-verbal cues for communication.
VI. Cognitive and Behavioral Aspects:
- Learning disabilities; Difficulty in acquiring knowledge and skills.
- Intellectual disabilities in some cases; Below-average intellectual functioning.
- Behavioral challenges; Emotional or behavioral issues that may impact daily life.
VII. Sensory and Perception Issues:
- Visual impairments; Problems with vision or visual processing.
- Auditory impairments; Hearing difficulties or processing issues.
- Sensory processing difficulties; Challenges in interpreting and responding to sensory information.
VIII. Seizures:
- Epilepsy in a significant percentage of cases; Recurrent seizures affecting brain function.
IX. Posture and Balance:
- Poor posture; Inability to maintain an upright and balanced body position.
- Balance issues; Difficulty in maintaining stability during movement or at rest.
X. Fine and Gross Motor Skills:
- Impaired fine motor skills; Difficulty in performing precise tasks with hands and fingers.
- Difficulty with gross motor skills; Challenges in performing larger movements like crawling, walking, or jumping.
XI. Feeding and Eating Difficulties:
- Challenges in chewing and swallowing; Difficulty in the process of biting, chewing, and swallowing food.
- Gastro-oesophageal reflux; Stomach contents flowing back into the esophagus.
- Nutritional concerns; Issues related to inadequate nutrient intake.
XII. Behavioral and Emotional Issues:
- Emotional challenges due to limitations; Psychological struggles arising from physical constraints.
- Social difficulties; Challenges in interacting and forming relationships with others.
XIII. Drooling:
- Excessive drooling due to lack of control; Inability to manage saliva flow.
XIV. Pain and Sleep Issues:
- Chronic pain; Persistent discomfort or pain.
- Sleep disturbances; Interruptions in regular sleep patterns.
XV. Orthopedic Complications:
- Scoliosis; Abnormal sideways curvature of the spine.
- Hip dislocation; Displacement of the hip joint.
- Skeletal deformities; Abnormalities in bone structure and shape.

I didn’t know that cerebral paly is a non progressive disorder.
Meaning the the brain damage is not progress.
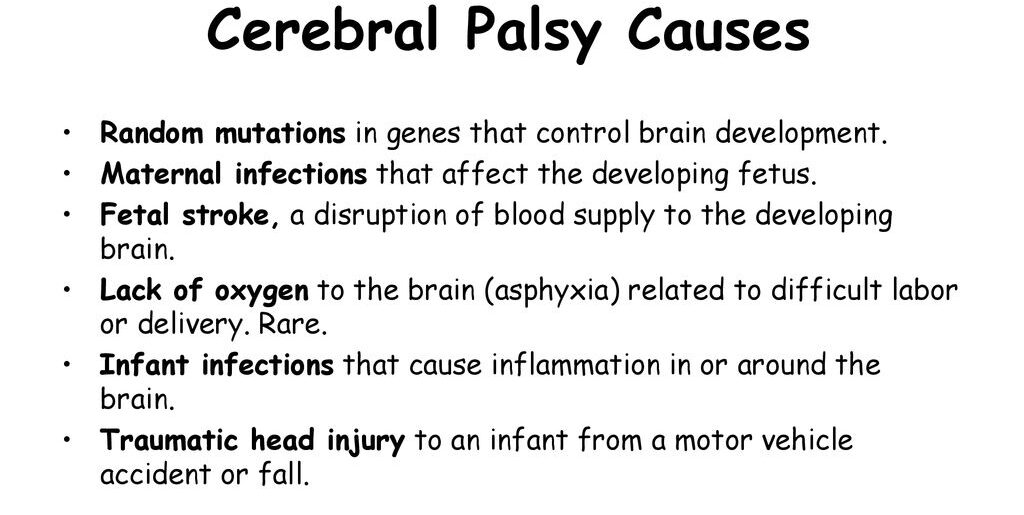
NB.In Uganda Asphyxia is the most leading cause of cerebral palsy