

Table of Contents
ToggleANTINEOPLASTIC AGENTS
Antineoplastic agents are a class of drugs designed to combat cancer by inhibiting the growth and proliferation of neoplastic cells (cancer cells). Also called Anticancer drugs.
The action of antineoplastic agents can be broadly categorized into two main mechanisms: affecting cell survival and enhancing the immune system’s ability to fight abnormal cells.
Common Terminology
- Alopecia: Hair loss, a common side effect due to the drug’s action on rapidly dividing cells.
- Angiogenesis: Formation of new blood vessels, which cancer cells induce to supply themselves with nutrients.
- Carcinoma: A type of cancer that starts in epithelial cells.
- Metastasis: The spread of cancer cells from the original site to other parts of the body.
- Neoplasm: An abnormal growth of tissue, which can be benign or malignant (cancerous).
- Sarcoma: A type of cancer that arises from connective tissues such as bone, muscle, and fat.
- Anaplasia: loss of organization and structure; property of cancer cells.
- Cancer: refers to a malignant neoplasm or new growth
Cancer can be divided into;
- Solid tumors
- Hematological
Solid Tumors; can further be differentiated into carcinomas, or tumors that originate in epithelial cells, and sarcomas, or tumors that originate in the mesenchyme and are made up of embryonic connective tissue cells.
Haematological Malignancies; involve blood forming organs of the body, the bone marrow, the lymphatic system. These malignancies alter the body’s ability to produce and regulate the cells found in the blood.
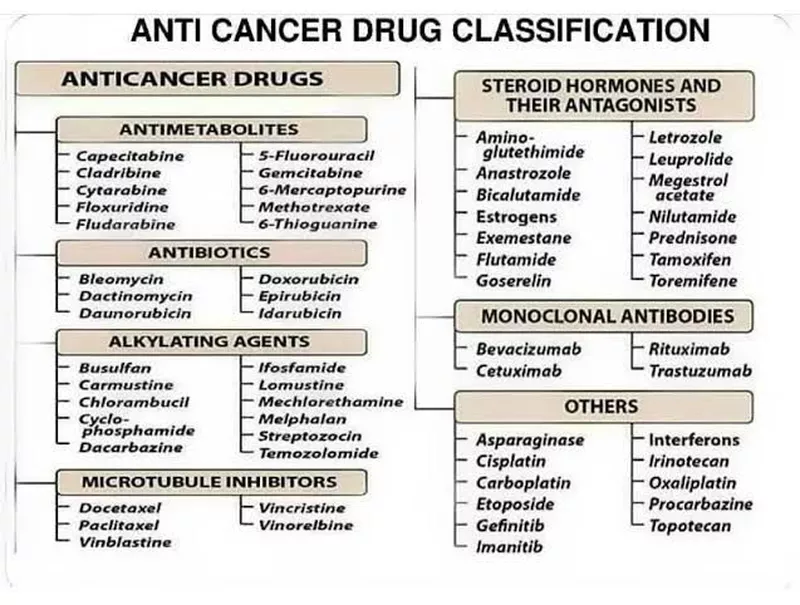
Classification of Antineoplastic Agents:
- Alkylating Agents: Interfere with DNA replication, most effective against slow-growing cancers.
- Antimetabolites: Resemble natural substances within the cell, disrupting DNA and RNA synthesis.
- Antineoplastic Antibiotics: Bind to DNA and prevent RNA synthesis, primarily affecting rapidly growing cells.
- Mitotic Inhibitors: Block cell division (mitosis), preventing the replication of cancer cells.
- Hormones and Hormone Modulators: Block or mimic hormones to inhibit the growth of hormone-sensitive tumors.
- Cancer Cell-Specific Agents: Target specific molecules involved in cancer cell growth and survival, minimizing damage to normal cells.
- Miscellaneous Antineoplastics: A diverse group with varying mechanisms of action, often used when other treatments are ineffective.
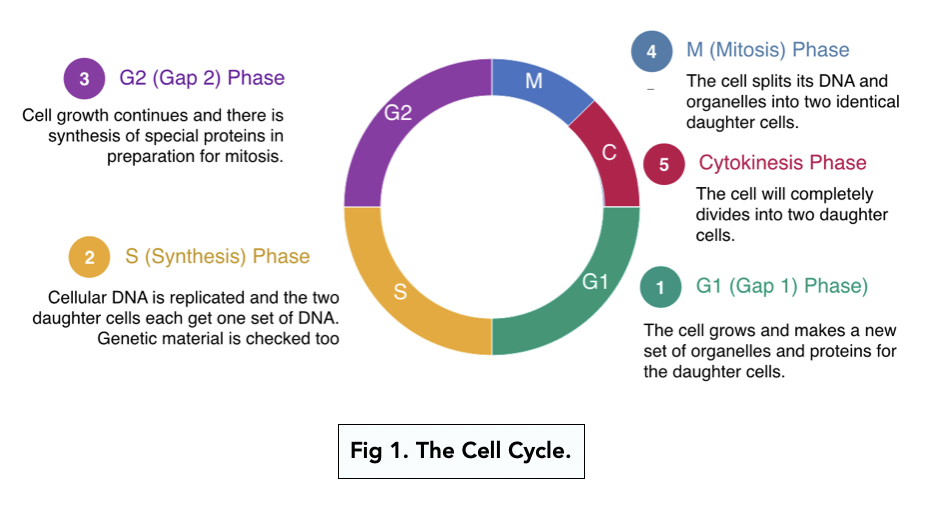
- Starts with G1 Phase: where the cell grows in size and releases enzymes for DNA replication. Cells may not progress hence remain at G0 phase.
- S Phase: Synthetic Phase: Where DNA replication occurs, cells make identical copies of their own chromosomes.
- G2 Phase: Check Point, When passed, they continue to grow and prepare themselves to divide.
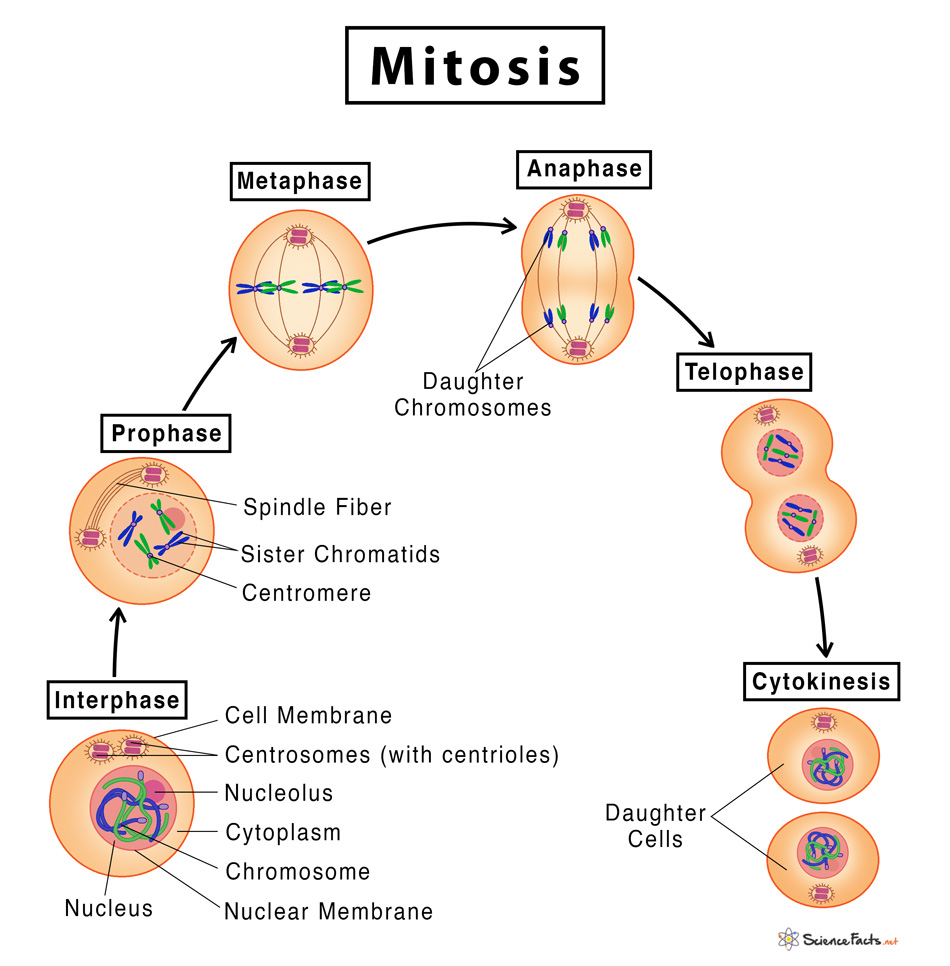
- Mitosis Phase: where cell division occurs
- Prophase: Chromosomes appear condensed and the nuclear envelope breaks down.
- Metaphase: Where microtubules in the center align,
- Anaphase: Chromosomes are separated
- Telophase: 2 daughter cells formed
- Cytokinesis: Either they become dormant(Gap 0) , or continue to G1 phase to create another cell division.
Types of Antineoplastic Drugs
Alkylating Agents/DNA Replication Inhibitors
Alkylating agents work by adding an alkyl group to the DNA, thereby preventing the DNA strands from uncoiling and replicating. This is particularly effective in treating slow-growing cancers.
Indications:
- Lymphomas
- Leukemias
- Myelomas
- Ovarian, testicular, and breast cancers
- Pancreatic cancer
- Pulmonary carcinoma (lung cancer)
- Rheumatoid arthritis
Contraindications:
- Pregnancy and lactation (due to severe effects on the fetus and neonate)
- Bone marrow suppression
- Renal and hepatic dysfunction
Adverse Effects:
- Gastrointestinal (GI): Nausea, vomiting, diarrhea, mucous membrane deterioration
- Genitourinary (GU): Renal toxicity, increased uric acid levels
- Hematological: Bone marrow suppression, leading to anemia, thrombocytopenia, and leukopenia
- Alopecia
Examples of Alkylating Agents:
Drug | Indications | Dosage |
Cyclophosphamide (Cytoxan, Neosar) | Lymphomas, Leukemias, Myelomas, Breast cancer | Induction: 40–50 mg/kg per day IV over 2–5 days; Maintenance: 1–5 mg/kg per day Orally/IV |
Busulfan (Busulfex, Myleran) | Chronic myelogenous leukemia (CML), Lymphomas | Induction: 4–8 mg/d Orally; Maintenance: 1–3 mg/d Orally |
Chlorambucil (Leukeran) | Hodgkin’s disease, Non-Hodgkin’s lymphoma | 0.1–0.2 mg/kg per day Orally for 3–6 weeks; Maintenance: 0.03–0.1 mg/kg per day Orally |
Antimetabolites
Antimetabolites mimic natural substances within the cell, interfering with DNA and RNA synthesis. These drugs are most effective against rapidly proliferating cells.
Indications:
- Leukemias
- Gastrointestinal cancers
- Breast, stomach, pancreas, and colon cancer
Contraindications:
- Pregnancy and lactation
- Bone marrow suppression
- Renal and hepatic dysfunction
- GI ulceration
Adverse Effects:
- CNS: Headache, drowsiness, dizziness
- Respiratory: Pulmonary toxicity, interstitial pneumonitis
- Hematological: Bone marrow suppression
- GI: Nausea, vomiting, diarrhea, hepatic toxicity
- GU: Renal toxicity
Examples of Antimetabolites:
Drug | Indications | Dosage |
Methotrexate (Rheumatrex, Trexall) | Leukemias, Rheumatoid arthritis | 15–30 mg Orally/IM depending on the disease being treated |
Fluorouracil (Adrucil, Carac) | Breast, stomach, colon cancer | 12 mg/kg per day IV on days 1–4, then 6 mg/kg IV on days 6, 8, 10, and 12 |
Antineoplastic Antibiotics
These drugs bind to DNA and inhibit RNA synthesis, primarily targeting rapidly dividing cells.
Indications:
- Testicular cancer
- Lymphomas
- Squamous cell carcinoma
- Choriocarcinoma
Contraindications:
- Pregnancy and lactation
- Bone marrow suppression
- Renal and hepatic dysfunction
- Pre-existing pulmonary or cardiac conditions
Adverse Effects:
- CNS: Headache, drowsiness, dizziness
- Respiratory: Pulmonary toxicity
- Hematological: Bone marrow suppression
- GI: Nausea, vomiting, hepatic toxicity
- GU: Renal toxicity
- Alopecia
Examples of Antineoplastic Antibiotics:
Drug | Indications | Dosage |
Bleomycin (Blenoxane) | Testicular cancer, Lymphoma | Test dose of 1-2 units given 2-4 hours before therapy; 0.25–0.5 units/kg IM, IV, or SC once/twice weekly |
Doxorubicin (Adriamycin, Doxil) | Breast cancer, Kaposi’s sarcoma | 60–75 mg/m2 as a single IV dose; repeat every 21 days |
Mitotic Inhibitors/Vinca Alkaloids
Mitotic inhibitors block cell division by inhibiting mitosis, specifically targeting the M phase of the cell cycle.
Indications:
- Leukemia
- Lymphomas (e.g., Hodgkin’s lymphoma)
- Kaposi’s sarcoma
- Testicular and breast cancer
Contraindications:
- Pregnancy and lactation
- Bone marrow suppression
- Renal and hepatic dysfunction
- GI ulceration
Adverse Effects:
- CNS: Headache, drowsiness, dizziness
- Hematological: Bone marrow suppression
- GI: Nausea, vomiting, mucous membrane deterioration
- GU: Renal toxicity
- Alopecia
- Neuropathy, stomatitis, constipation
Examples of Mitotic Inhibitors:
Drug | Indications | Dosage |
Vincristine (Oncovin, Vincasar) | Leukemia, Lymphoma | Adult: 1.4 mg/m2 IV at weekly intervals |
Vinblastine (Velban) | Hodgkin’s disease, Lymphoma | Adult: 3.7 mg/m2 IV once weekly; Pediatric: 2.5 mg/m2 IV once weekly |
Hormones and Hormone Modulators
Some cancers, particularly those involving the breast tissue, ovaries, uterus, prostate, and testes, are sensitive to estrogen stimulation. Estrogen-receptor sites on the tumor react with circulating estrogen, and this reaction stimulates the tumor cells to grow and divide
Hormones and hormone modulators block or interfere with these receptor sites to prevent growth of the cancer and cause cell death.
Some hormones are used to block the release of gonadotropic hormones in breast or prostate cancer if the tumors are responsive to gonadotropic hormones. Others may block androgen-receptor sites directly.
Indications:
- Breast cancer in postmenopausal women
- Prostate cancer
Contraindications and Cautions
- Known allergy to drug: Prevent hypersensitivity reactions
- Hypercalcemia: Contraindication to the use of toremifene because the drug can increase serum calcium
- Pregnancy and lactation: Severe effects on the fetus and neonate
- Bone marrow suppression: Index of re-dosing and dosing levels
- Renal and hepatic dysfunction: Interfere with drug metabolism and excretion
- Known GI ulceration or ulcerative diseases: Can be exacerbated by the effects of the drug.
Adverse Effects:
- Menopausal symptoms: Hot flashes, vaginal dryness, mood changes
- Hematological: Bone marrow suppression
- GI: Hepatic toxicity
- GU: Renal toxicity
- Hypercalcemia
Examples of Hormones and Hormone Modulators:
Drug | Indications | Dosage |
Tamoxifen (Nolvadex) | Breast cancer | 20–40 mg Orally per day |
Anastrozole (Arimidex) | Breast cancer in postmenopausal women | 1 mg Orally per day |
Quick Quiz
Anticancer Drugs Quiz
Pharmacology - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
Anticancer Drugs Quiz
Pharmacology
Preparing questions...
Choose your answer and keep your streak alive.
Great effort.
Here is your quick performance summary.
Incase You Needd Detailed, 👇👇👇👇👇
Antineoplastic agents are a class of drugs designed to combat cancer by inhibiting the growth and proliferation of neoplastic cells (cancer cells). They are also commonly referred to as Anticancer drugs or Chemotherapy.
The action of antineoplastic agents can be broadly categorized into two main mechanisms: affecting cell survival (cytotoxicity) and enhancing the immune system’s ability to fight abnormal cells (immunotherapy/targeted therapy).
- Before 1940: No effective treatment available for systemic cancers.
- Before 1955: Surgery was the primary and only definitive treatment.
- 1955–1965: Radiotherapy became widely established.
- After 1965: The advent and widespread use of systemic Chemotherapy.
- Modern Era: Introduction of Immunotherapy and Gene Therapy, revolutionizing targeted cancer treatment.
| Cell Cycle Phase | Cell Cycle Specific (CCS) Drugs | Cell Cycle Non-Specific (CCNS) Drugs |
|---|---|---|
| G1 - S Phase | Etoposide |
These agents affect cells across all phases: ➔ Platinum compounds (Cisplatin, Carboplatin) ➔ Alkylating agents (Cyclophosphamide, Busulfan, Nitrosoureas) ➔ Antibiotics (Anthracyclines, Dactinomycin, Mitomycin) ➔ Camptothecins |
| S Phase | Antimetabolites (Methotrexate, 5-FU, Cytarabine, 6-MP) | |
| G2 - M Phase | Bleomycin, Etoposide | |
| M Phase (Mitosis) | Vinca alkaloids, Taxanes, Ixabepilone, Estramustine |
- Cure or induce prolonged "remission": Macroscopic and microscopic features of the cancer disappear entirely. Highly achievable in: Acute Lymphoblastic Leukaemia (ALL), Wilm's tumor, Ewing's sarcoma, Hodgkin's lymphoma (in children), testicular teratoma, and choriocarcinoma.
- Palliation: Aimed at the shrinkage of an evident tumor, alleviation of symptoms, and prolongation of life rather than absolute cure. Targeted for: Breast cancer, ovarian cancer, endometrial carcinoma, CLL, CML, Small cell lung cancer (SCLC), and Non-Hodgkin lymphoma.
- Insensitive Tumors: These are less sensitive to chemotherapy, but life may still be prolonged. Includes: Cancer of the esophagus, cancer of the stomach, squamous cell carcinoma of the lung, melanoma, pancreatic cancer, myeloma, and colorectal cancer.
- Adjuvant Therapy: Used routinely now for "mopping up" residual cancer cells, including micrometastases, after surgery or radiation. Mainly utilized in solid tumors.
- It is analogous to Bacterial chemotherapy but with critical differences:
- Selectivity of drugs is highly limited (they attack normal host cells as well).
- No or less defense mechanism (the host immune system does not recognize cancer as readily as bacteria; cytokines are used as adjuvants now to boost this).
- The goal is to kill all malignant cells to stop progeny.
- Tumors contain subpopulations of cells that differ in their rate of proliferation and susceptibility to chemotherapy.
- Total Tumor Cell Kill via COMBINATION CHEMOTHERAPY: Formerly, single drugs were used; now, 2-5 drugs are used in intermittent pulses.
- Utilizes drugs which are effective when used alone.
- Combines drugs with different mechanisms of action.
- Combines drugs with differing toxicities (and different mechanisms of toxicities) to prevent overlapping fatal side effects (e.g., combining bone marrow-sparing Bleomycin with a myelosuppressive agent).
- Utilizes synergistic biochemical interactions.
- Applies an optimal schedule determined by trial and error, relying heavily on cell cycle specificity.
- Intrinsic Resistance: Tumors naturally possess primary resistance without prior exposure. Examples: Malignant melanoma, renal cell cancer, and brain cancer.
- Acquired Resistance: Develops after initial exposure.
- Single drug resistance: Change in the genetic apparatus, amplification, or increased expression of one or more specific genes targeted by the drug.
- Multidrug resistance (MDR): Resistance to a wide variety of drugs after exposure to a single variety. Often due to increased expression of a normal gene (the MDR1 gene) which codes for a cell surface glycoprotein (P-glycoprotein) involved in active drug efflux (pumping the drug out of the cell).
Chemotherapy is harmful to normal tissues because it has a steep dose-response curve and a low therapeutic index. It is particularly harmful to rapidly multiplying normal tissues (GI mucosa, Bone Marrow, Reticuloendothelial [RE] system, gonads, and hair cells). Effects occur in a dose-dependent manner.
- Bone Marrow Depression (BMD): Leukopenia, thrombocytopenia, anemia. This is the primary dose-limiting toxicity for most treatments.
- Buccal Mucosa Erosion: High epithelial turnover leads to stomatitis, severe mucositis, and bleeding gums.
- Gastrointestinal (GIT): Diarrhea, shedding of mucosa, hemorrhage. Nausea and vomiting are severe due to direct stimulation of the Chemoreceptor Trigger Zone (CTZ).
- Skin: Alopecia (hair loss).
- Gonads: Oligospermia, impotence, amenorrhoea, and permanent infertility.
- Lymphoreticular System: Lymphocytopenia and inhibition of lymphocyte function, leading to a loss of host defense mechanisms and extreme susceptibility to infections.
- Other systemic: Carcinogenicity (secondary tumors), Teratogenicity, and Hyperuricemia (due to rapid tumor cell lysis releasing purines).
| Drug | Distinctive Toxicity |
|---|---|
| Cyclophosphamide | Alopecia, Hemorrhagic cystitis, SIADH (Syndrome of Inappropriate Antidiuretic Hormone). |
| Ifosfamide | Hemorrhagic cystitis, SIADH. |
| Busulfan | Pulmonary fibrosis ("Busulfan lung"), Hyperpigmentation, Adrenal insufficiency, Tonic-clonic seizures. |
| Procarbazine | Secondary leukemias, Disulfiram-like reaction (with alcohol), behavioral changes, CNS depression. |
| Cisplatin | Severe Emesis, Nephrotoxicity, Peripheral sensory neuropathy, Ototoxicity (deafness). |
Toxicities are countered via intermittent therapy (giving normal cells time to recover) and specific pharmacological rescue agents:
| Drug (Rescue/Preventive Agent) | Mechanism of Action | Indications / Used For |
|---|---|---|
| Allopurinol | Inhibits xanthine oxidase. | Prevents hyperuricemia from massive tumor lysis syndrome. |
| Rasburicase | Recombinant urate oxidase (converts uric acid to soluble allantoin). | Prevents hyperuricemia from rapid tumor lysis. |
| Mesna (Sodium-2-mercaptoethane sulfonate) | Neutralizing agent (binds toxic metabolite acrolein). | Prevents hemorrhagic cystitis due to Ifosfamide and high-dose Cyclophosphamide. |
| Leucovorin (Folinic Acid) | Repletes Tetrahydrofolic acid directly. | "Leucovorin Rescue" after high-dose Methotrexate to save bone marrow and GIT mucosa. |
| Amifostine | Scavenges free radicals. | Prevents radiation-induced xerostomia and Cisplatin-induced nephrotoxicity. |
| Dexrazoxane | Iron chelator. | Prevents cardiotoxicity due to Anthracyclines (Doxorubicin, Daunorubicin). |
| Palifermin | Keratinocyte growth factor. | Prevents severe mucositis following heavy chemotherapy. |
| Pilocarpine | Cholinergic agonist. | Treats radiation-induced xerostomia (dry mouth). |
| Pamidronate / Zoledronate | Bisphosphonates. | Treats hypercalcemia of malignancy and bone metastases. |
| Epoetin alpha / Darbepoetin | Recombinant Erythropoietin. | Treats chemotherapy-induced anemia. |
| Filgrastim / Peg-filgrastim | G-CSF (Granulocyte Colony-Stimulating Factor). | Febrile neutropenia prophylaxis; speeds recovery of granulocytopenia. |
| Sargramostim | GM-CSF (Granulocyte-Macrophage CSF). | Myeloid reconstitution. |
| Oprelvekin | IL-11 (Interleukin-11). | Treats severe chemotherapy-induced thrombocytopenia. |
| Ondansetron / Granisetron / Palonosetron | 5-HT3 antagonists. | Prevents acute nausea and vomiting. |
| Aprepitant | NK-1 (Neurokinin-1) receptor antagonist. | Prevents Cisplatin-induced delayed vomiting. |
Classification is based on chemical structure, biochemical mechanism of action (blocking nucleic acid synthesis, interfering with DNA structure, blocking RNA/protein synthesis, influencing hormones), and cell cycle phase specificity.
- Mechanism of Action: They act by binding irreversibly to nucleic acids (DNA). Nitrogen mustards inhibit cell reproduction by adding an alkyl group. Bifunctional alkylating agents cause intrastrand linking and cross-linking of the DNA double helix (sugar-phosphate backbone).
- After alkylation, DNA is unable to replicate and cannot synthesize proteins or essential cell metabolites. Consequently, cell reproduction is inhibited, metabolic functions fail, and the cell eventually dies.
- Nitrogen Mustards: Mechlorethamine, Cyclophosphamide, Ifosfamide, Melphalan, Chlorambucil.
- Mechlorethamine: The first alkylating agent employed clinically. Bifunctional (crosslinks DNA). Extremely unstable and is inactivated within a few minutes following administration, thus given IV. Used in MOPP regimen for Hodgkin's disease. Highly vesicant (severe local toxicity on extravasation). ADRs: Severe vomiting, myelosuppression.
- Cyclophosphamide: A prodrug transformed into active aldophosphamide and phosphoramide mustard in the liver. Given orally or IV. Used for ALL, NHL, Polycythemia Vera, Hodgkin's lymphoma, breast and ovary cancers. Causes hemorrhagic cystitis (due to acrolein).
- Ifosfamide: Has a longer half-life, used mainly for testicular tumors. Also causes hemorrhagic cystitis.
- Chlorambucil: Orally active against lymphoid tissues. Preferred for CLL, Polycythemia Vera, and NHL.
- Melphalan: Oral agent used for Multiple Myeloma.
- Alkyl Sulfonates:
- Busulfan: Orally active. Great effect for Chronic Granulocytic/Myelogenous Leukemia (CML). Delayed toxicities: Pulmonary infiltrates/fibrosis ("Busulfan lung"), tonic-clonic seizures in epileptics, skin pigmentation, adrenal insufficiency.
- Nitrosoureas:
- Carmustine (BCNU) & Lomustine (CCNU): Bifunctional; active against broad spectrums of neoplastic disease. They inhibit synthesis of both DNA and RNA, as well as proteins. These drugs are highly lipophilic, easily crossing the blood-brain-barrier (BBB), making them excellent for primary and metastatic brain tumors. Also used for Hodgkin's, melanoma, and GI adenocarcinomas.
- Major Toxicity: Highly mutagenic/carcinogenic. Delayed bone marrow depression (prolonged leukopenia/thrombocytopenia), and pulmonary fibrosis.
- Platinum Coordination Compounds:
- Cisplatin: Forms crosslinks within DNA strands. Very powerful IV agent against Testicular cancer, ovary, bladder, head, and neck carcinomas. Toxicity is severe: Renal tubular damage (minimized via massive hydration + amifostine), Ototoxicity, peripheral neuropathy, and VERY SEVERE vomiting (treated with Ondansetron/Aprepitant).
- Carboplatin: A derivative of cisplatin with significantly less nephrotoxicity, neurotoxicity, and ototoxicity (but higher myelosuppression).
These are structural analogues of essential metabolites that interfere with DNA/RNA synthesis (block nucleic acid biosynthesis). Myelosuppression is the primary dose-limiting toxicity.
- Methotrexate (MTX): Structure is similar to folic acid. It actively transports into mammalian cells and competitively inhibits dihydrofolate reductase (DHFR), the enzyme that normally converts dietary folate to the tetrahydrofolate required for thymidine and purine synthesis.
- Kinetics & Indications: Orally, IM, IV, and intrathecally (for CSF entry). Used for ALL, Breast cancer, Tumors of head/neck, Meningeal metastases. It was the first demonstration of curative chemotherapy for Choriocarcinoma.
- Leucovorin (Folinic acid) Rescue: Administered as part of high-dose MTX therapy. Leucovorin is directly converted to tetrahydrofolic acid (producing DNA/cellular protein) in spite of the presence of MTX, rescuing bone marrow and GIT mucosal cells from lethal toxicity.
- 5-Fluorouracil (5-FU): Analogue of thymine. Converted to 5-fluoro-2-deoxy-uridine monophosphate (5-FdUMP), which irreversibly inhibits thymidylate synthase. This blocks the conversion of deoxyuridylic acid to deoxythymidylic acid, causing failure of DNA synthesis. Used for solid tumors (breast, colorectal, gastric, head/neck). Toxicity: Hand and foot syndrome, severe oral/GI ulceration.
- Cytarabine: Inhibits DNA polymerase. Used IV for Acute Myeloid Leukemia (AML). Delayed toxicity includes cerebellar ataxia (neurotoxicity).
- 6-Mercaptopurine (6-MP) & 6-Thioguanine (6-TG): Inhibit purine ring biosynthesis and nucleotide interconversions. 6-MP is used for childhood ALL maintenance and remission, and in combination with MTX for choriocarcinoma.
- Important Interaction: 6-MP is metabolized by xanthine oxidase (which is inhibited by Allopurinol). If a patient is taking Allopurinol for hyperuricemia, the dose of 6-MP must be adjusted to ½ or ¼ to prevent fatal bone marrow toxicity. Well tolerated long term but causes mild hepatotoxicity.
- Hydroxyurea: Inhibits ribonucleotide reductase. Used orally for CML, AML (blast crisis), and Polycythemia vera.
- Anthracyclines (Doxorubicin, Daunorubicin): Insert themselves into DNA causing breaks. They activate Topoisomerase II, causing DNA strand breaks, and generate excess free radicals (superoxide) causing DNA damage.
- Unique Toxicity: Known to irreversibly damage cardiac cells (Cardiomyopathy). Prevented with Dexrazoxane.
- Uses: Doxorubicin (Breast, ovary, lung, prostate, ALL, sarcomas, neuroblastoma). Daunorubicin (ALL, AML).
- Resistance: Develops due to increased efflux of drug via P-glycoprotein.
- Bleomycin: Used for Carcinoma testis, malignant effusions, Hodgkin's. Toxicity: Pulmonary fibrosis, stomatitis, oedema of hands. Causes minimal myelosuppression (alopecia common).
- Dactinomycin (Actinomycin D): Used for Wilm’s tumour.
- Mitomycin C: Carcinoma stomach. Causes severe thrombocytopenia and leukopenia.
- Streptozotocin: Targeted for Insulinoma (pancreatic islet cell tumors). Toxicity: Renal damage, hypoglycemia, nephrogenic diabetes insipidus.
- Vinca Alkaloids (Vincristine, Vinblastine, Vinorelbine): Bind tubulin, destroy the spindle apparatus to produce mitotic arrest (M phase).
- Vincristine: ALL, NHL. Toxicity: Peripheral neuritis, alopecia, BMD.
- Vinblastine: Hodgkin's Disease. Toxicity: Loss of reflexes, BMD.
- Vinorelbine: Carcinoma lung. Toxicity: Paresthesia, hyporeflexia, fatigue.
- Taxanes (Paclitaxel, Docetaxel): Stabilize microtubules, preventing disassembly.
- Paclitaxel: Carcinoma breast, ovary. Toxicity: Peripheral neuritis, BMD.
- Docetaxel: Advanced breast cancer. Toxicity: Fluid retention, neurotoxicity, neutropenia.
- Etoposide: A podophyllotoxin (toxin found in the mandrake root). Inhibits the enzyme Topoisomerase II, causing breaks in DNA inside cancer cells, preventing them from dividing. Useful for Testicular cancer and Small Cell Lung Cancer (SCLC). Side effects: Vomiting, alopecia, bone marrow suppression.
- Camptothecin Analogues (Irinotecan, Topotecan): Inhibit Topoisomerase I.
- L-Asparaginase: Depletes the amino acid asparagine, inhibiting protein synthesis. Used IV for ALL in children. Toxicity: Hepatotoxicity, mental depression, pancreatitis.
- Mitotane: Used for Adrenocortical carcinoma. Toxicity: Adrenal insufficiency, lethargy, diarrhea.
Influence hormone homeostasis in hormone-sensitive tumors.
| Agent | Cancers Where Preferred | Delayed Toxicity / Comments |
|---|---|---|
| Corticosteroids (Hydrocortisone, Prednisone) | ALL, CLL, NHL, Hodgkin's, Multiple myeloma | Fluid retention, hypertension, diabetes mellitus, susceptibility to infection, moon face. |
| Androgens (Testosterone) | Premenopausal breast cancer (estrogen receptor positive) | Fluid retention, masculinization. |
| Oestrogens (Diethylstilboestrol, Ethinyloestradiol) | Carcinoma prostate, Postmenopausal breast cancer (ER negative) | Feminization in males, fluid retention. |
| Progestins (Hydroxyprogesterone, Medroxyprogesterone) | Carcinoma endometrium | None significant. |
| Antiandrogens (Flutamide, Bicalutamide) | Carcinoma prostate | None significant. |
| Antiestrogens (Tamoxifen - SERM) | Carcinoma breast (early stage, metastatic after surgery) | Risk of endometrial proliferation/cancer. |
| GnRH Agonists (Goserelin, Leuprolide) | Carcinoma prostate | Medical castration effect. |
| Aromatase Inhibitors (Letrozole, Anastrozole, Aminoglutethimide) | Metastatic breast cancer (postmenopausal) | Osteoporosis. |
| Peptide Hormone Inhibitors (Octreotide) | Carcinoid tumour | Controls severe carcinoid syndrome symptoms. |
| Drug | Inhibits TK activated by: | Indication |
|---|---|---|
| Axitinib / Pazopanib | VEGFR - 1,2,3 / abl-bcr | Advanced renal cell carcinoma |
| Imatinib | Abl-bcr (Philadelphia chromosome), c-KIT | CML, GIST (Gastrointestinal Stromal Tumor) |
| Bosutinib / Dasatinib / Nilotinib | Abl-bcr, src, VEGFR | CML (often for Imatinib-resistant cases) |
| Crizotinib | c-MET, ALK | Non-small cell lung carcinoma (ALK-positive) |
| Cabozantinib / Vandetanib | c-MET, VEGFR-2, EGFR | Medullary carcinoma thyroid |
| Erlotinib / Gefitinib | EGFR, abl-bcr, PDGF | Non-small cell lung carcinoma, Pancreatic carcinoma |
| Lapatinib | HER-2/neu, erb-B2, abl-bcr | Breast carcinoma (HER2 positive) |
| Regorafenib | VDGFR2, TIE2 | Colorectal carcinoma, GIST |
| Ruxolitinib / Tofacitinib | JAK 1,2 | Myelofibrosis / Rheumatoid arthritis |
| Sorafenib / Sunitinib | VEGFR, PDGFR, RAF, c-KIT, RET | Renal cell carcinoma, Hepatocellular carcinoma, Pancreatic neuroendocrine, GIST |
| Vemurafenib | BRAF | Malignant melanoma (BRAF V600E positive) |
| Monoclonal Antibody | Targeted Against | Indication | Comments / Toxicities |
|---|---|---|---|
| Rituximab | CD-20 | Non-Hodgkin lymphoma, CLL | Infusion reactions common. |
| Alemtuzumab | CD-52 | Low grade lymphomas and CLL | Profound immunosuppression. |
| Trastuzumab | HER 2/neu | Breast Carcinoma (metastatic) | Can cause severe cardiotoxicity / cardiac failure. |
| Cetuximab / Panitumumab | EGFR | EGFR-positive metastatic colorectal carcinoma | Causes rash, Hypomagnesemia, and Interstitial lung disease. |
| Bevacizumab | VEGF (Vascular Endothelial Growth Factor) | Metastatic colorectal carcinoma | Combined with 5-FU. Inhibits angiogenesis. |
| Gemtuzumab | CD-33 | CD-33 Positive AML | Linked to calicheamicin (antibody-drug conjugate). |
| Tositumomab (I-131) / Ibritumomab (Y-90) | CD-20 | Relapsed lymphomas | Conjugated with radioisotopes for targeted radiation. |
| Denileukin diftitox | IL-2 receptor | Recurrent cutaneous T-cell lymphoma | Recombinant IL-2 plus diphtheria toxin. |
Modern oncology relies heavily on standardized, combination protocols based on extensive clinical trials.
| Diagnosis | Treatment of Choice (Regimen) |
|---|---|
| Acute Lymphocytic Leukaemia (ALL) | Induction: Vincristine + Prednisolone + Daunorubicin + Asparaginase + Intrathecal Methotrexate. Maintenance: Methotrexate + 6-Mercaptopurine + Cyclophosphamide. Consolidation: Hyper-CVAD alternated with Cytarabine+Methotrexate. |
| Acute Myeloid Leukaemia (AML) | Cytarabine + Daunorubicin/Idarubicin. |
| Chronic Myelogenous Leukaemia (CML) | Imatinib (Busulfan or Interferon as alternatives). Bone marrow transplant in selected patients. |
| Chronic Lymphocytic Leukaemia (CLL) | FCR (Fludarabine, Cyclophosphamide, Rituximab) or Fludarabine/Chlorambucil+Prednisone alone. |
| Hairy cell leukemia | Cladribine. |
| Hodgkin's disease | Stage I/II: Radiotherapy. Stage III/IV: ABVD (Doxorubicin [Adriamycin], Bleomycin, Vinblastine, Dacarbazine). |
| Non-Hodgkin lymphoma | CHOP-R (Cyclophosphamide, Doxorubicin, Vincristine, Prednisolone + Rituximab). |
| Multiple Myeloma | Bortezomib + Dexamethasone + Lenalidomide (or Melphalan + Prednisone). |
| Waldenstrom macroglobulinemia | FCR (Fludarabine, Cyclophosphamide, Rituximab). |
| Polycythemia vera | Hydroxyurea (or Busulfan/Chlorambucil). |
| Choriocarcinoma | Methotrexate + folic acid OR Cisplatin + Etoposide. |
| Carcinoma testis | Bleomycin + Cisplatin + Etoposide (BEP regimen). |
| Wilm's tumour | Surgery + radiotherapy followed by Vincristine + Dactinomycin. |
| Non-small cell lung cancer | Cisplatin + Vinorelbine ± Bevacizumab. |
| Small cell lung cancer | Cisplatin + Etoposide. |
| Mesothelioma | Cisplatin + Pemetrexed. |
| Head and neck cancer | Cisplatin + 5-FU. |
| Carcinoma breast stage 1 | Tamoxifen after breast surgery. |
| Carcinoma breast stage II to IV | Cyclophosphamide + Methotrexate + 5-FU (CMF) OR Trastuzumab + Prednisone + Antiestrogen. |
| Carcinoma ovary | Cisplatin/Carboplatin + Paclitaxel + Interferon. |
| Carcinoma prostate | GnRH agonist OR Oestrogen + Androgen antagonist (Flutamide). |
| Melanoma | Dacarbazine, Cisplatin, Interferon. |
| Carcinoma adrenal gland | Mitotane. |
| Carcinoid tumour | Doxorubicin + Cyclophosphamide OR 5-FU + Octreotide. |
- Contraindications Check: Assess for drug allergies, severe hepatorenal impairment, pre-existing bone marrow suppression, and verify pregnancy/lactation status (ensure barrier contraception is utilized by women of childbearing age).
- Baseline Physical Assessment: Check orientation, reflexes, vital signs, bowel sounds, and oral mucosa to establish baseline data before therapy begins.
- Laboratory Monitoring:
- CBC with differential: Crucial to identify bone marrow suppression (leukopenia, neutropenia, thrombocytopenia, anemia). Calculates the Absolute Neutrophil Count (ANC).
- Renal/Hepatic panels (BUN, Creatinine, AST, ALT, Bilirubin): To determine the need for dose adjustments and identify toxicities.
- Uric Acid: Monitor for Tumor Lysis Syndrome (prophylactic Allopurinol or Rasburicase may be needed).
| No. | Nursing Diagnosis | Interventions & Rationale |
|---|---|---|
| 1 | Risk for Infection related to chemotherapy-induced leukopenia and immunosuppression. |
|
| 2 | Imbalanced Nutrition: Less than body requirements related to severe nausea, vomiting (CTZ stimulation), and stomatitis/mucositis. |
|
| 3 | Risk for Bleeding related to chemotherapy-induced thrombocytopenia. |
|
| 4 | Disturbed Body Image related to alopecia and physical changes from targeted therapies (e.g., severe acneiform rash). |
|
| 5 | Risk for Impaired Tissue Integrity (Vesicant Toxicity) related to extravasation of alkylating agents or antibiotics (e.g., Mechlorethamine, Doxorubicin, Vincristine). |
|
- Presentation Slides: Treatment options of cancer / Anticancer drugs (Slides 57 pages detailing Cell Cycle, Alkylating Agents, Antimetabolites, Antibiotics, Targeted Therapies, Toxicities, and Therapy of Choice).
- Brunton, L. L., Hilal-Dandan, R., & Knollmann, B. C. (2017). Goodman & Gilman's The Pharmacological Basis of Therapeutics (13th ed.). McGraw-Hill Education.
- Katzung, B. G. (2017). Basic & Clinical Pharmacology (14th ed.). McGraw-Hill Education.
- Nursing considerations adapted from Oncology Nursing Society (ONS) guidelines for safe handling and administration of chemotherapy.
Quick Quiz
Anticancer Drugs Quiz
Pharmacology - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
Anticancer Drugs Quiz
Pharmacology
Preparing questions...
Choose your answer and keep your streak alive.
Great effort.
Here is your quick performance summary.
Quizze questions
It’s a great work and am able to understand better. Thanks 🙏