

Normal flora
Normal Flora and Host-Microbe Interactions
Concept of Normal Flora
The human body is not sterile; it is home to a vast and complex community of microorganisms. Normal Flora (also called the normal microbiota or commensals) are the microorganisms that live on or inside the body of a healthy person without causing disease under normal circumstances.
- The majority of normal flora are bacteria and some yeasts.
- Viruses, protozoa, and helminths (worms) are generally considered pathogens, not normal flora.
- These organisms can become opportunistic pathogens if they are introduced to a different part of the body or if the host becomes immunocompromised.

Types of Normal Flora
- Resident Flora: These are microorganisms that are almost always present in a particular area of the body at a given age. They are fixed types of microorganisms that, if disturbed (e.g., by soap or antibiotics), will promptly re-establish themselves. They are like the permanent residents of a neighborhood.
- Transient Flora: These are microorganisms that are present at a given time and then disappear. They are "temporary visitors" that may be present for hours, days, or weeks but do not establish a permanent colony because of competition from resident flora and the body's defense mechanisms.

Anatomic Distribution of Normal Flora
Normal flora colonize body surfaces that are exposed to the external environment. Internal organs and tissues like the blood, brain, muscles, and lungs are normally sterile.
Skin Flora
The skin is a complex environment with dry, moist, and oily areas, each hosting different microbes. The dominant group is Gram-positive bacteria because they are more resistant to drying and high salt concentrations (from sweat).
- Key residents include Staphylococcus epidermidis, Micrococcus species, and diphtheroids (like Propionibacterium acnes, which is linked to acne).
- Staphylococcus aureus can also be found, particularly in moist areas like the nostrils and perineum.
Oral and Upper Respiratory Tract Flora
The mouth is a rich habitat for microbes. The pharynx and nose are also heavily colonized.
- The mouth contains numerous species, especially Streptococcus species (like Streptococcus mutans, which contributes to dental caries by forming biofilms called plaque).
- Anaerobes thrive in the gingival crevices (the space between teeth and gums).
- The pharynx can be a colonization site for potentially pathogenic bacteria like Streptococcus pneumoniae, Haemophilus influenzae, and Neisseria meningitidis, which may not cause illness in a healthy carrier but can cause disease if they spread.
Gastrointestinal (GI) Tract Flora
The density and composition of flora change drastically along the GI tract.
- Stomach: Has very few microbes due to its high acidity (low pH). Most are transient. Helicobacter pylori is an important exception that can survive the acid and is a major cause of stomach ulcers.
- Small Intestine: The duodenum is sparsely populated, but microbial numbers increase toward the ileum.
- Large Intestine (Colon): Contains the largest microbial population in the body (10⁹ to 10¹¹ bacteria per gram of feces). It is predominantly (>99%) populated by anaerobes like Bacteroides, Clostridium, and facultative anaerobes like E. coli.
Urogenital Flora
- Vagina: The flora is dominated by Lactobacillus species in women of reproductive age. These bacteria ferment glycogen to produce lactic acid, creating an acidic pH (around 4.5) that prevents the overgrowth of pathogens like the yeast Candida albicans. The flora changes with age and hormonal levels.
- Urethra: The distal (outer) part of the urethra is colonized by a sparse mixed flora. The rest of the urinary tract (bladder, ureters, kidneys) is sterile.
The Roles and Importance of Normal Flora
Benefits to the Host
- Gut bacteria synthesize and secrete essential vitamins that humans cannot produce or get in sufficient quantities from diet alone. Key examples include Vitamin K (crucial for blood clotting) and several B-complex vitamins (like B12, biotin, riboflavin, and folate).
- They also aid in the digestion and absorption of certain carbohydrates (like fiber) that human digestive enzymes cannot break down, releasing beneficial short-chain fatty acids (SCFAs).
- Normal flora prevent colonization by harmful pathogens by competing for limited attachment sites on epithelial surfaces.
- They also compete for essential nutrients, effectively "starving out" potential invaders.
- This process creates a biological barrier, making it much harder for pathogens to establish an infection.
- The constant presence of normal flora stimulates the development and maturation of the host's immune system, particularly in the gut (Gut-Associated Lymphoid Tissue or GALT).
- This "training" helps the immune system to differentiate between harmless commensals and dangerous pathogens.
- The exposure to flora leads to the production of natural antibodies that may cross-react with and provide protection against related pathogens encountered later in life.
- Many gut bacteria produce substances that inhibit or kill other, more harmful bacteria.
- Lactobacillus species in the vagina produce lactic acid, creating a low pH environment that prevents the overgrowth of yeast like Candida albicans.
- Gut bacteria can produce fatty acids, peroxides, and highly specific antibiotic-like proteins called bacteriocins (e.g., colicins produced by E. coli), which are lethal to closely related bacteria.
- Some normal flora can metabolize and detoxify certain harmful compounds that are ingested in food or produced during metabolism.
Harmful Effects and Disadvantages of Normal Flora
- The Host is Immunocompromised: A weakened immune system due to HIV/AIDS, chemotherapy, immunosuppressive drugs (for transplants), or malnutrition allows normally harmless flora to become pathogenic.
- Flora are Introduced to a Sterile Site:
- A break in the skin from a wound or surgery can allow Staphylococcus aureus to enter the bloodstream, causing bacteremia or sepsis.
- Perforation of the intestine (e.g., from an ulcer or injury) can release gut flora like Bacteroides fragilis into the abdominal cavity, causing peritonitis.
- E. coli from the gut is the most common cause of Urinary Tract Infections (UTIs) when it ascends the urethra.
- While rare, some normal flora have been linked to cancer. For example, chronic inflammation caused by certain gut bacteria may contribute to the development of colorectal cancer.
- Helicobacter pylori, which can be part of the stomach flora, is a known carcinogen linked to stomach cancer.
- Normal flora from a healthcare worker can be transmitted to a vulnerable patient, where it can cause a nosocomial (hospital-acquired) infection. This is a major reason for strict hand hygiene protocols.

Symbiotic Relationships
Symbiosis (from Greek, meaning "living together") is a close and long-term biological interaction between two different species. The organisms involved are called symbionts. These relationships are critical in understanding how microbes interact with their hosts.
- Definition: A relationship where both organisms benefit. It is a win-win situation.
- Example 1 (Classic): E. coli in the human colon gets a stable, nutrient-rich environment, and in return, it produces Vitamin K, which is essential for human blood clotting.
- Example 2: Ruminant animals like cows have microbes in their rumen that digest cellulose from grass, which the cow cannot do on its own. The microbes get food, and the cow gets nutrients from the digested cellulose.
- Definition: An association where one organism benefits, and the other is largely unaffected (neither harmed nor helped).
- Example 1: Staphylococcus epidermidis living on human skin gets nutrients from dead skin cells and secretions, but it typically does not harm or benefit the human host.
- Example 2: Many bacteria in the human mouth live as commensals, feeding on food particles without causing any issues in a healthy individual with good oral hygiene.
- Note: The line between commensalism and mutualism/parasitism can be blurry. A commensal can become an opportunistic pathogen if circumstances change.
- Definition: A relationship where one organism (the parasite) benefits at the expense of the other (the host), which is harmed.
- This is the relationship all pathogenic microorganisms have with their hosts. The degree of harm can range from mild (like in the common cold) to severe and fatal (like in Ebola).
- Example 1: Plasmodium falciparum, the protozoan that causes malaria, lives in and destroys human red blood cells, causing severe disease.
- Example 2: Mycobacterium tuberculosis lives inside human lung cells, causing tissue damage and the disease tuberculosis.
- Definition: A relationship where one organism is harmed, and the other is unaffected.
- Example: The mold Penicillium produces penicillin, which kills nearby bacteria. The bacteria are harmed, but the mold is not significantly affected by the bacteria's presence or absence. This is the basis of antibiotic action.
Characteristics and Spread of Infectious Disease
An infection is the successful colonization of a host by a microorganism. Infections can lead to disease, which causes signs and symptoms resulting in a deviation from the normal structure or functioning of the host. Microorganisms that can cause disease are known as pathogens.
The signs of disease are objective and measurable, and can be directly observed by a clinician. Vital signs, which are used to measure the body’s basic functions, include body temperature (normally 37 °C [98.6 °F]), heart rate (normally 60–100 beats per minute), breathing rate (normally 12–18 breaths per minute), and blood pressure (normally between 90/60 and 120/80 mm Hg). Changes in any of the body’s vital signs may be indicative of disease. For example, having a fever (a body temperature significantly higher than 37 °C or 98.6 °F) is a sign of disease because it can be measured.
Unlike signs, symptoms of disease are subjective. Symptoms are felt or experienced by the patient, but they cannot be clinically confirmed or objectively measured. Examples of symptoms include nausea, loss of appetite, and pain. Such symptoms are important to consider when diagnosing disease, but they are subject to memory bias and are difficult to measure precisely. Some clinicians attempt to quantify symptoms by asking patients to assign a numerical value to their symptoms. For example, the Wong-Baker Faces pain-rating scale asks patients to rate their pain on a scale of 0–10. An alternative method of quantifying pain is measuring skin conductance fluctuations. These fluctuations reflect sweating due to skin sympathetic nerve activity resulting from the stressor of pain.
Distinguishing Between Signs and Symptoms of Disease
Understanding this difference is fundamental to accurate clinical assessment and diagnosis. It forms the basis of how a healthcare provider documents a patient's condition.
- Key Examples: Fever (a measured temperature of 38.5°C), high blood pressure, a visible rash, edema (swelling), abnormal heart sounds heard with a stethoscope, elevated white blood cell count from a lab test, or a positive rapid diagnostic test for malaria.
- Key Examples: Pain, nausea, headache, fatigue, chills, itching, dizziness, or a general feeling of being unwell (malaise).
Patient Case Scenario: Signs vs. Symptoms in Pneumonia
A 45-year-old man comes to the clinic. His clinical picture illustrates the difference:
- A temperature of 39.2°C (a sign: fever).
- A respiratory rate of 28 breaths/minute (a sign: tachypnea).
- An oxygen saturation of 89% on room air (a sign: hypoxemia).
- Upon listening to his chest with a stethoscope, the nurse hears crackles in the right lower lobe (a sign).
In this case, the patient's subjective symptoms led him to seek care, while the objective signs measured by the nurse help confirm a diagnosis of pneumonia.
Nomenclature of Disease Conditions
A specific group of signs and symptoms characteristic of a particular disease is called a syndrome. Many syndromes are named using a nomenclature based on signs and symptoms or the location of the disease.
| Affix | Meaning | Example and Explanation |
|---|---|---|
| cyto- | cell | cytopenia: reduction in the number of blood cells |
| hepat- | of the liver | hepatitis: inflammation of the liver |
| -pathy | disease | neuropathy: a disease or disorder of the nervous system |
| -emia | of the blood | bacteremia: the presence of bacteria in the blood |
| -itis | inflammation | colitis: inflammation of the colon |
| -lysis | destruction | hemolysis: the destruction of red blood cells |
| -oma | tumor | lymphoma: cancer of the lymphatic system |
| -osis | diseased or abnormal condition | leukocytosis: an abnormally high number of white blood cells |
Classifying Diseases
Infectious vs. Non-infectious Diseases
An infectious disease is any disease caused by the direct effect of a pathogen. A pathogen may be cellular (bacteria, parasites, and fungi) or acellular (viruses, viroids, and prions). Some infectious diseases are also communicable, meaning they are capable of being spread from person to person through either direct or indirect mechanisms. Some infectious communicable diseases are also considered contagious diseases, meaning they are easily spread from person to person. Not all contagious diseases are equally so; the degree to which a disease is contagious usually depends on how the pathogen is transmitted. For example, measles is a highly contagious viral disease that can be transmitted when an infected person coughs or sneezes and an uninfected person breathes in droplets containing the virus. Gonorrhea is not as contagious as measles because transmission of the pathogen (Neisseria gonorrhoeae) requires close intimate contact (usually sexual) between an infected person and an uninfected person.
In contrast to communicable infectious diseases, a noncommunicable infectious disease is not spread from one person to another. One example is tetanus, caused by Clostridium tetani, a bacterium that produces endospores that can survive in the soil for many years. This disease is typically only transmitted through contact with a skin wound; it cannot be passed from an infected person to another person. Similarly, Legionnaires disease is caused by Legionella pneumophila, a bacterium that lives within amoebae in moist locations like water-cooling towers. An individual may contract Legionnaires disease via contact with the contaminated water, but once infected, the individual cannot pass the pathogen to other individuals.
Types of Non-infectious Diseases
| Type | Definition | Example |
|---|---|---|
| Inherited | A genetic disease passed from parent to offspring. | Sickle cell anemia |
| Congenital | A disease that is present at or before birth (can be genetic or caused by other factors). | Down syndrome |
| Degenerative | Progressive, irreversible loss of function in organs or tissues. | Parkinson disease |
| Nutritional deficiency | Impaired body function due to a lack of specific nutrients. | Scurvy (vitamin C deficiency) |
| Endocrine | Disease involving malfunction of hormone-producing glands. | Hypothyroidism |
| Neoplastic | Abnormal cell growth (can be benign or malignant). | Lung cancer |
| Idiopathic | A disease for which the cause is unknown. | Idiopathic pulmonary fibrosis |
Types of Infectious Diseases by Acquisition and Transmission
- A disease that is very easily spread is often called a contagious disease. Measles and chickenpox are highly contagious.
- Examples: Tuberculosis, HIV, Measles, Influenza, Cholera.
- Example 1 (Environmental): Tetanus. A person gets tetanus when Clostridium tetani spores from the soil enter a deep wound. You cannot "catch" tetanus from someone who has it.
- Example 2 (Opportunistic): A bladder infection caused by a person's own E. coli from their gut.
- Example: A patient develops a wound infection after surgery because the surgical site was not properly cleaned, or develops sepsis after a procedure with a contaminated endoscope.
- Example: A patient develops a urinary tract infection from an indwelling catheter (Catheter-Associated UTI or CAUTI), or pneumonia from being on a ventilator (Ventilator-Associated Pneumonia or VAP).
- Example: Rabies from a dog bite, Anthrax from handling infected livestock, or Avian Influenza from infected birds.

The Stages of an Acute Infectious Disease
An acute disease typically progresses through five distinct stages. The severity of signs and symptoms directly correlates with the number of pathogens present in the body.
1. Incubation Period: The initial period between infection and the first appearance of any signs or symptoms. The length varies greatly depending on the pathogen, the initial dose, and the host's immunity.

































![[Full anterior and posterior views of the human skeleton with major bones and key joints labeled.]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/Full-anterior-and-posterior-views-of-the-human-skeleton-with-major-bones-and-key-joints-labeled.jpg)
![[Diagram showing the human skeleton with the axial skeleton highlighted or color-coded differently from the appendicular skeleton.]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/axial-skeleton-highlighted-or-color-coded-differently-from-the-appendicular-skeleton.jpg)
![[Cross-section diagram of a bone showing the outer layer of compact bone surrounding the inner network of spongy bone. Maybe show a flat bone cross-section (diploe) as well.]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/ClassificationofBonesontheBasisofShape-e1751439762811.jpg)
![[Detailed, labeled diagram of a long bone showing all key anatomical features: diaphysis, epiphysis, metaphysis, epiphyseal line/plate, articular cartilage, periosteum, endosteum, medullary cavity, compact bone, spongy bone.]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/603_Anatomy_of_Long_Bone-1.jpg)
![[Cross-section diagram of a bone showing the outer layer of compact bone surrounding the inner network of spongy bone. Maybe show a flat bone cross-section (diploe) as well.]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/Cross-section-diagram-of-a-bone-showing-the-outer-layer-of-compact-bone.jpg)
![[Diagram showing the different types of bone cells (osteogenic cell, osteoblast, osteocyte, osteoclast) and their location/role in bone tissue.]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/types-of-bone-cells-osteogenic-cell-osteoblast-osteocyte-osteoclast.jpg)
![[Diagram illustrating the process of endochondral ossification, showing the hyaline cartilage model being progressively replaced by bone tissue from primary and secondary ossification centers.]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/endochondral-ossification.jpg)
![[Diagram illustrating both longitudinal growth at the epiphyseal plate and appositional growth (growth in width) occurring simultaneously in a long bone.]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/longitudinal-growth-at-the-epiphyseal-plate-and-appositional-growth-1.jpg)
![[Diagram or table illustrating common types of fractures (e.g., transverse, oblique, spiral, comminuted, compression, greenstick, open/closed).]](https://nursesrevisionuganda.com/wp-content/uploads/2023/05/ezgif.com-webp-to-jpg-11-1.jpg)
![[Diagram illustrating the four stages of fracture healing: 1. Hematoma formation, 2. Fibrocartilaginous callus formation, 3. Bony callus formation, 4. Bone remodeling.]](https://nursesrevisionuganda.com/wp-content/uploads/2023/03/Illustration-of-stages-in-bone-healing-after-a-fracture.jpg)
![[Diagram illustrating the three main structural classifications of joints: Fibrous joint (suture), Cartilaginous joint (symphysis or synchondrosis), and Synovial joint. Clearly label the components of a synovial joint (articular cartilage, joint capsule, synovial membrane, synovial fluid, joint cavity, ligaments).]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/Classification-of-Joints.png)
![[Diagrams illustrating the six different types of synovial joints (Plane, Hinge, Pivot, Condyloid, Saddle, Ball-and-Socket) with a small illustration of the bone shapes and arrows indicating the types of movement allowed for each, and examples of where they are found in the body.]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/cartilagenous-joints.jpg)
![[Diagram illustrating the three main structural classifications of joints: Fibrous joint (suture), Cartilaginous joint (symphysis or synchondrosis), and Synovial joint. Clearly label the components of a synovial joint (articular cartilage, joint capsule, synovial membrane, synovial fluid, joint cavity, ligaments).]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/types-of-synovial-joints-1.jpg)
![[Images illustrating common joint disorders: Osteoarthritis (showing cartilage erosion), Rheumatoid Arthritis (showing joint deformity), Gout (inflamed joint), diagram of a sprained ankle, diagram of a joint dislocation.]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/common-joint-disorders.webp)
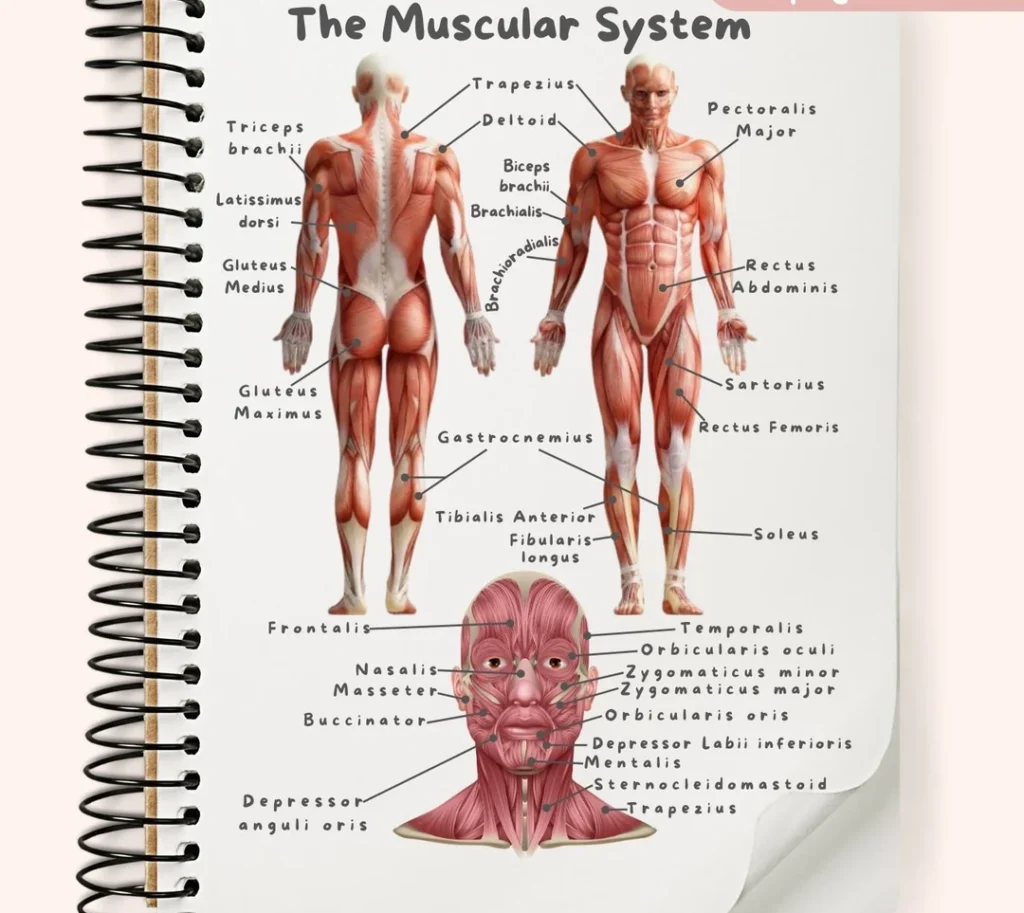
![[An overview diagram showing the major muscles of the human body, anterior and posterior views. Label main muscle groups.]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/1105_Anterior_and_Posterior_Views_of_Muscles2-1024x631-1.jpg)
![[Microscopic view of skeletal muscle tissue, showing its long, cylindrical fibers, striations, and multiple nuclei located peripherally.]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/microscopic-skeletal-muscle-e1751345586323.webp) Smooth Muscle:
Smooth Muscle:
![[Microscopic view of smooth muscle tissue, highlighting its spindle shape, single central nucleus, and lack of striations.]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/Smooth-musclet-tissue-1-1-e1751389483746.png) Cardiac Muscle:
Cardiac Muscle:
![[Microscopic view of cardiac muscle tissue, showing striations, branching cells, central nuclei, and prominent intercalated discs connecting the cells.]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/Microscopic-view-of-cardiac-muscle-tissue.jpg)
![[Diagram showing the hierarchical structure of a skeletal muscle, starting from the entire muscle organ, down to a fascicle, a single muscle fiber (cell), and finally a myofibril, illustrating the connective tissue coverings at each level.]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/Diagram-showing-the-hierarchical-structure-of-a-skeletal-muscle.jpg)
![[Detailed diagram illustrating the structure of thick (myosin) and thin (actin, tropomyosin, troponin, elastic/titin) filaments and showing their arrangement within a sarcomere.]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/Structure-of-Sarcomere.webp)
![[Diagram of a motor unit, showing a motor neuron originating from the spinal cord, its axon branching out, and each axon branch forming a neuromuscular junction with a different skeletal muscle fiber within the muscle.]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/Diagram-of-a-motor-unit.jpg)
![[Diagram of a motor unit, showing a motor neuron originating from the spinal cord, its axon branching out, and each axon branch forming a neuromuscular junction with a different skeletal muscle fiber within the muscle.]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/nueromuscular-junction.png)
![[Detailed diagram of the neuromuscular junction, clearly labeling the presynaptic axon terminal, synaptic vesicles containing ACh, the synaptic cleft, the motor end-plate with junctional folds, and acetylcholine receptors on the muscle fiber membrane.]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/Detailed-diagram-of-the-neuromuscular-junction-clearly-labeling-the-presynaptic-axon-terminal.jpg)
![[Series of detailed diagrams illustrating the step-by-step process of neuromuscular transmission at the NMJ, from arrival of action potential to ACh release, binding, EPP generation, and initiation of muscle action potential.]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/Step-by-step-process-of-neuromuscular-transmission-at-the-NMJ-1.jpg)
![[Diagram clearly illustrating the difference between a relaxed sarcomere and a contracted sarcomere, showing how the thin filaments move inwards and the Z-discs get closer while the thick and thin filaments retain their original length.]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/Diagram-clearly-illustrating-the-difference-between-a-relaxed-sarcomere-and-a-contracted-sarcomere.jpg)
![[Series of detailed diagrams illustrating the steps of the sliding filament theory and cross-bridge cycling: 1. Calcium binding to troponin/tropomyosin movement, 2. Cross-bridge formation, 3. Power stroke, 4. ATP binding and detachment, 5. ATP hydrolysis and re-cocking of myosin head.]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/steps-of-the-sliding-filament-theory-and-cross-bridge-cycling.jpg)
![[Flowchart or diagram comparing the three main metabolic pathways for ATP production in muscle cells: Creatine Phosphate System (Direct Phosphorylation), Anaerobic Glycolysis, and Aerobic Respiration. Show inputs, outputs, speed, duration supported, and location.]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/Flowchart-or-diagram-comparing-the-three-main-metabolic-pathways-for-ATP-production-in-muscle-cells-1.jpg)
![[Diagram clearly illustrating the concepts of muscle origin and insertion using a specific muscle (e.g., Biceps Brachii or Gastrocnemius) and showing how contraction pulls the insertion towards the origin.]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/concepts-of-muscle-origin-and-insertion-using-a-specific-muscle.jpg)
![[Diagram illustrating the roles of different muscles (agonist, antagonist, synergist, fixator) during a specific movement, such as elbow flexion or forearm pronation/supination.]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/roles-of-different-muscles-agonist-antagonist-synergist-fixator.jpg)
![[Diagram illustrating isotonic (concentric and eccentric) and isometric contractions with simple examples like lifting and holding a weight.]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/isotonic-concentric-and-eccentric-and-isometric-contractions.jpg)
![[Illustrations showing various common body movements (flexion, extension, abduction, adduction, rotation, circumduction) at different joints.]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/common-body-movements-flexion-extension-abduction.webp)
![[Illustrations showing movements of the ankle and foot (dorsiflexion, plantar flexion, inversion, eversion) and movements of the forearm/wrist (supination, pronation, opposition of the thumb).]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/common-body-movements-flexion-extension-abduction-adduction-rotation-circumduction-at-different-joints.jpg)
![[Diagrams illustrating the concept of muscle origin and insertion, and showing how muscles act on joints as levers (maybe show a simple example like the elbow joint).]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/concept-of-muscle-origin-and-insertion-and-showing-how-muscles-act-on-joints-as-levers-1.png)
![[Images illustrating common muscular disorders: muscle strain, tendinitis, muscular dystrophy (showing muscle wasting), myasthenia gravis (e.g., drooping eyelid), diagram of compartment syndrome, image of an inguinal hernia.]](https://nursesrevisionuganda.com/wp-content/uploads/2025/07/common-muscular-disorders.jpg)

