Cell Injury & Death
Cell Injury, Death, and Adaptation
By the end of this comprehensive guide, you will be deeply conversant with:
- The different cellular responses to injury and the specific agents that cause them.
- The various types and stages of cell injury (Reversible vs. Irreversible).
- The underlying biochemical mechanisms and distinct morphological changes observed in cell injury.
- The defining characteristics of Cell Death (Necrosis vs. Apoptosis) and other emerging pathways.
- The different forms of cellular adaptations (Hypertrophy, Hyperplasia, Atrophy, Metaplasia) and cellular depositions, along with their clinicopathological relevance.
Cellular Responses to Stress
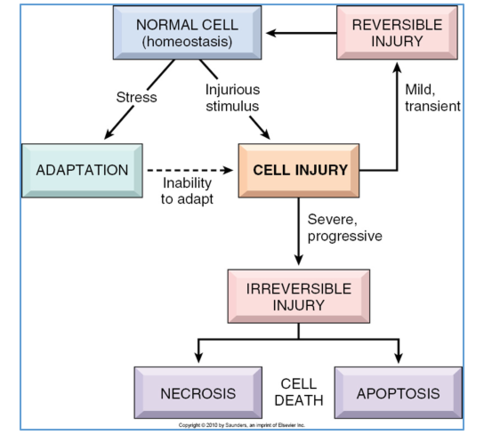
Cells are active, dynamic participants in their environment. They do not merely exist; they constantly adjust their internal structure and function to accommodate changing physiological demands and extracellular stresses. Under normal conditions, cells maintain a steady, balanced state called homeostasis, where the intracellular environment is kept within a highly regulated, narrow range of physiologic parameters.
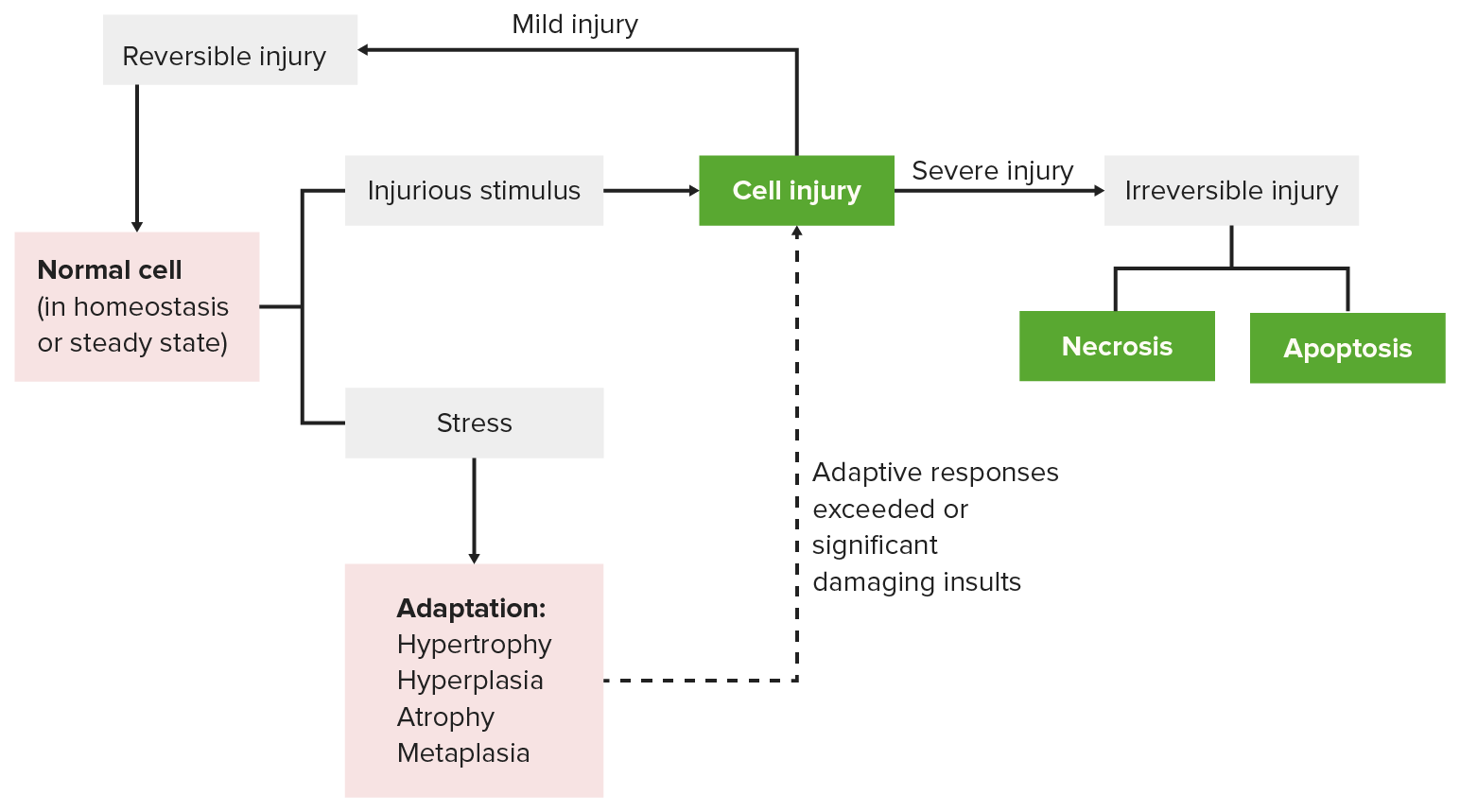
However, when a cell encounters stress or a pathologic stimulus, it follows a specific progression of responses:
- Adaptation: The cell's first response is to adapt. This allows the cell to achieve a "new steady state," preserving its viability and function in a hostile environment (e.g., a muscle cell growing larger to handle heavy lifting).
- Reversible Cell Injury: If the adaptive capability is exceeded, or if the external stress is inherently harmful but mild/transient, the cell sustains injury. However, up to a certain point, this injury is reversible, and the cell can return to a stable baseline if the stress is removed.
- Irreversible Cell Injury and Cell Death: If the injurious stimulus is severe, persistent, or rapid in onset, the cell passes a "point of no return." It suffers irreversible injury and ultimately dies via Necrosis or Apoptosis.
The Myocardium (Heart Muscle)
- Adaptation: In a patient with chronic high blood pressure, the heart must work harder to pump blood. In response to this increased hemodynamic load, the heart muscle cells enlarge (Hypertrophy). This adaptation helps short-term but increases the oxygen/metabolic demand of the heart.
- Reversible Injury: If a coronary artery narrows and the blood supply becomes inadequate (ischemia), the muscle first suffers reversible injury. The cells may swell and stop contracting efficiently, but they are not dead yet.
- Irreversible Injury: Unless the blood supply is rapidly restored (e.g., via a stent or clot-busting drug), the cells cross the threshold into irreversible injury, leading to cell death (Myocardial Infarction / Heart Attack).
Causes of Cell Injury
The agents that can injure cells range from the very large (physical trauma) to the submicroscopic (genetic mutations). They are generally grouped into seven categories:
1. Oxygen Deprivation (Hypoxia & Ischemia)
Hypoxia is a deficiency of oxygen, which fundamentally injures cells by reducing aerobic oxidative respiration (halting ATP production). It is an extremely important and common cause of cell injury and death.
- Ischemia (Arterial obstruction): The most common cause of hypoxia. Ischemia is a loss of blood supply. Elaboration: Ischemia is actually worse than pure hypoxia because it not only deprives the tissue of oxygen but also deprives it of metabolic substrates (glucose) and fails to remove toxic metabolic waste products (like lactic acid).
- Inadequate oxygenation of the blood: Due to cardiorespiratory failure (e.g., severe pneumonia or heart failure).
- Decreased oxygen-carrying capacity: Seen in severe anemia, severe blood loss, or Carbon Monoxide (CO) poisoning (where CO irreversibly binds hemoglobin, blocking oxygen).
2. Physical Agents
Physical forces can physically tear, burn, or irradiate cells. Examples include:
- Mechanical trauma (crush injuries, lacerations).
- Extremes of temperature (burns causing protein coagulation, deep cold causing ice crystal formation).
- Sudden changes in atmospheric pressure (decompression sickness).
- Radiation (ionizing radiation directly breaks DNA and creates free radicals).
- Electric shock (causes cardiac arrhythmias and severe tissue burning).
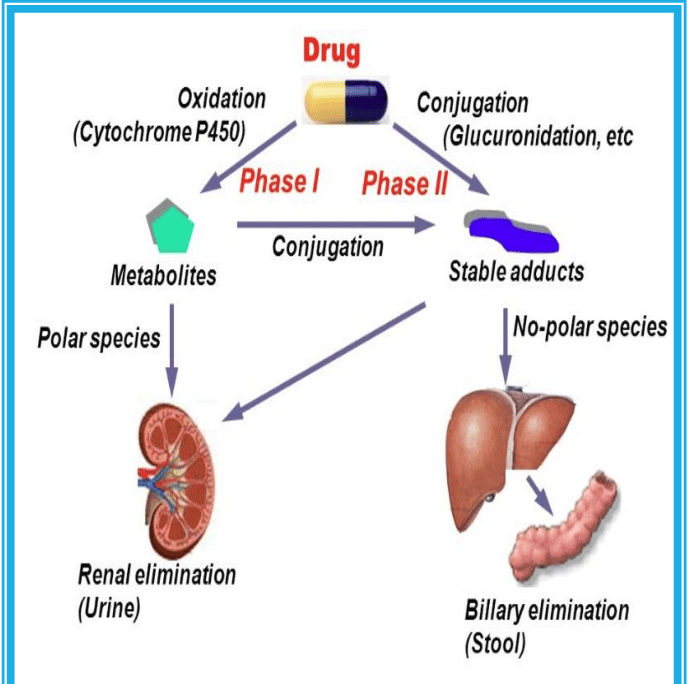
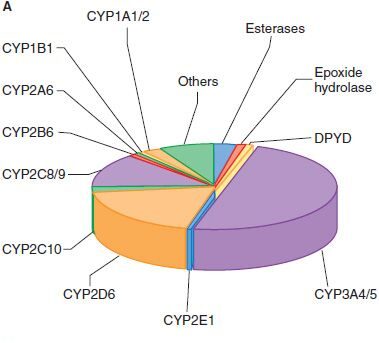
3. Chemical Agents and Drugs
The list of chemicals that may produce cell injury defies compilation; almost any substance can be toxic in the wrong amount.
- Harmless substances in excess: Simple chemicals like glucose or salt in hypertonic concentrations can cause cell injury directly by deranging electrolyte and fluid balance, drawing water out of cells and killing them. Even pure oxygen at high concentrations is toxic (causing oxidative stress).
- Poisons: Strong acids and alkalis directly destroy cell membranes.
- Toxins and Drugs: Trace amounts of poisons (cyanide, arsenic), environmental pollutants (asbestos, carbon monoxide), social drugs (ethanol/alcohol, cigarette smoke), and even therapeutic drugs (chemotherapy) can injure cells.
4. Infectious Agents
Biological pathogens attack cells either by directly invading them or by releasing toxins. These range from submicroscopic viruses (which hijack the cell's DNA/RNA machinery) to bacteria, fungi, protozoa, and metazoa (tapeworms several feet in length).
5. Immunologic Reactions
While the immune system defends against pathogens, friendly fire can cause massive tissue damage.
- Autoimmune diseases: Injurious reactions to endogenous self-antigens (the body attacks its own cells).
- Allergic reactions: Exaggerated immune responses to external agents (viruses, environmental substances, allergens) are important causes of tissue injury.
6. Genetic Abnormalities
Errors in the DNA code can lead to cell death by preventing the creation of essential proteins.
- Deficient protein function: Such as enzyme defects leading to inborn errors of metabolism.
- Accumulation of damage: Misfolded proteins or damaged DNA trigger cell death (apoptosis) if they are beyond repair.
- Chromosomal abnormalities: Examples include congenital malformations associated with Down Syndrome (Trisomy 21).
7. Nutritional Imbalances
A major global cause of cell injury.
- Deficiencies: Protein-calorie deficiencies cause an appalling number of deaths, chiefly among low-income populations. Specific vitamin deficiencies (e.g., Scurvy from Vitamin C deficiency) are not uncommon even in developed countries.
- Excesses: Nutritional excesses, such as obesity and high-fat diets, are significant factors in cellular injury leading to atherosclerosis, diabetes, and cancer.
Factors Affecting Cell Response to Injury
Why does one cell survive a stress while another dies? The outcome depends on two sets of variables:
Variables of the Injurious Agent
- Nature of the injury: (Is it a mild toxin or a severe physical crush?)
- Duration of injury: (Did the ischemia last for 5 minutes or 50 minutes?)
- Severity: (A low dose vs. a massive overdose of a drug).
Variables of the Cell
- Type: Skeletal muscle cells can withstand hypoxia for 2-3 hours without dying. A brain neuron will die in 3-5 minutes of hypoxia.
- State: A well-nourished cell full of glycogen has a better chance of surviving ischemia than a starved cell.
- Adaptability: Some cells are inherently better at changing their metabolic pathways to survive.
Note: Any injurious stimulus may simultaneously trigger multiple, interconnected mechanisms that damage cells.
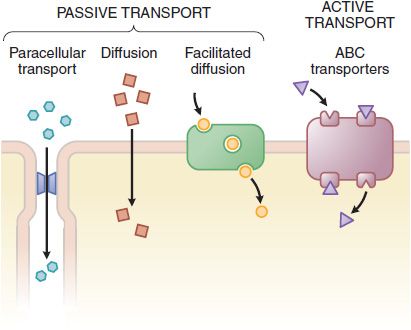
Mechanisms of Cell Injury
At the biochemical level, cellular injury usually targets four critical cellular components: Mitochondria, Cell Membranes, DNA, and Calcium homeostasis.
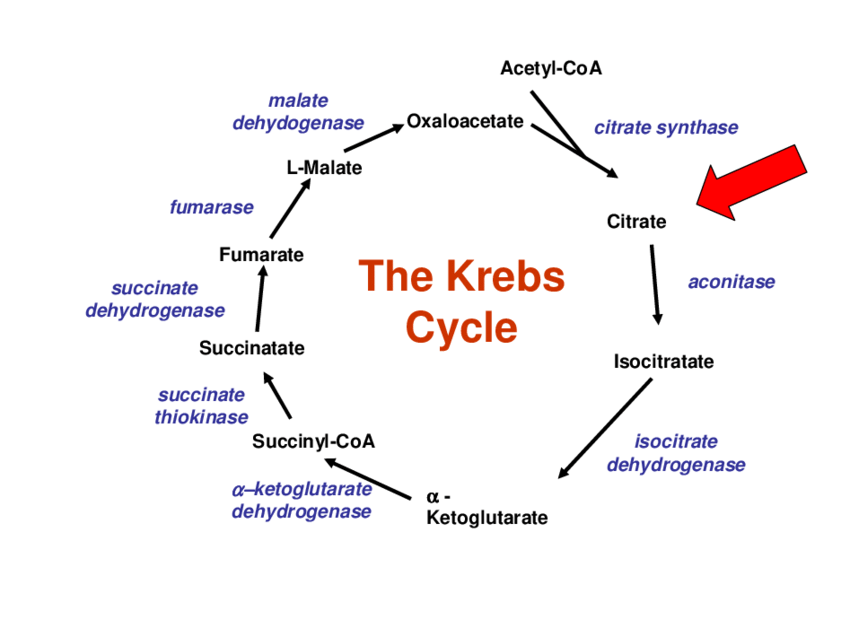
1. Mitochondrial Damage
Mitochondria are the "powerhouses" of the cell, supplying life-sustaining energy by producing ATP. They are critical players in all pathways leading to cell injury and death. Three major consequences arise when they are damaged:
- ATP Depletion: Decreased ATP synthesis is heavily associated with hypoxic and chemical injury.
- The Domino Effect of ATP Depletion: Without ATP, the sodium-potassium (Na+/K+) membrane pump fails. Sodium rushes into the cell, dragging water with it, causing the cell and endoplasmic reticulum (ER) to swell. Anaerobic glycolysis ramps up to compensate, producing lactic acid which drops the cellular pH. The acidic pH causes ribosomes to detach from the rough ER, resulting in a severe reduction in protein synthesis.
- Incomplete Oxidative Phosphorylation: Damaged mitochondria fail to process oxygen correctly, leading to the creation of toxic Reactive Oxygen Species (ROS).
- Leakage of Pro-Apoptotic Proteins: Damage to the mitochondrial membrane allows proteins (like Cytochrome c) to leak into the cytoplasm, signaling the cell to commit suicide (Apoptosis).
2. Membrane Damage
Early loss of selective membrane permeability is a consistent feature of most forms of cell injury (except apoptosis, where the membrane initially stays intact). Damage can occur to the outer plasma membrane, the mitochondrial membrane, or the lysosomal membrane.
- Causes: ATP depletion reduces phospholipid synthesis. Increased calcium activates phospholipases (which destroy the membrane) and proteases (which damage the cellular cytoskeleton).
- Result: Loss of the plasma membrane allows cellular contents to leak out and extracellular fluids to rush in. Loss of lysosomal membranes unleashes highly acidic, destructive enzymes into the cytoplasm, digesting the cell from the inside out.
3. Damage to DNA and Proteins
Damage to nuclear DNA activates specific sensors (like the p53 tumor suppressor protein). If the DNA damage is too severe to be repaired, p53 triggers apoptosis to prevent the cell from becoming cancerous.
- Causes of DNA Damage: Exposure to radiation, chemotherapeutic drugs, ROS, or spontaneous aging (e.g., deamination of cytosine to uracil).
- Protein Damage: Accumulation of misfolded proteins causes "ER stress," which also initiates apoptotic death pathways.
4. Influx of Intracellular Calcium (Loss of Calcium Homeostasis)
Normally, cytosolic calcium is kept extremely low. Calcium ions normally serve as tightly controlled second messengers. However, injurious agents (like ischemia or toxins) cause calcium to rush in from the extracellular fluid and leak out of the smooth ER and mitochondria.
Excess calcium is highly toxic because it inappropriately activates cellular enzymes:
- Phospholipases: Break down cell membranes.
- Proteases: Break down membrane and cytoskeletal proteins.
- Endonucleases: Fragment DNA and chromatin.
- ATPases: Accelerate the depletion of whatever ATP is left.
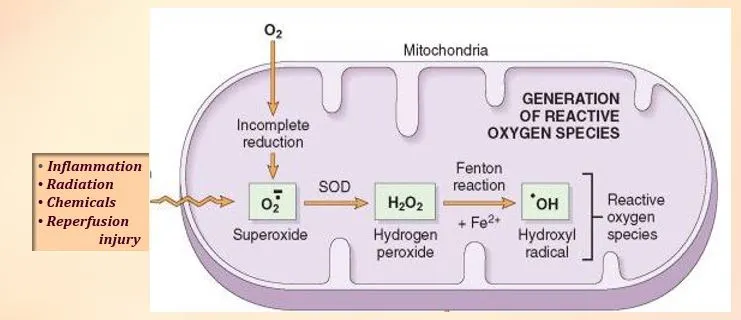
5. Accumulation of Oxygen-Derived Free Radicals (Oxidative Stress)
Free radicals are chemical species with a single unpaired electron in their outer orbit. This makes them highly unstable and aggressively reactive. They smash into adjacent molecules (lipids, proteins, DNA) to steal electrons, causing a chain reaction of damage. Cell injury by Reactive Oxygen Species (ROS) is a critical mechanism in chemical/radiation injury, ischemia-reperfusion injury, aging, and microbial killing.
The Three Main Free Radicals (ROS)
- Superoxide anion (O2•⁻): Contains one extra electron. Generated by incomplete reduction of oxygen during oxidative phosphorylation or by phagocytes.
- Hydrogen peroxide (H2O2): Contains two extra electrons. Converted from superoxide by Superoxide Dismutase (SOD).
- Hydroxyl radical (•OH): Contains three extra electrons. The most fiercely reactive ROS. Generated from water by radiation, or from H2O2 via the Fenton reaction.
Pathologic Effects of Free Radicals:
- Lipid Peroxidation: Radicals attack the double bonds of polyunsaturated lipids in cell membranes, destroying membrane integrity.
- Protein Modification: They promote protein cross-linking, breakdown, and misfolding.
- DNA Damage: They cause single- and double-strand breaks in DNA, leading to mutations and cell death.
The Progression of Cell Injury
All stresses and noxious influences exert their effects first at the molecular or biochemical level. There is a distinct time lag between the stress occurring and the morphologic (structural) changes becoming visible.
- Biochemical alterations (loss of ATP, enzyme activation) happen almost instantly.
- Ultrastructural changes (swelling of mitochondria, visible only under an electron microscope) happen minutes to hours later.
- Light microscopic changes (visible to a pathologist on a slide) take considerably longer (hours to days).
- Gross morphologic changes (visible to the naked eye, like a pale, dead piece of heart tissue) take the longest.
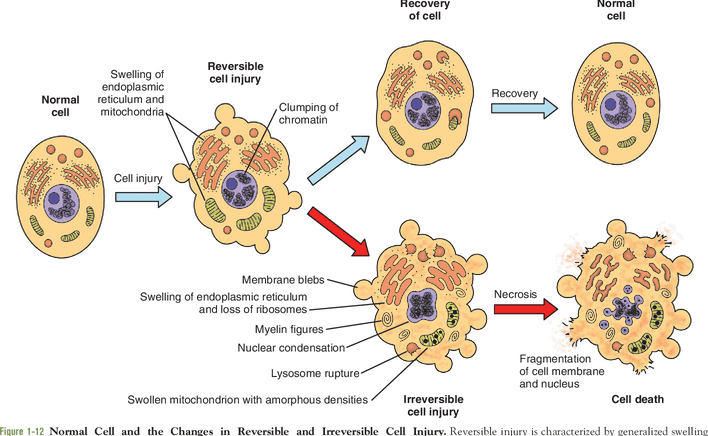
Reversible Cell Injury
Reversible injury characterizes the early stages or mild forms of injury. The functional and structural alterations are correctable if the damaging stimulus is removed. Two main morphological features are consistently seen:
1. Cellular Swelling
Cellular swelling is the very first manifestation of almost all forms of injury to cells. It is a direct result of the failure of energy-dependent ion pumps (the ATP-dependent Na+/K+ plasma membrane pump) due to ATP depletion from hypoxia or toxins. Sodium accumulates inside the cell, creating an osmotic pull that brings water rushing in.
- Gross Appearance: The affected organ (like the kidney, liver, or heart) becomes enlarged, pale, and heavy. The cut surface bulges outward and is slightly opaque.
- Microscopic Terminology: Pathologists historically refer to this using several terms:
- Cloudy swelling: Describing the gross/microscopic haziness.
- Hydropic change: Reflecting the accumulation of water.
- Vacuolar degeneration: Because the swollen, pinched-off segments of the ER appear as clear vacuoles inside the cytoplasm.
- Early Alterations include: Generalized swelling of the cell and organelles, blebbing of the plasma membrane, detachment of ribosomes from the ER, and early clumping of nuclear chromatin.
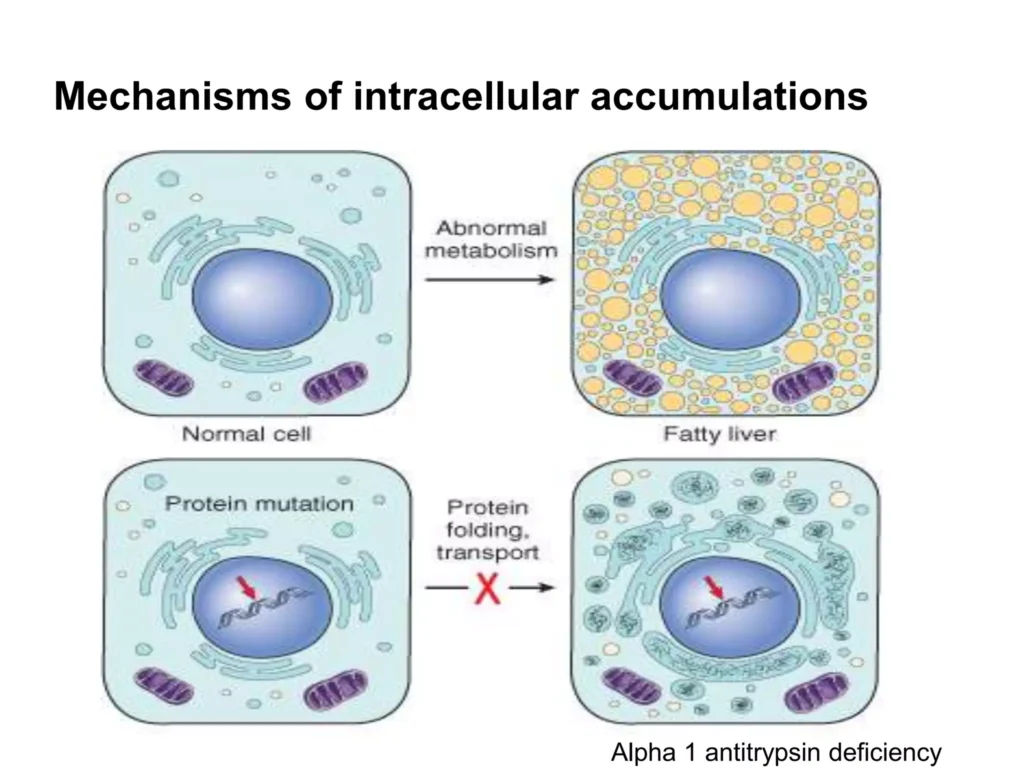
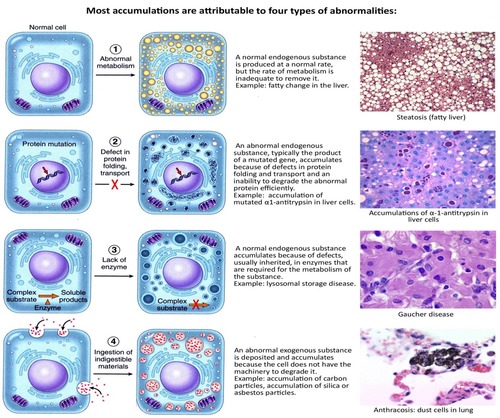
2. Fatty Change (Steatosis)
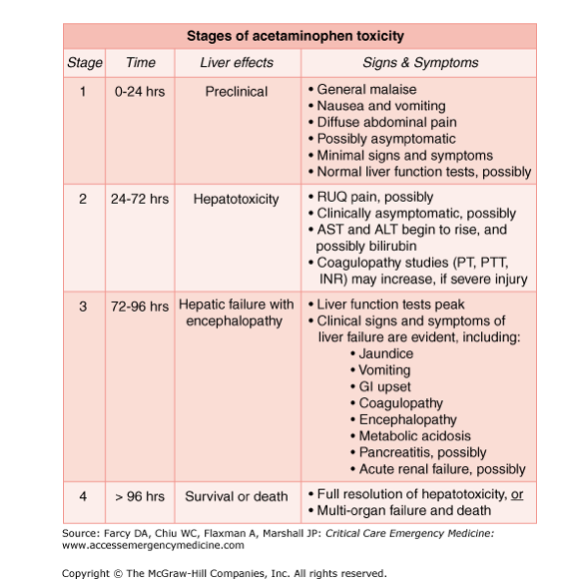
Fatty change describes the abnormal accumulation of triglycerides within parenchymal cells. It is most often seen in the liver because the liver is the major organ involved in fat metabolism, but it also occurs in the heart, muscle, and kidney.
- Mechanism: Toxic injury disrupts normal metabolic pathways (such as the inability to package triglycerides into apoproteins to export them), leading to a rapid accumulation of lipid-filled vacuoles in the cytoplasm.
- Causes: Toxins, protein malnutrition, obesity, diabetes mellitus, anoxia, and importantly, Alcohol abuse.
3. Intracellular vs Extracellular Depositions: Hyaline Change
The word "Hyaline" means glassy. It is a descriptive histologic term, not a specific substance. It refers to any alteration that yields a glassy, homogeneous, pink (eosinophilic) appearance in H&E stained tissue sections.
- Intracellular Hyaline: Mainly seen in epithelial cells.
- Hyaline droplets: Seen in proximal tubular epithelial cells of the kidney due to excessive protein reabsorption.
- Mallory’s hyaline: Aggregates of intermediate filaments in liver cells, a hallmark of alcoholic liver disease.
- Viral inclusions: Nuclear or cytoplasmic hyaline masses seen in viral infections (e.g., Cytomegalovirus).
- Russell bodies: Excessive immunoglobulins accumulating in the rough ER of plasma cells, forming pink, glowing globules.
- Extracellular Hyaline: Seen in connective tissues.
- Hyaline degeneration in old leiomyomas (fibroids) of the uterus.
- Hyalinized old scars consisting of dense fibro-collagenous tissue.
- Hyaline arteriolosclerosis: Thickening of small renal blood vessels due to hypertension and diabetes mellitus.
- Hyalinized glomeruli in chronic kidney disease.
Irreversible Cell Injury and Cell Death
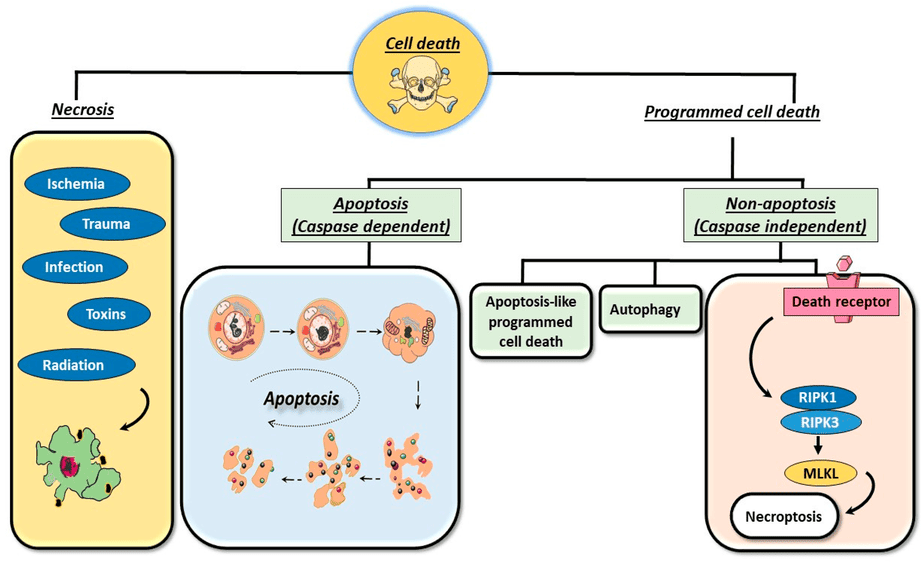
When the injury is too severe or prolonged, the cell passes a point of no return. There are two principal types of cell death: Necrosis and Apoptosis. They differ fundamentally in their mechanisms, morphology, and roles in physiology and disease.
A. NECROSIS
Necrosis is strictly a pathologic process. It is "cell murder." It is the culmination of irreversible cell injury.
Mechanism: Severe injury (ischemia, microbes, burns, chemicals) causes the cell membrane to fail. Intracellular proteins denature, and cellular contents leak out. This leakage invariably triggers a robust inflammatory response from the host to clean up the dead cells. Leakage of specific cellular enzymes into the blood is the basis for clinical blood tests (e.g., elevated Troponin indicates necrotic heart muscle).
Morphological Changes in Necrosis
Nuclear Changes (The hallmark of cell death):
- Pyknosis The nucleus dramatically shrinks and condenses into a solid, dark, basophilic (blue/purple) mass.
- Karyorrhexis The pyknotic nucleus undergoes fragmentation, breaking apart into destructive pieces.
- Karyolysis The chromatin totally breaks up and dissolves (fades away) due to DNAse enzymes, leaving an empty, "ghost" cell.
Cytoplasmic Changes:
- Increased eosinophilia: The cytoplasm turns intensely pink/red because denatured proteins bind eosin dye strongly, and the blue-staining RNA has been destroyed.
- Myelin figures: Whorled, clumped phospholipid masses derived from damaged cell membranes.
- Vacuolation: The cytoplasm appears bubbly and moth-eaten as organelles are digested.
Patterns of Tissue Necrosis
When masses of cells die, the gross and microscopic appearance takes on specific patterns depending on the cause and location:
The most common form. The architecture of the dead tissue is preserved for several days. The injury denatures not only structural proteins but also the enzymes that would normally digest the cell, so the cell maintains its shape as a firm, pale "ghost." This is characteristic of infarcts (areas of ischemic necrosis) in all solid organs except the brain.
Characterized by the rapid digestion of dead cells, transforming the tissue into a viscous liquid mass. Seen in focal bacterial/fungal infections because microbes strongly stimulate white blood cells. Leukocytes release digestive enzymes, liquefying the tissue into creamy yellow pus. Curiously, hypoxic death in the Central Nervous System (brain) always manifests as liquefactive necrosis.
Not a specific pattern, but a clinical term. Usually applied to a limb (e.g., lower leg or toes) that lost its blood supply and underwent coagulative necrosis across multiple tissue planes (Dry Gangrene). If a bacterial infection is superimposed, bacteria and inflammatory cells liquefy the dead tissue, turning it into Wet Gangrene.
The term means "cheeselike," referring to the friable, white, crumbly appearance of the dead tissue. It is most often encountered in foci of tuberculous (TB) infection. Microscopically, it appears as a structureless collection of lysed cells and granular debris enclosed within a distinct inflammatory border called a granuloma.
Refers to focal areas of fat destruction resulting from the release of activated pancreatic lipases (seen in severe emergency acute pancreatitis). The enzymes liquefy fat cell membranes in the peritoneum, splitting triglycerides into fatty acids. These fatty acids rapidly combine with calcium to produce grossly visible, chalky-white areas—a process known as fat saponification.
A special form of vascular damage seen in immune reactions. It occurs when complexes of antigens and antibodies deposit in the walls of arteries (vasculitis syndromes). These immune complexes, mixed with leaked plasma proteins, produce a bright pink, amorphous appearance on an H&E stain, resembling fibrin.
B. APOPTOSIS
Apoptosis is highly regulated, programmed cell death. It is "cell suicide." The cell activates enzymes that degrade its own nuclear DNA and nuclear/cytoplasmic proteins.
Key characteristic: The apoptotic cell breaks up into plasma membrane-bound fragments called apoptotic bodies. Because the membrane remains intact, cellular contents do not leak out. Therefore, apoptosis does not elicit an inflammatory reaction. The cell is quietly devoured by macrophages.
Causes of Apoptosis
- Physiologic (Normal): Required for normal embryogenesis (e.g., deleting webbing between fingers), hormone-dependent involution (menstruation), and eliminating cells that have outlived their usefulness.
- Pathologic (Disease): Eliminates cells injured beyond repair to prevent collateral damage. Causes include:
- DNA Damage: From radiation or chemotherapy. If the cell cannot fix the DNA, it kills itself to prevent cancer.
- Accumulation of Misfolded Proteins: Leads to Endoplasmic Reticulum (ER) stress, triggering apoptosis.
- Infections: Especially viruses. Cytotoxic T-Lymphocytes (CTLs) recognize viral proteins on infected cells and forcibly induce apoptosis to eliminate the reservoir of infection.
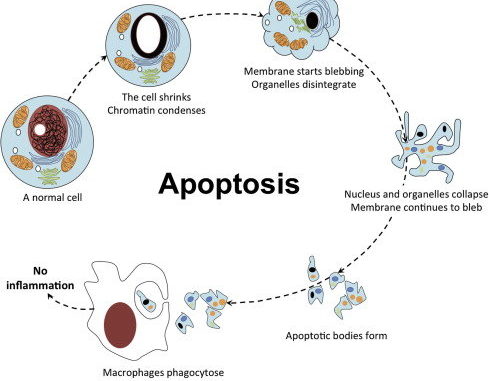
Morphology of Apoptosis
- Cell Shrinkage: The cell becomes smaller, cytoplasm becomes dense, and organelles pack tightly together.
- Chromatin Condensation: The most characteristic feature. Chromatin forms dense masses against the nuclear membrane, and the nucleus breaks into fragments.
- Cytoplasmic Blebs & Apoptotic Bodies: The membrane bubbles outward (blebbing) and pinches off, forming membrane-bound packets containing cytoplasm and organelles.
- Phagocytosis: Macrophages recognize receptors on the apoptotic bodies, ingest them rapidly, and degrade them without any surrounding inflammation.
Mechanism of Apoptosis (The Caspase Cascade)
Apoptosis is governed by a balance of death and survival signals. The ultimate goal is the activation of Caspases (enzymes that act as cellular executioners). The process involves an Initiation Phase (caspases become active) and an Execution Phase (caspases tear the cell apart).
There are two distinct initiation pathways that converge on execution:
- The Mitochondrial (Intrinsic) Pathway:
- This is the major pathway in most physiologic and pathologic situations.
- It is controlled by the permeability of the mitochondrial outer membrane, which is governed by the BCL2 family of proteins (20+ members).
- Anti-apoptotic (The Protectors): BCL2, BCL-XL, MCL1. They reside in the mitochondrial membrane and keep it sealed, preventing death.
- Pro-apoptotic (The Killers): BAX and BAK. When activated, they oligomerize (clump together) to punch channels in the mitochondrial membrane.
- Sensors (The Initiators / BH3-only proteins): BAD, BIM, BID, Puma, Noxa. When the cell senses stress (DNA damage, loss of growth factors), these sensors are activated. They neutralize the protectors and activate the killers (BAX/BAK).
- Once BAX/BAK punch holes in the mitochondria, Cytochrome C leaks into the cytoplasm. This initiates the caspase cascade by activating the initiator Caspase-9.
- The Death Receptor (Extrinsic) Pathway:
- Initiated by the engagement of "death receptors" on the plasma membrane. These are members of the Tumor Necrosis Factor (TNF) family, characterized by a cytoplasmic "death domain."
- The best-known receptors are TNFR1 and Fas (CD95).
- Mechanism: A T-lymphocyte expressing Fas Ligand (FasL) binds to the Fas receptor on a target cell. This causes several Fas molecules to group together inside the cell, forming a binding site for an adaptor protein called FADD.
- FADD pulls together inactive pro-caspases, forcing them to cleave each other and generate the active initiator Caspase-8 (or 10).
- Note: Viruses can produce a protein called FLIP, which blocks FADD binding, preventing Caspase-8 activation and allowing the virus to keep the host cell alive.
- Cross-talk: Caspase-8 can also cleave a protein called BID, linking the extrinsic pathway into the intrinsic mitochondrial pathway for an amplified death signal.
- The Execution Phase:
- Both pathways converge to activate the executioner caspases, notably Caspase-3 and Caspase-6. These enzymes act like molecular scissors. They cleave inhibitors of DNAse (allowing DNA degradation to begin), and they break down the structural cytoskeleton, leading to the physical fragmentation of the cell.
C. Other Mechanisms of Cell Death
- Necroptosis: A hybrid. Morphologically, it looks exactly like messy necrosis (cell swelling, lysis, inflammation). Mechanistically, it is strictly controlled by a signal transduction pathway like apoptosis. It is often called "programmed necrosis."
- Pyroptosis: Programmed cell death accompanied by the massive release of the fever-inducing cytokine IL-1 (causing a fiery inflammatory response).
- Ferroptosis: Triggered when excessive intracellular iron or reactive oxygen species overwhelm the cell's glutathione-dependent antioxidant defenses, leading to unchecked, fatal membrane lipid peroxidation.
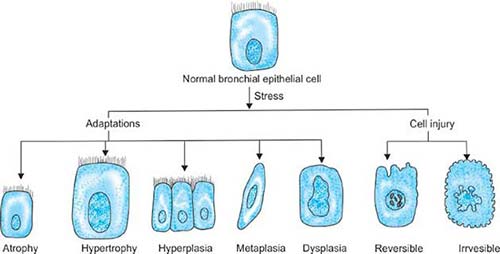
Cellular Adaptations to Stress
If a stress is not immediately lethal, cells adapt. Adaptations are reversible changes in the number, size, phenotype, metabolic activity, or functions of cells. They can be Physiologic (normal responses to hormones, like uterus growth in pregnancy) or Pathologic (responses to disease/stress to escape injury).
Definition: An increase in the size of existing cells, resulting in an increase in the size of the organ. There are no new cells. The bigger cells just contain more structural proteins and organelles to handle increased demand.
- Where it happens: Primarily in cells that cannot divide (Permanent cells like cardiac and skeletal muscle).
- Physiological Examples: Massive growth of the uterus during pregnancy (driven by estrogen). Bulging skeletal muscles in weightlifters due to increased demand.
- Pathological Examples: Cardiac muscle hypertrophy due to chronic hemodynamic overload (e.g., chronic hypertension or aortic valve disease). Smooth muscle hypertrophy in the stomach/intestines proximal to a stricture or obstruction (e.g., pyloric stenosis).
- Compensatory hypertrophy: If one kidney is removed, the remaining kidney undergoes massive hypertrophy (and some hyperplasia) to filter the body's blood alone.
Definition: An increase in the number of cells in an organ or tissue. It frequently occurs concurrently with hypertrophy.
- Where it happens: Only in cell populations capable of dividing (Labile cells like skin/mucosa, and Stable cells like liver/kidney/glands). It does not occur in permanent cells (neurons, cardiac muscle).
- Physiological Examples: Hormonal: Breast glandular proliferation during puberty and lactation. Endometrial proliferation during the normal menstrual cycle. Compensatory: Liver regeneration. If a surgeon removes 70% of a healthy liver, the remaining cells rapidly undergo hyperplasia to restore the liver to its original size.
- Pathological Examples: (Usually driven by excessive hormone or growth factor stimulation). Endometrial hyperplasia: Excess estrogen causes abnormal thickening of the uterine lining, leading to heavy bleeding (and a risk of cancer). Benign Prostatic Hyperplasia (BPH) in older men, driven by androgens. Viral infections: Human Papillomavirus (HPV) forces skin cells to divide rapidly, causing skin warts and mucosal lesions.
Definition: Shrinkage in the size of the cell by the loss of cell substance, resulting in the reduction of organ size. It represents a retreat to a smaller size at which survival is still possible.
- Mechanisms: A combination of decreased protein synthesis (due to reduced metabolic demand) and increased protein degradation (primarily via the ubiquitin-proteasome pathway). It is often accompanied by increased autophagy ("self-eating").
- Physiological Examples: Involution of the postpartum uterus; shrinkage of the thyroglossal duct in embryogenesis; atrophy of gonads after menopause.
- Pathological Examples: Disuse atrophy: Muscle wasting in a limb immobilized by a plaster cast. Denervation atrophy: Muscle wasting following nerve damage (e.g., polio or spinal cord injury). Ischemic atrophy: Brain shrinkage in late adulthood due to atherosclerotic narrowing of cerebral arteries. Nutritional atrophy: Marasmus/starvation. Cachexia in late-stage cancer. Endocrine atrophy: Loss of pituitary hormones causes adrenal and thyroid atrophy. Pressure atrophy: A slowly expanding benign tumor or aneurysm exerts physical pressure on surrounding healthy tissue, compromising its blood supply.
Definition: A reversible cellular adaptation in which one fully mature (adult) cell type—either epithelial or mesenchymal—is replaced by another mature cell type. It occurs via the genetic reprogramming of local stem cells.
- Squamous Metaplasia: The most common form. Smokers: In the respiratory tract, delicate ciliated columnar epithelium is repeatedly irritated by smoke and reprogrammed to produce rugged stratified squamous epithelium (losing mucus secretion and ciliary clearance). Vitamin A deficiency: Induces squamous metaplasia in the respiratory, urinary, and salivary tracts. Chronic irritation: Gallstones or kidney stones can induce squamous metaplasia in excretory ducts.
- Columnar Metaplasia: Barrett's Esophagus: In chronic acid reflux, the normal squamous epithelium of the lower esophagus is continuously burned by stomach acid. It undergoes metaplasia to become intestinal-like columnar epithelium (a precursor to esophageal cancer).
- Mesenchymal Metaplasia: Bone or cartilage forming in soft tissues where it doesn't belong (e.g., bone formation in injured muscle or aging arterial walls).
Cell Injury & Death Read More »