


INHALATION
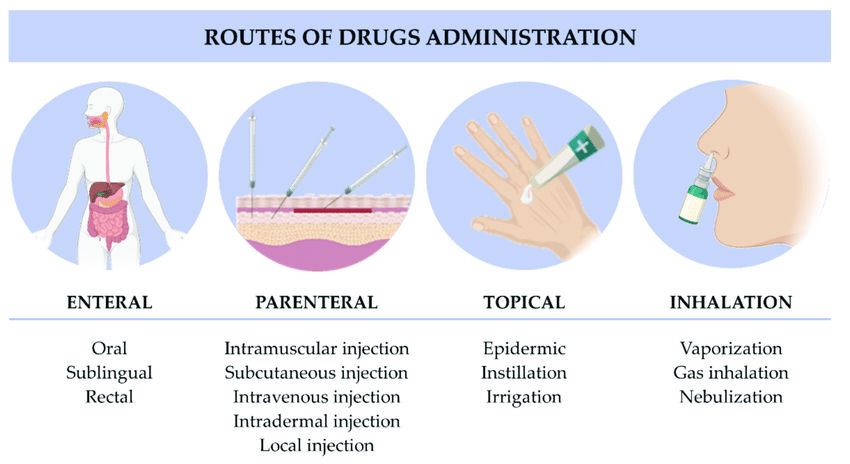
Inhalation is the breathing of air vapor or volatile medicine into the lungs.
Types
- Dry inhalation: Oxygen Administration: this is given when the respiratory capacity is diminished as in chest injuries, pneumonia and cardiac failure.
- Moist/steam inhalation: It is used in case of inflammation of air passages and the nasal sinuses. These are given to:
- Warm and moisten the air breathed in and relieve irritation e.g. in bronchitis, after tracheotomy and other chest conditions.
- To relieve inflammation and coughing e.g. in colds.
- To relieve congestion and oedema e.g. in sinusitis and acute laryngitis.
- Nebuliser: this produces vapors which is inhaled by the patient for example in asthma to relieve spasms of the bronchial tubes or for the relief of chest pain in angina pectoris. Other indications include Respiratory diseases eg asthma, pneumonia, Airway obstruction, Nasal congestion, Nasal bleeding, Chest injuries and Cardiac failure.
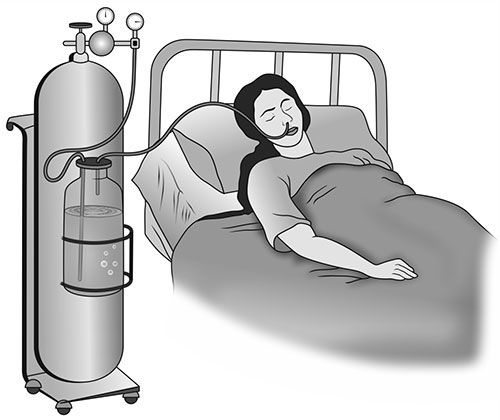
DRY INHALATION (Oxygen administration)
It is given when the respiratory tract is diminished as in chest injuries, cardiac failure and pneumonia.
REQUIREMENTS FOR OXYGEN ADMINISTRATION
Clean tray
- Rubber tubing.
- BLB oxygen mask.
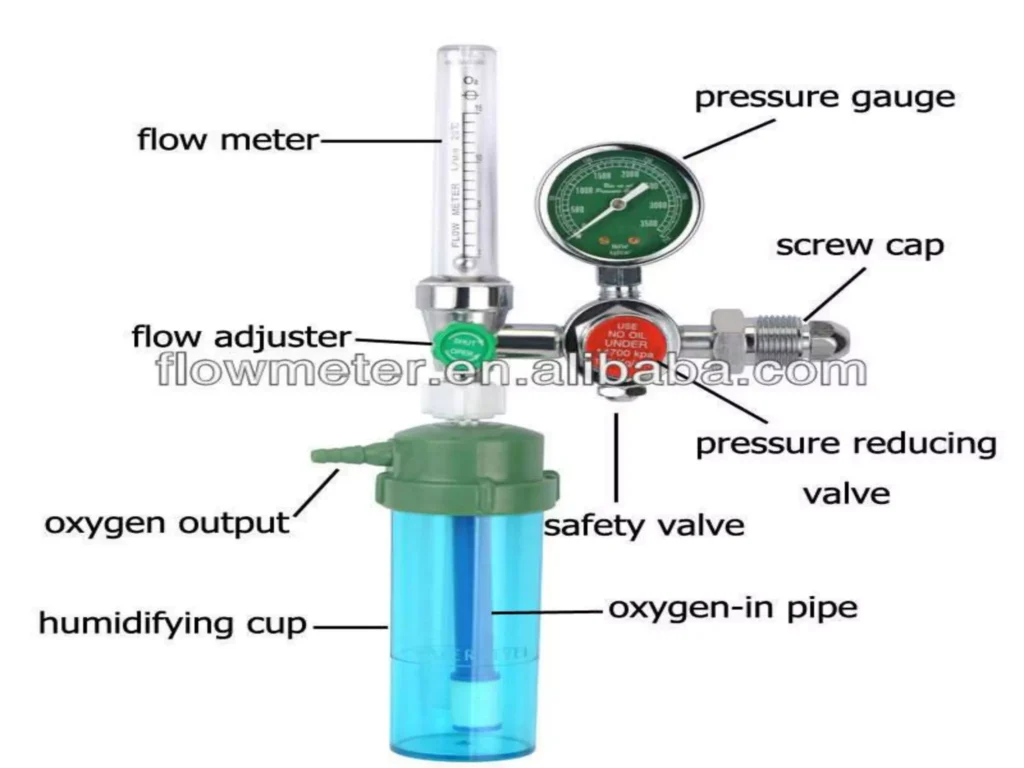
- Flowmeter.
- Nasal catheter.
- Gallipot with gauze pads.
- Humidifier with distilled water
Bedside
- Oxygen source.
- Screen
PROCEDURE
Parts of an Oxygen Flowmeter
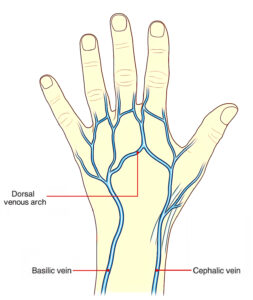
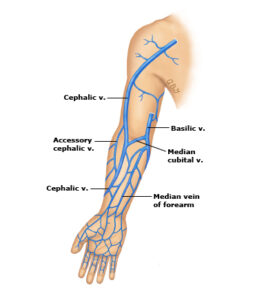
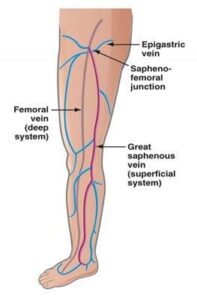
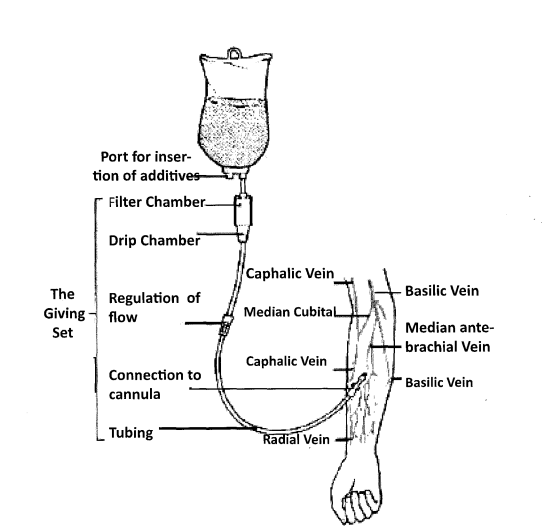
SOME OF THE RECOMMENDED VEINS FOR INTRAVENOUS INFUSION
COMPLICATIONS OF INTRAVENOUS INJECTIONS
- Incorrect IV Site Placement: Inserting the IV into the wrong vessel (e.g., artery instead of vein) can lead to severe consequences.
- Medication Errors: Misidentification of medications, incorrect dosages, or incompatible mixing can result in serious adverse reactions.
- Rapid Administration and Undesired Effects: Delivering medications too quickly can lead to undesirable effects like hypotension, cardiac arrhythmias, allergic reactions, and fluid overload.
- Thrombophlebitis: Inflammation of a vein, often with a blood clot, can occur due to frequent IV injections, improper technique, or certain medications.
- Circulatory Overload: Infusing too much fluid too quickly can overwhelm the circulatory system, leading to fluid buildup and strain on the heart and lungs.
- Embolism: A blood clot, air bubble, or foreign matter blocking a blood vessel can occur due to thrombophlebitis, improper IV line placement, or air entering the line.
- Shock: Severe allergic reactions, blood loss, or sepsis can lead to a life-threatening decrease in blood flow to vital organs.
- Infiltration/Extravasation: When IV fluids leak out of the vein into the surrounding tissues, it can cause pain, swelling, and tissue damage.
- Phlebitis: Inflammation of a vein without a clot, often caused by irritation from the IV catheter or medication.
- Air Embolism: Air entering the bloodstream through the IV line can travel to the heart or lungs, causing blockage and potentially leading to respiratory distress or cardiac arrest.
- Catheter-Related Bloodstream Infection (CRBSI): A serious complication where bacteria enter the bloodstream through the IV catheter, leading to fever, chills, and potentially sepsis.
- Nerve Damage: Incorrect placement of the IV catheter can damage nerves in the area, resulting in pain, numbness, or weakness.
- Hematoma: Bleeding into the surrounding tissues from the IV puncture site, appearing as a bruise.
- Phlebosclerosis: Hardening of the vein due to repeated IV punctures or irritation from the catheter.
Common Sites for Intramuscular Injections
- Gluteal Muscle: The outer upper quadrant of the buttock is the safest site, as it avoids the sciatic nerve.
- Thigh Muscles: The upper outer third of the thigh muscles.
- Deltoid Muscle: Used for small injections (up to 2 ml) if the patient has enough muscle mass, but this site should be avoided whenever possible.
COMPLICATIONS OF INTRAMUSCULAR INJECTIONS
1. Abscess Formation: This occurs when unsterile needles and syringes are used, or when oily substances are not injected deep enough. The injection site becomes inflamed and filled with pus.
- Prevention: Strict adherence to aseptic technique, proper needle selection, and injecting oily substances deep into the muscle tissue are crucial.
2. Nerve Injury: Incorrectly positioning the needle can damage nearby nerves, causing pain, numbness, weakness, or paralysis.
- Prevention: Thorough anatomical knowledge, correct landmark identification, and careful needle insertion are essential.
3. Tissue Damage/Necrosis: Injecting too much medication, using irritating substances, or repeated injections in the same site can lead to tissue damage and cell death.
- Prevention: Administering the correct dosage, choosing less irritating medications, and rotating injection sites regularly can minimize this risk.
4. Hematoma: A hematoma forms when blood leaks into the surrounding tissue after the injection, causing a bruise or swelling.
- Prevention: Applying pressure to the injection site after the injection can help prevent hematoma formation.
5. Pain and Discomfort: Intramuscular injections can be painful, especially if the medication is irritating or the injection technique is not correct.
- Prevention: Using proper injection technique, choosing a suitable needle size, and warming the medication to room temperature can reduce pain.
6. Allergic Reactions: Some individuals may have an allergic reaction to the medication or the ingredients in the solution.
- Prevention: Thorough patient history, allergy testing, and careful observation for signs of allergic reactions are crucial.
7. Injection into a Blood Vessel: The needle may unintentionally enter a blood vessel, leading to potential complications like drug overdose or embolism.
- Prevention: Aspirating (drawing back on the plunger) before injecting helps to ensure the needle is not in a blood vessel.
8. Delayed-Onset Muscle Soreness: Some medications can cause muscle soreness or stiffness that may not appear until several hours or days after the injection.
- Prevention: No specific prevention, but staying hydrated and avoiding strenuous activity after the injection may help.
9. Infection: Improper sterile technique can lead to infection at the injection site.
- Prevention: Strict adherence to aseptic technique is essential.
10. Air Embolism: Although rare, air can be injected into the bloodstream, leading to complications like respiratory distress or cardiac arrest.
- Prevention: Using proper technique to ensure no air is introduced into the syringe or needle.
Formula for Calculating the Drop Rate
To calculate the drop rate, use the following formula:

Example:
The doctor has prescribed 1000 mls of 5% dextrose infusion to run in 10 hours. How many drops per minute will you regulate if the infusion set has a drop factor of 20?

Thanks for the good summarized notes
Thanks for the precised notes
Thanks so summarized notes
We really appreciate u for your endless efforts in compiling of these precise and understandable notes . Personally am too grateful
Thanks you for the great work.
You make the world a better place by making things easier.
Really this can save someone
Thanks for the initiative
Thanks for the notes
Thanks for the good info. But of late they recommend that the blood is administered at its temperature from the fridge not warming it. Thanks
Thanks for this well eleborated notes..
Thanks but how can I access the revision questions
Thanks for the good work
Thx alot but formulate revision questions also..
Good resource for nurse
WITH LOVE JOY AND COMPASSION,I TAND HERE BY SAYING THAT THANK YOU SO MUCH FOR YOUR PRE_SIZED NOTES FOR THE BETTER LEARNING OF OUR BELOVED NURSES AND MIDWIVES IN OUR COUNTRY,C,CONTINENT THE WORLD AT LARGE
THANK YOU, YOURS
GODFEARING JB