

Antidepressants are a class of medications primarily used to treat clinical depression (major depressive disorder), anxiety disorders, chronic pain, and addiction. They are widely known as "mood elevators."
Historical Context: The first antidepressant drug to be discovered was a monoamine oxidase inhibitor by Crane (1957) and Kline (1958).
- Depression, or major depressive disorder (MDD), is a mood disorder characterized by feelings of extreme sadness, anhedonia (inability to feel pleasure), and hopelessness.
- A patient may experience depressive episodes that last for several days, weeks, or even months, significantly impairing daily functioning.
The core mechanism of most antidepressants relies on the Monoamine Hypothesis.
- Antidepressants act by preventing the re-uptake of key biogenic amines/neurotransmitters involved in mood regulation, specifically serotonin (5-HT) and noradrenaline (norepinephrine/NE).
- By inhibiting the reuptake pumps (transporters) on the pre-synaptic neuron, the rapid clearance of these neurotransmitters is prevented.
- This action builds up their quantities in the synaptic cleft to normal physiological levels, resulting in a good clinical therapeutic effect.
- Delayed Onset: Antidepressants commonly take 2 to 3 weeks before their clinical mood-elevating effects are fully realized. This delay is thought to be due to the time required for neuroplastic changes, up/down-regulation of pre-synaptic autoreceptors, and increased production of Brain-Derived Neurotrophic Factor (BDNF).
Antidepressants have a wide range of psychiatric and off-label medical indications:
- Psychotic depression (major depression with psychotic features).
- Agitated depression (depression accompanied by psychomotor agitation and restlessness).
- Neurotic depression (dysthymia or persistent depressive disorder).
- Reactive depression (adjustment disorder with depressed mood following a specific stressor).
- Atypical depression (characterized by mood reactivity, weight gain, hypersomnia, and leaden paralysis).
- Unipolar depression (standard major depressive episodes without mania).
- Suicidal tendencies (to improve underlying severe depressive symptoms, though close monitoring is required initially).
- N.B: Can also be used as an adjunct in the treatment of alcoholism.
- Specifically used for early morning awakening (a classic biological sign of severe depression).
- The patient wakes up feeling unrefreshed, lacks energy in the morning, and feels too weak to wake up. This phenomenon is known as diurnal variation of mood.
- Anorexia nervosa: Patients have an appetite but deliberately refuse to eat due to body image distortion.
- Bulimia nervosa: Characterized by episodes of excessive eating (bingeing) followed by compensatory behaviors (purging).
- Panic disorder (with or without agoraphobia).
- Agoraphobia (fear of places where escape might be difficult).
- Social phobia (Social Anxiety Disorder).
- School phobia (separation anxiety presenting as school refusal).
- Obsessive-Compulsive Disorder (OCD): With or without comorbid depression (requires higher doses of serotonergic drugs).
- Chronic body complaints: Somatic symptom disorders or chronic pain syndromes without physical pathology (e.g., fibromyalgia, neuropathy).
- Nocturnal enuresis (Bedwetting): If this follows no physical pathology, specific antidepressants (like Imipramine) can be used in small doses to contract the internal bladder sphincter.
- Migraine headache: Used for migraine prophylaxis (e.g., Amitriptyline).
- Attention Deficit Hyperactivity Disorder (ADD/ADHD): Used off-label when stimulants are ineffective or contraindicated.
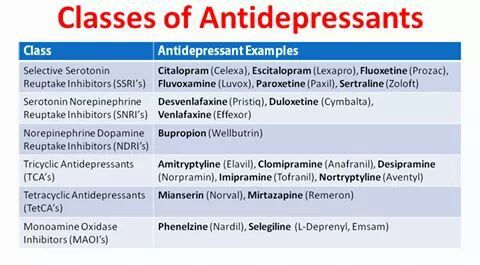
- Selective Serotonin Re-uptake Inhibitors (SSRIs)
- Tricyclic Antidepressants (TCAs)
- Tetracyclic Antidepressants (TetCAs / Atypicals)
- Monoamine Oxidase Inhibitors (MAOIs)
- Serotonin Norepinephrine Reuptake Inhibitors (SNRIs)
These are newer antidepressants which target a specific neurotransmitter transporter—the serotonin reuptake pump. They work by selectively increasing serotonin levels in the synaptic cleft without causing significant cholinergic, histaminergic, or adrenergic blockade. They are much safer in overdose and cause fewer side effects compared to older antidepressants (like TCAs).

- Has a very long half-life (up to 4-6 days, with an active metabolite, norfluoxetine, lasting up to 16 days). This long duration provides a "self-tapering" effect, significantly reducing the risk of discontinuation syndrome compared to other SSRIs.
- It is considered an "activating" SSRI due to its 5-HT2C antagonism, which can lead to increased energy, focus, and alertness early in treatment.
- Potent inhibitor of CYP2D6 and CYP3A4 enzymes, which necessitates careful monitoring for drug-drug interactions, especially with antipsychotics or TCAs.
- 20mg - 60mg, given once daily (o.d) in the morning ('mane').
- In cases of treatment-resistant depression or OCD, dosages may occasionally be titrated up to 80mg/day.
- A once-weekly 90mg delayed-release formulation is also available for maintenance therapy in stabilized patients.
- Obsessive-compulsive disorder (OCD) in both adult and pediatric populations.
- Major Depressive Disorder (MDD), notably the only SSRI FDA-approved for treating depression in children aged 8 and older.
- Premenstrual dysphoric disorder (PMDD), often marketed under the brand name Sarafem.
- Bulimia nervosa; it remains the only FDA-approved medication for the treatment of this specific eating disorder at higher doses (60mg).
- Panic disorder with or without agoraphobia.
- Nausea and GI distress are common during the initial weeks of therapy.
- Weight loss (initially), though long-term use can eventually lead to weight neutrality or slight gain.
- Agitation/nervousness and anxiety, particularly in the first few days of titration due to its stimulating properties.
- Dryness of the mouth (xerostomia) and constipation related to mild secondary effects.
- Insomnia and vivid dreams; patients are often advised to take the dose early to avoid sleep disruption.
- Headache, which is usually transient and resolves with continued use.
- Sexual dysfunction (anorgasmia/decreased libido/delayed ejaculation) which remains one of the most common reasons for long-term non-compliance.
- Increased risk of suicidal ideation in children, adolescents, and young adults (Black Box Warning).
- Hepatic/renal disease: Requires dosage adjustment or less frequent dosing due to the liver-dependent metabolism of the drug.
- Monoamine Oxidase Inhibitors (MAOIs): Requires a mandatory 5-week washout period after stopping Fluoxetine before starting an MAOI to avoid serotonin syndrome.
- Caution in Pregnancy: Though often used, it carries some risks such as persistent pulmonary hypertension of the newborn (PPHN) and requires risk/benefit analysis.
- History of Bipolar Disorder: May precipitate a switch into mania or hypomania (manic switch).
- Highly potent SSRI with a short half-life (approximately 21 hours), meaning there is no active metabolite to cushion the drop in blood levels.
- Slightly more anticholinergic (M1 receptor affinity) and sedating than other SSRIs, making it unique in the class for its calming effect.
- Known for causing severe withdrawal (discontinuation) syndrome—characterized by "brain zaps," dizziness, and irritability—if stopped abruptly.
- Strong inhibitor of CYP2D6, which can increase the plasma levels of many other cardiovascular and psychiatric medications.
- 20mg - 60mg, given once daily at night ('nocte') due to its sedating properties.
- Controlled-release (CR) versions (12.5mg to 75mg) are available to potentially mitigate gastrointestinal side effects.
- Doses for panic disorder and OCD typically trend toward the higher end of the spectrum (40-60mg).
- Major Depression, particularly when presenting with high levels of anxiety or insomnia.
- Generalized Anxiety Disorder (GAD) and Social phobia (Social Anxiety Disorder).
- OCD and Post-Traumatic Stress Disorder (PTSD).
- Panic disorder and Premenstrual Dysphoric Disorder (PMDD).
- Vasomotor symptoms (hot flashes) associated with menopause (low-dose formulation).
- Sedation and somnolence, which can be beneficial for anxious patients but problematic for daytime functioning.
- Dryness of mouth and constipation, more pronounced than other SSRIs due to anticholinergic activity.
- Marked weight gain; Paroxetine is generally associated with the highest risk of significant weight gain among SSRIs.
- Sexual dysfunction, including high rates of erectile dysfunction and ejaculatory delay.
- Sweating (diaphoresis) and asthenia (weakness/fatigue).
- Hepatic/renal disease: Clearance is decreased in patients with severe impairment.
- Pregnancy (FDA Category D): Specifically associated with an increased risk of fetal cardiac defects like ventricular septal defects (VSD) and atrial septal defects (ASD) during the first trimester.
- Concurrent use with Thioridazine or Pimozide due to the risk of QTc prolongation and arrhythmias.
- Abrupt cessation: Strongly discouraged to avoid the intense discontinuation syndrome.
- In addition to serotonin reuptake inhibition, it has mild dopamine reuptake inhibition (DRI), which may contribute to its efficacy in atypical depression and cognitive focus.
- Highly bound to plasma proteins (approx. 98%), which is a consideration for patients on other highly protein-bound drugs like Warfarin.
- Very safe for patients with a history of cardiac ischemia or recent Myocardial Infarction (the SADHEART trial confirmed its safety profile in cardiac patients).
- 50mg - 200mg/day.
- Usually started at 25mg or 50mg; increases are made in 50mg increments at weekly intervals.
- Absorption is significantly increased when taken with food (up to 30-40% increase in bioavailability).
- Post-Traumatic Stress Disorder (PTSD): It is considered a first-line agent.
- Obsessive-compulsive disorder (OCD) and Major Depression.
- Panic disorders and Social Anxiety Disorder.
- Premature ejaculation (off-label use of the sexual side effect to prolong latency).
- Premenstrual dysphoric disorder (PMDD): Can be dosed daily or only during the luteal phase.
- Prominent GI upset: Nausea and diarrhea are very common. It is often referred to clinically as "squirtraline" due to its tendency to cause loose stools compared to other SSRIs.
- Anorexia and transient weight loss at the start of treatment.
- Insomnia and tremors, likely linked to its mild dopaminergic activity.
- Sexual dysfunction, specifically delayed orgasm and decreased libido.
- Dizziness and fatigue.
- Hepatic/renal disease: Primary metabolism occurs in the liver; severe cirrhosis requires lower or less frequent doses.
- Concurrent use of MAOIs or Disulfiram (the oral liquid concentrate of Sertraline contains 12% alcohol).
- Cautious use in pregnancy: Generally considered one of the safer SSRIs during breastfeeding due to low levels of infant exposure.
- Seizure disorders: Like all antidepressants, it should be used with caution in patients with a low seizure threshold.
Other common SSRIs include Citalopram (Celexa - watch for dose-dependent QT prolongation, limit to 40mg/day or 20mg in elderly) and Escitalopram (Lexapro - the S-enantiomer of citalopram, highly selective, faster onset, and generally better tolerated with fewer drug interactions), and Fluvoxamine (Luvox - strictly approved for OCD; notable for potent CYP1A2 inhibition which interacts significantly with caffeine and theophylline).
TCAs are well absorbed by mouth and undergo significant first-pass metabolism in the liver. They act by increasing the availability of the biogenic amine neurotransmitters Noradrenaline (NE) and 5-Hydroxytryptamine (Serotonin/5-HT) in the synaptic cleft through blocking their re-uptake into the pre-synaptic neuron by inhibiting the SERT (serotonin transporter) and NET (norepinephrine transporter). In addition to their primary action, TCAs also act as antagonists at various other receptors including H1 histamine receptors (leading to sedation), alpha-1 adrenergic receptors (leading to orthostatic hypotension), and muscarinic acetylcholine receptors (causing anticholinergic effects). TCAs have a long half-life (ranging from 10 to 70 hours depending on the specific drug and individual metabolism); they are therapeutically effective if given once a day (usually at night). The onset of their antidepressant action is relatively slow and variable, with 2-4 weeks elapsing before any noticeable improvement in mood occurs, though side effects often appear immediately.
- It is a tertiary amine tricyclic with high sedating properties due to potent H1 receptor antagonism.
- Possesses some of the strongest anticholinergic (antimuscarinic) effects in the class, which can lead to significant blurred vision, urinary retention, and cognitive clouding in the elderly.
- Metabolized in the liver into Nortriptyline, which is itself an active antidepressant (a secondary amine).
- Usually started in smaller doses (e.g., 10-25mg) and gradually increased (titrated) to minimize the impact of side effects and allow the body to build tolerance.
- Given as a single dose at night to utilize its sedating effect for sleep and to ensure peak plasma levels occur while the patient is resting.
- 25mg - 75mg nocte for initial or mild cases.
- Maximum dose up to 200mg nocte in hospitalized or severely depressed patients; however, doses above 150mg require careful cardiac monitoring.
- Lower doses (10mg-50mg) are common for non-psychiatric indications.
- A very good antidepressant in agitated depression (depression with restlessness and anxiety) where its sedative properties provide immediate relief for insomnia.
- Heavily used off-label for chronic neuropathic pain (post-herpetic neuralgia, diabetic neuropathy).
- Effective for fibromyalgia and as a first-line agent for migraine prophylaxis.
- Treatment of persistent insomnia associated with mood disorders.
- It is a tertiary amine tricyclic with less sedating property compared to Amitriptyline, as it has slightly less affinity for the H1 receptor.
- It has a more balanced effect on serotonin and norepinephrine reuptake inhibition compared to its metabolite, Desipramine (which is highly selective for norepinephrine).
- Known for having a significant effect on the "internal biological clock" and autonomic nervous system.
- Same as amitriptyline (25mg - 200mg/day).
- Usually divided into smaller doses initially or given as a single nighttime dose if sedation occurs.
- Therapeutic drug monitoring (TDM) may be used to ensure blood levels are within the therapeutic window (150-300 ng/mL).
- A very good drug for depressive patients with psychomotor retardation (lethargy, slowed movement, and lack of energy) due to its slightly more "activating" profile relative to amitriptyline.
- Historically used for nocturnal enuresis (bedwetting) in children over 6 years old by increasing bladder capacity and altering sleep patterns.
- Highly effective in the treatment of Panic disorder with or without agoraphobia.
- Management of chronic pain syndromes and "masked" depression.
- Highly serotonergic compared to other TCAs, behaving more like an SSRI in its affinity for the serotonin transporter (SERT).
- It is the most potent inhibitor of serotonin reuptake among all the tricyclic antidepressants.
- Its metabolite, desmethylclomipramine, provides potent norepinephrine reuptake inhibition, giving it a dual-action (SNRI-like) profile.
- It is the gold-standard TCA mainly indicated in obsessive-compulsive neurosis (OCD) with an underlying depression; it was the first medication ever approved for OCD.
- Effective in treatment-resistant depression where SSRIs have failed.
- Used for cataplexy associated with narcolepsy.
- Treatment of premature ejaculation and certain phobic states.
- 50mg starting dose, increased gradually to avoid GI distress and seizure risk.
- Maintenance dose typically ranges from 100mg to 150mg, with a maximum of 250mg nocte.
- Requires caution at higher doses as it is associated with a higher risk of seizures than other antidepressants.
TCAs have a narrow therapeutic index. In overdose, they are cardiotoxic, causing widening of the QRS complex, arrhythmias (Torsades de pointes), and heart block. They also cause CNS toxicity (convulsions and coma). The "3 C's" of TCA overdose are Coma, Convulsions, and Cardiotoxicity.
These are closely related to TCAs but have a four-ring structure. They often possess different receptor affinities, making them useful for specific depressive presentations.
- Pharmacology: A strong norepinephrine reuptake inhibitor.
- Advantage: Works well on both agitated and retarded depression.
- Dosage: 50mg - 75mg b.d (twice daily) or t.d.s (three times a day) in 24 hours.
- Expanded Note: Maprotiline carries a higher risk of inducing seizures compared to other antidepressants, so dose escalation must be cautious. Another famous drug in this generalized atypical/tetracyclic class is Mirtazapine (Remeron), known for increasing appetite and causing heavy sedation.
Because these older drugs are "dirty drugs" (they bind to many unintended receptors), they have a broad and dangerous side-effect profile:
- Central Nervous System: Sedation, causes mania (switching from depression to bipolar mania in susceptible patients), blurred vision.
- Anti-histaminic (H1 blockade): Profound sedation and weight gain.
- Anti-cholinergic (M1 blockade): Dry mouth, dry eyes, constipation, urinary retention, blurred vision.
- Anti-adrenergic (Alpha-1 blockade): Mild to severe postural hypotension (orthostatic hypotension), sedation, sexual dysfunction.
- Cardiovascular (Na+ channel blockade): Tachycardia, cardiac arrhythmias, may cause heart block. This is what makes TCAs highly lethal in overdose.
- Others: Nausea & vomiting, bone marrow depression, urticaria (rash).
The earliest class of antidepressants. Currently, they are rarely used as first-line agents due to their gross side effects and dangerous food/drug interactions. They have largely been replaced by SSRIs and TCAs.
- Mechanism: They work by irreversibly (usually) inhibiting the enzyme monoamine oxidase, thereby increasing the concentration of stored monoamines in the presynaptic terminal, especially noradrenaline, dopamine, and serotonin.
- Indications: Depressive-neurosis, anxiety, phobic states, atypical depression, and severe depressive illness which has failed to respond to other therapies (Treatment-Resistant Depression).
- A hydrazine derivative that acts as a potent, irreversible, non-selective inhibitor of Monoamine Oxidase (MAO-A and MAO-B).
- By inhibiting MAO, it increases the concentrations of epinephrine, norepinephrine, serotonin, and dopamine throughout the central nervous system.
- It also has a unique effect on GABA-transaminase, which increases GABA levels in the brain, potentially contributing to its superior efficacy in treating anxiety.
- 15mg - 30mg bid / tds (twice or three times daily).
- Treatment usually begins at 15mg three times a day, increasing rapidly to at least 60mg per day to achieve effective MAO inhibition.
- Maximum dose 60mg - 90mg in 24 hours depending on clinical response and tolerability.
- "Atypical" depression, characterized by mood reactivity, oversleeping, and overeating.
- Severe anxiety states and Social Anxiety Disorder.
- Refractory Obsessive-compulsive disorder (OCD) and Panic Disorder where other treatments have failed.
- Significant weight gain and increased appetite.
- Orthostatic hypotension (dizziness upon standing), which can be severe in the elderly.
- Peripheral edema (fluid retention) and muscle tremors.
- Nervousness, insomnia, and sometimes daytime somnolence.
- Risk of "Hypertensive Crisis" if taken with tyramine-rich foods (the "cheese effect").
- Diabetes: Can alter hypoglycemic responses and insulin requirements.
- CVS disease: History of stroke or heart failure due to blood pressure fluctuations.
- Liver disease: Potential for hepatotoxicity as it is a hydrazine derivative.
- Pheochromocytoma or any catecholamine-secreting tumors.
- An irreversible, non-selective hydrazine MAOI similar in mechanism to phenelzine but generally considered to have a slightly cleaner side effect profile for some patients.
- Works by inhibiting the breakdown of monoamine neurotransmitters, thereby enhancing synaptic transmission.
- 20mg - 60mg in single or divided doses.
- Usually starts at 10mg twice daily, titrating up to a maximum of 60mg daily.
- Same as phenelzine, specifically indicated for patients who have not responded to SSRIs or TCAs.
- Particularly effective for depression with melancholic features or phobic symptoms.
- Weight loss (unlike phenelzine which often causes gain), though weight gain is still possible.
- Hypotension and drowsiness.
- Sexual dysfunction including impotence and anorgasmia.
- Paradoxical mania or hypomania in susceptible individuals.
- Jaundice and nausea, indicating the need for periodic liver function tests.
- Diabetes, CVS disease, and Liver disease.
- Avoid use with sympathomimetic drugs (like decongestants) or other antidepressants.
- A non-hydrazine MAOI with a chemical structure similar to amphetamine.
- It provides rapid MAO inhibition and has pronounced stimulating properties because it triggers the release of norepinephrine and dopamine.
- Unlike hydrazine MAOIs, it does not carry the same high risk of hepatotoxicity.
- 20mg - 40mg bid (usually taken morning and noon to avoid insomnia).
- Maximum dose can reach up to 60mg per day in specialized settings.
- Severe insomnia due to its stimulant-like structure; patients should avoid late-day dosing.
- Weight gain (but significantly less common than with phenelzine).
- Restlessness, agitation, and overstimulation.
- Postural hypotension and palpitations.
- Same as phenelzine, with additional caution in patients with a history of hyperthyroidism or agitation.
- Strict adherence to a low-tyramine diet is mandatory to prevent stroke or hypertensive crisis.
Mono-amine oxidase inhibitors interact lethally with certain foods and drugs.
The Hypertensive Crisis ("Cheese Reaction")
This is a life-threatening (fatal) spike in blood pressure. It is caused by the MAOI inhibiting the breakdown of Tyramine in the gut and liver. Tyramine enters the bloodstream, travels to sympathetic nerve terminals, and forces a massive release of stored noradrenaline.
- Foods to strictly avoid (High Tyramine): Aged cheese, yeast extracts, wine (especially Chianti/red wine), smoked fish, beans with broad pods (fava beans), avocado, and leftover food which is decomposing/fermenting.
- Interacting Drugs to avoid:
- Amphetamine (and other stimulants/decongestants)
- Ephedrine / Pseudoephedrine
- Barbiturates
- Phenytoin
- Tricyclic anti-depressants
- SSRIs and SNRIs: Combining MAOIs with serotonergic drugs causes fatal Serotonin Syndrome (hyperthermia, rigidity, myoclonus, coma). A washout period of at least 2 weeks (5 weeks for fluoxetine) is mandatory before switching.
Important Note on Duration of Therapy: Anti-depressants must be given to patients for at least 6 months after clinical improvement. For example, if a patient has been on treatment for 3 months and improves, the clinician must count 6 months ahead of continuation therapy without defaulting to prevent rapid relapse.
These newer agents work by affecting two chemical messengers (neurotransmitters) used to communicate between brain cells—serotonin and noradrenaline—hence regulating mood and relieving depression. They combine the dual-action efficacy of TCAs (affecting both pathways) with the safety and tolerability profile of SSRIs, as they lack the significant antihistamine and anticholinergic side effects of older drugs.
 <
<
- A potent inhibitor of neuronal serotonin and norepinephrine reuptake.
- It has low affinity for dopaminergic, adrenergic, cholinergic, and histaminergic receptors.
- The starting dose is 60mg, taken once a day.
- This can be increased up to 120mg, taken once a day for severe depression or chronic pain.
- Doses above 120mg are rarely more effective and significantly increase side effect burden.
- Major Depressive Disorder (MDD) and Generalized Anxiety Disorder (GAD).
- Nerve pain such as fibromyalgia, diabetic peripheral neuropathy, and chronic musculoskeletal pain.
- Used to treat stress-related emotional symptoms.
- Urinary incontinence in women (stress urinary incontinence) as it increases the tone of the external urethral sphincter.
- Difficulty sleeping (insomnia) or somnolence; headaches and feeling dizzy.
- Blurred vision and dry mouth (xerostomia).
- GI disturbances: constipation, diarrhea, and prominent nausea or vomiting.
- Sweating (diaphoresis) and tiredness/fatigue.
- Decreased appetite and weight loss.
- Sexual dysfunction: decreased libido, erectile dysfunction, or delayed orgasm.
- A bleeding disorder: Serotonin depletion in platelets can increase bleeding time.
- Diabetes: May affect glycemic control; requires careful monitoring.
- Epilepsy: Should only be taken if epilepsy is well controlled.
- Kidney/Liver disease: Duloxetine is hepatotoxic; it should not be prescribed to patients with chronic liver disease or heavy alcohol use.
- Uncontrolled Narrow-Angle Glaucoma: Can cause pupillary dilation (mydriasis).
- At lower doses (<150mg/day), it primarily blocks serotonin reuptake, acting much like an SSRI.
- At higher doses (>150mg/day), it robustly blocks noradrenaline reuptake, providing the full SNRI effect.
- At very high doses, it also provides weak dopamine reuptake inhibition.
- Severe or melancholic depression.
- Generalized Anxiety Disorder (GAD) and Social Anxiety Disorder.
- Panic Disorder and Post-traumatic Stress Disorder (PTSD).
- Similar to duloxetine but notorious for causing dose-dependent hypertension (systolic and diastolic) due to increased noradrenaline levels.
- Severe discontinuation syndrome: Stopping abruptly can cause "brain zaps," extreme vertigo, and flu-like symptoms.
- Increased sweating and potentially high heart rate (tachycardia).
- Desvenlafaxine (Pristiq): The active metabolite of venlafaxine. It bypasses the hepatic CYP2D6 metabolism pathway, making it a more predictable choice for "poor metabolizers" or patients on multiple medications.
- Milnacipran/Levomilnacipran: Other SNRIs that have a higher ratio of noradrenaline to serotonin inhibition compared to venlafaxine.
- Crane, G. E. (1957). Iproniazid (Marsilid) phosphate, a therapeutic agent for mental disorders and debilitating disease. Psychiatric Research Reports, 8, 142-152.
- Kline, N. S. (1958). Clinical experience with iproniazid (Marsilid). Journal of Clinical and Experimental Psychopathology, 19(2), 72-78.
- ABC News. (n.d.). Common antidepressants could fuel the rise of superbugs, study finds.
- MedWorks Media. (n.d.). Amitriptyline | Elavil Prescribing Information.
- InternationalPharmacy.com. (n.d.). Nardil Tabs (Phenelzine) Information.
- Tasnim Pharmaceutical Company. (n.d.). Duloxetine® 30 Product Monograph.
- Stahl, S. M. (2021). Stahl's Essential Psychopharmacology: Neuroscientific Basis and Practical Applications (5th ed.). Cambridge University Press. (Used for pharmacological expansions).
Mechanism of action for Tetracycline antidepressants
Tricyclic antidepressants (TCAs) work by inhibiting the reuptake of neurotransmitters such as serotonin and norepinephrine in the brain. This leads to increased levels of these neurotransmitters in the synaptic cleft, which helps to improve mood and alleviate depressive symptoms.
TCAs primarily block the reuptake pumps, or transporters, responsible for removing serotonin and norepinephrine from the synaptic cleft back into the presynaptic neuron. By blocking these transporters, TCAs increase the concentration of these neurotransmitters in the synapse, allowing for enhanced transmission of signals between neurons.
Additionally, TCAs also have antagonist effects on various receptors, including histamine receptors, alpha-adrenergic receptors, and muscarinic acetylcholine receptors. These receptor-blocking effects contribute to the side effects commonly associated with TCAs, such as sedation, dry mouth, constipation, and blurred vision.
Overall, the mechanism of action of TCAs involves both the inhibition of neurotransmitter reuptake and the modulation of various receptors, leading to increased levels of serotonin and norepinephrine in the brain, which helps to alleviate depressive symptoms.
Thanks