
Normal Pathway of Aqueous Humor
Aqueous fluid Circulation:
- The aqueous fluid is a clear fluid produced in the Cilliary body then it will flow out through the Iris, lens, Pupil, Cornea, Anterior Chamber Trabecular Meshwork then to the Schlemm Canal.
- The aqueous fluid flows nourishing the cornea and lens.
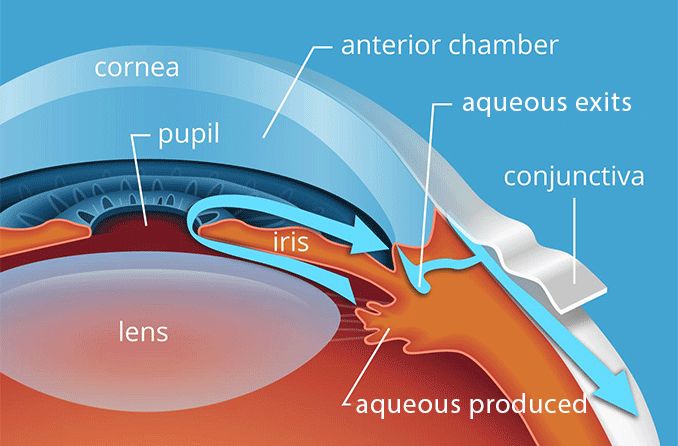
- The eye has an internal fluid circulation system
- Fluid is produced at the base of the iris
- The fluid flows through the pupil to the front of the iris
- The fluid exits the eye at the angle between the iris and the cornea where it drains through a spongy meshwork
The IOP is determined by:
- Rate of aqueous production in the ciliary body
- Resistance encountered by the aqueous as it flows out of the passages.

Pathophysiology of Glaucoma
The underlying cause of open-angle glaucoma remains unclear.
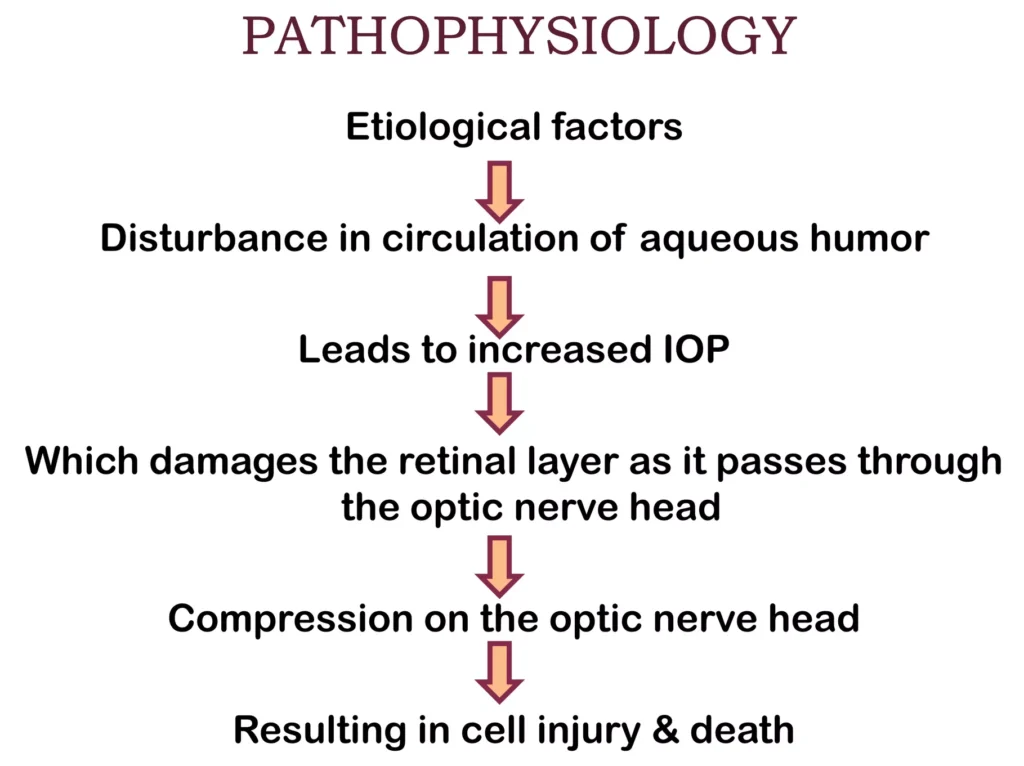
Excess production of aqueous humor, and decreased outflow of aqueous humor, are the key factors in the pathophysiology of glaucoma.
Excess production of aqueous humor can occur, leading to an increase in intraocular pressure. Additionally, there may be a decrease in the outflow of aqueous humor due to blockage or narrowing of the drainage pathways.
The increased intraocular pressure puts pressure on the optic nerve, compromising its blood supply and leading to ischemia. The optic nerve is responsible for transmitting visual information from the eye to the brain. When the optic nerve is damaged, it can result in the loss of vision.
Diagnosis of Glaucoma
Screening for glaucoma is usually performed as part of a standard eye examination performed by optometrists and ophthalmologists.
- History taking: Examination for glaucoma also could be assessed with more attention given to sex, race, history of drug use, refraction, inheritance and family history.
Glaucoma tests;
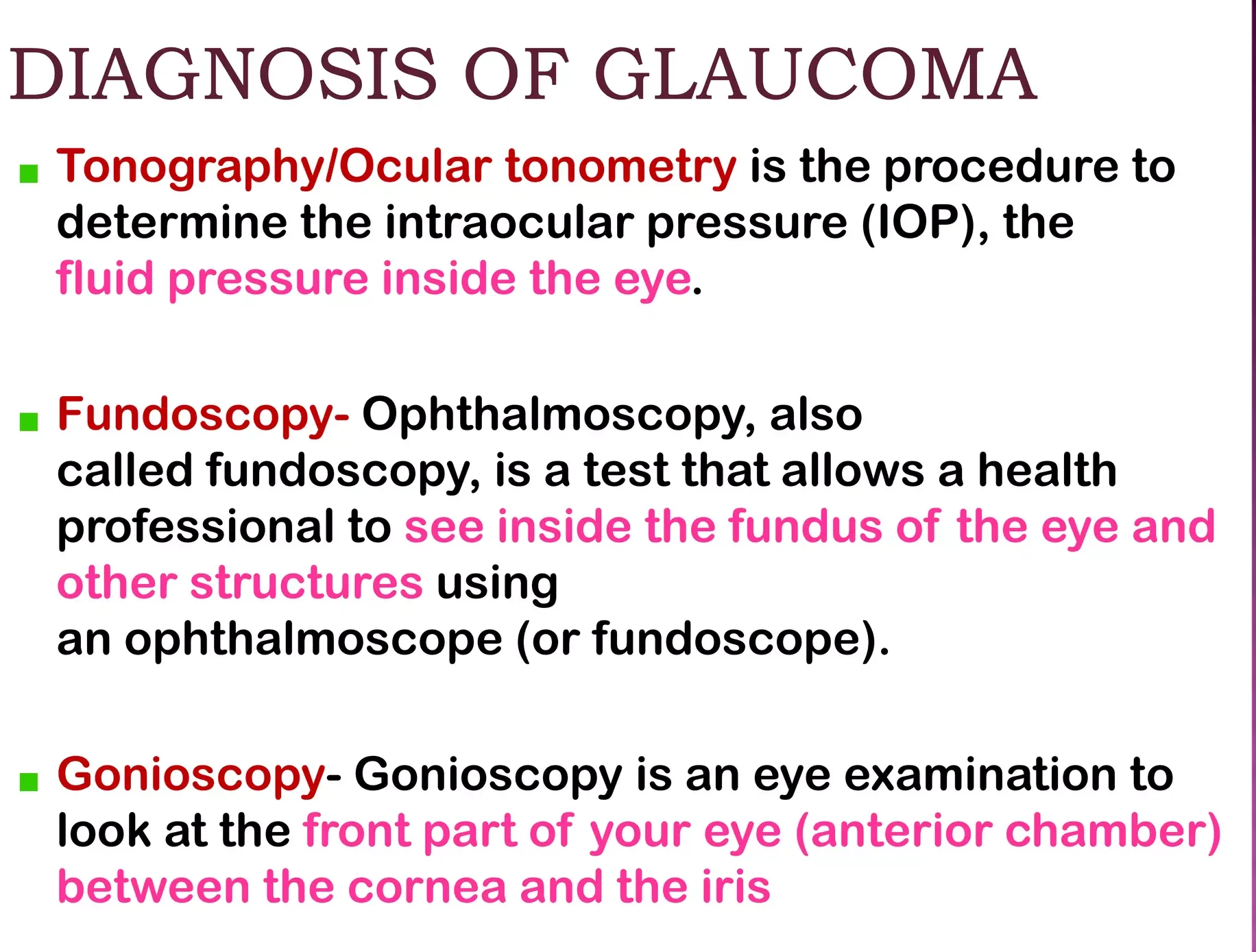
- Tonometry: This test measures the intraocular pressure (IOP) within the eye. The examiner will numb the eye with eye drops and then use a tonometer to measure the pressure. This can be done by applying a puff of warm air or using a tiny tool.
- Gonioscopy: This test examines the angle where the iris meets the cornea. Eye drops are used to numb the eye, and a hand-held contact lens with a mirror is gently placed on the eye to visualize the angle between the cornea and iris.
- Ophthalmoscopy (Dilated Eye Examination): This test examines the shape and color of the optic nerve. Eye drops are used to dilate the pupil, allowing the examiner to use a magnification device with a light to examine the optic nerve
- Perimetry (Visual Field Test): This test assesses the complete field of vision. Patient is asked to look straight ahead while a light spot is presented in different areas of the peripheral vision. This helps create a map of the vision.
- Pachymetry: This test measures the thickness of the cornea. A pachymeter is gently placed on the front of the eye to measure the corneal thickness. This measurement can help in understanding eye pressure readings.
- Nerve Fiber Analysis: Imaging techniques such as optical coherence tomography, scanning laser polarimetry, and scanning laser ophthalmoscopy can be used to assess the thickness of the retinal nerve fiber layer.
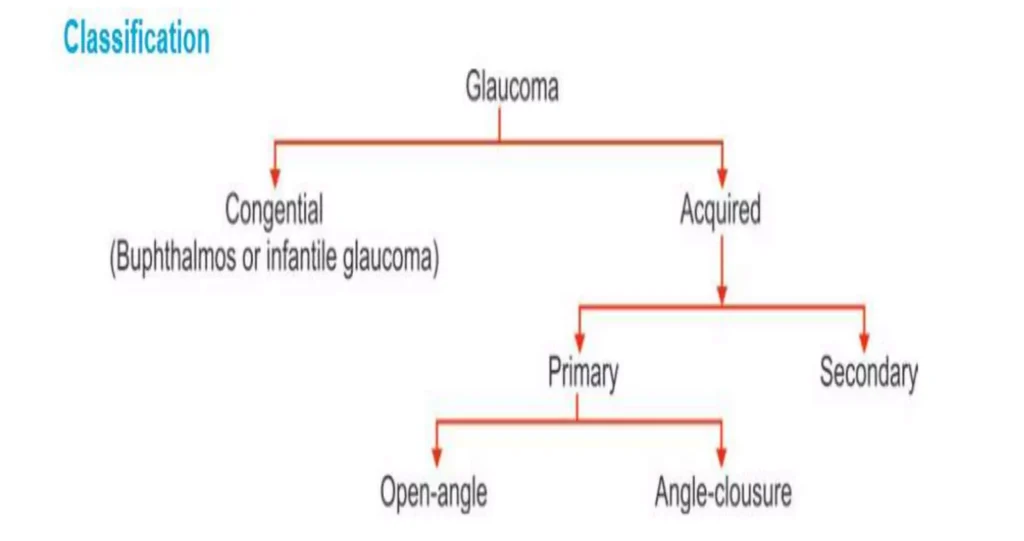
Classification of Glaucoma.
Glaucoma has been classified into specific types:

Congenital Glaucoma
Congenital glaucoma is a rare form of glaucoma that is present at birth or develops shortly after birth.
- It is characterized by abnormalities in the angle of anterior chamber obstructing the outflow of aqueous humour, leading to increased intraocular pressure and potential damage to the optic nerve.
- Congenital glaucoma can manifest at birth ( True Congenital) before 3 years ( Infantile) or between 3-16 years Juvenile).
Clinical Feature of Congenital Glaucoma.
- Age of onset: Congenital glaucoma presents in infants and young children, usually before the age of 3 years.
- Triad of symptoms: The classic triad of symptoms associated with congenital glaucoma includes :
- Watering (epiphora): Excessive tearing or watery eyes.
- Photophobia: Sensitivity to light.
- Blepharospasm: Involuntary contraction or twitching of the eyelids.
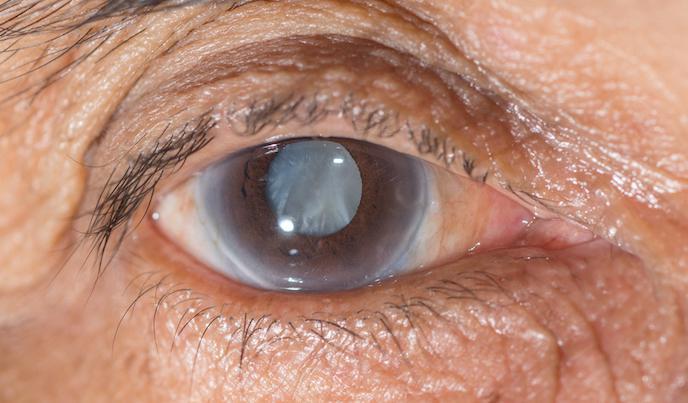
- Buphthalmos: Congenital glaucoma can cause enlargement of the eyeball, known as buphthalmos or “ox eye or bull’s eye” . This occurs due to increased intraocular pressure (IOP) and rapid expansion of the eye.
- Corneal changes: The elevated IOP in congenital glaucoma can lead to corneal enlargement and clouding. This can result in corneal edema and opacification, which may cause visual impairment.
- Haab striae: Horizontal or oblique breaks in Descemet membrane, known as Haab striae, can be seen in congenital glaucoma. These striae are a result of the stretching of the cornea due to increased IOP.
- Optic nerve damage: If left untreated or uncontrolled, congenital glaucoma can lead to optic nerve damage. This can result in vision loss.
- Variable presentation: The severity and presentation of congenital glaucoma can vary. Some cases may be unilateral (affecting one eye) while others may be bilateral (affecting both eyes).
- Blepharospasm (involuntary forceful closure of eyes): In congenital glaucoma, blepharospasm is a common clinical feature that refers to the involuntary and forceful closure of the eyelids.
- Excessive lacrimation: Excessive tearing or lacrimation is another common symptom of congenital glaucoma since the increased pressure in the eye can cause the tear ducts to produce more tears than usual.
- Enlarged and edematous cornea: The cornea, the clear front part of the eye, can become enlarged and edematous in congenital glaucoma. The increased pressure in the eye can lead to fluid accumulation in the cornea, causing it to swell which can result in cloudiness and opacification of the cornea.
- Thin and blue sclera: The sclera, the white outer layer of the eye, may appear thin and blue in congenital glaucoma, due to increased pressure in the eye. The blue color is due to the visibility of the underlying choroid layer through the thin sclera.
- Deep anterior chamber: Congenital glaucoma can cause a deepening of the anterior chamber, which is the space between the cornea and the iris. The increased pressure in the eye can push the iris backward, resulting in a deeper anterior chamber.
- Flat lens: In congenital glaucoma, the lens of the eye may appear flat. The increased pressure in the eye can affect the shape and position of the lens. This can lead to changes in the focusing ability of the eye.
- Optic disc atrophy: Optic disc atrophy, which refers to the degeneration and loss of nerve fibers in the optic disc, can occur in congenital glaucoma. The increased pressure in the eye can cause damage to the optic nerve.
Management of Congenital Glaucoma
The management of congenital glaucoma involves a combination of medical therapy and surgical interventions.
The main Aims of management is to lower intraocular pressure (IOP) and prevent further damage to the optic nerve.
Medical Therapy:
- Medical therapy is often used as a temporary measure to control IOP and clear the cornea before surgery.
- Medications such as topical beta-blockers like timolol, betaxolol, or prostaglandin analogs, and carbonic anhydrase inhibitors may be prescribed to reduce IOP.
Surgical Interventions:
1. Angle Surgery: The mainstay of treatment for congenital glaucoma is angle surgery, which aims to improve aqueous outflow and lower IOP.
- Goniotomy: In this procedure, an incision is made across the trabecular meshwork to improve drainage of aqueous humor.
- Trabeculotomy: This surgery involves incising the trabecular meshwork to create a new drainage pathway for aqueous humor.
2. Trabeculectomy: If angle surgery is not successful in controlling IOP, trabeculectomy may be performed. This procedure involves creating a new drainage channel to bypass the trabecular meshwork.
3. Glaucoma Implant Surgery: In cases where other surgical options fail, glaucoma implant surgery may be considered. This involves the placement of a drainage device, such as a Molteno, Baerveldt, or Ahmed implant, to regulate the flow of aqueous humor and lower IOP.
Follow-up and Monitoring:
- Regular follow-up visits with an ophthalmologist are essential to monitor IOP, assess the effectiveness of treatment, and detect any potential complications or disease progression.
- Ongoing management may involve adjustments to medication dosages, additional surgical interventions if necessary, and monitoring for potential long-term complications such as refractive errors or amblyopia.
ACQUIRED GLAUCOMA
Acquired glaucoma refers to glaucoma that develops later in life due to various factors such as age, genetics, underlying medical conditions, or trauma.
It is a chronic and progressive condition that requires ongoing management to control IOP and preserve vision.
It is further divided into;
PRIMARY GLUCOMA.
- Primary Open angle glaucoma.
- Primary angle closure Glaucoma
- Chronic angle closure glaucoma.
SECONDARY GLAUCOMA
- Lens induced glaucoma
- Glaucoma due to uveitis
- Neurovascular Glaucoma
- Glaucoma associated with intraocular tumor
- Steroid induced glaucoma.

PRIMARY OPEN-ANGLE GLAUCOMA (POAG)
Primary Open-Angle Glaucoma (POAG) also called as open angle glaucoma or chronic simple glaucoma or simple complex glaucoma results from the overproduction of aqueous humour through trabecular mesh work resulting into increased IOP and damage to optic nerve, resulting into loss of vision.
In this type there in no narrowing of the anterior chamber BUT there is resistance in the trabecular meshwork to aqueous flow resulting in gradual increase in IOP along with cupping of the optic disc and visual fields defects.
Predisposing factors for primary glaucoma include:
- Cigarette smoking.
- Diabetes Mellitus and Hypertension diseases.
- Myopia (nearsightedness).
- Old age.
Clinical features of primary glaucoma may include:
- Asymptomatic in the early stages.
- Mild headache and pain in the eye.
- Difficulty in reading.
- Delayed dark adaptation.
- Alteration in vision sites.
- Mild ache in the eyes
- Increased IOP ( more than24 mmhg)
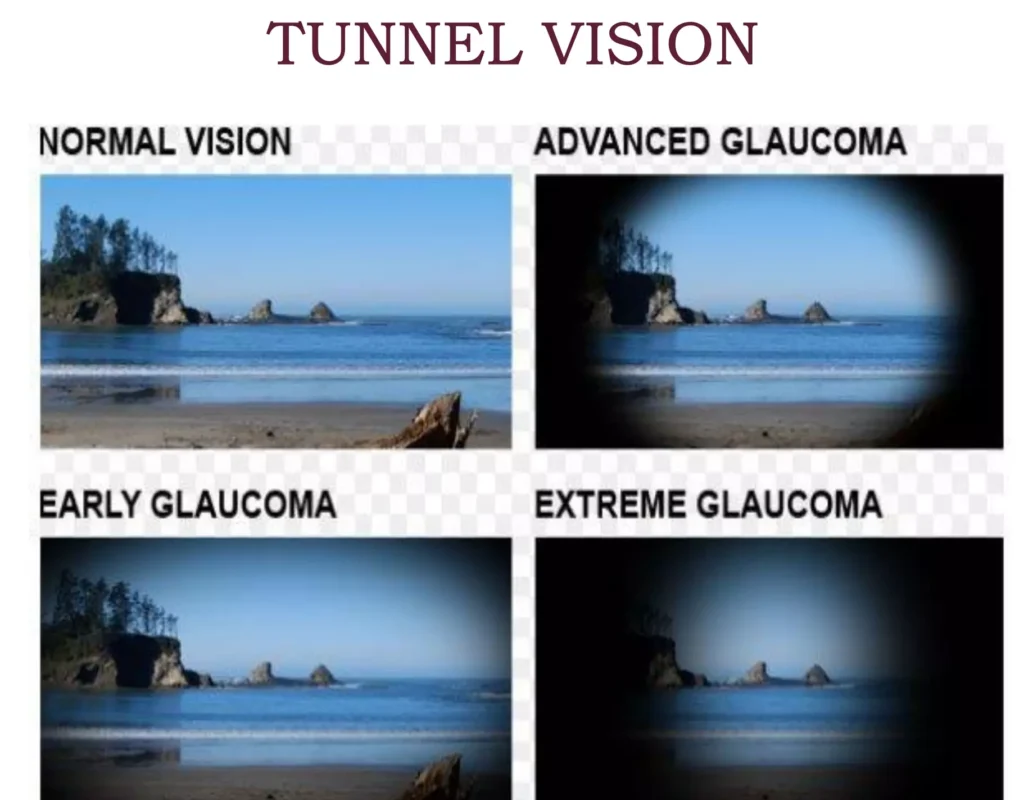
- Loss of Peripheral vision
- Reduced visual acquity at night.
- Corneal edema
- Visual field deficit.
Investigations for primary glaucoma include:
- Tonometry: To measure intraocular pressure (IOP). In glaucoma, IOP may remain permanently high in the late stages and fluctuating in the early stages.
- Gonioscopy: To assess the angle of the anterior chamber. Narrowing of the angle may be observed in glaucoma.
- Fundus examination: Done with the use of ophthalmoscopy and a slit lamp biomicroscope to look for disc changes.
- Perimetry: To assess changes in the visual field.
Treatment options for primary glaucoma include:
Medical treatment: This is the first choice for open-angle glaucoma.
- Topical beta blockers: These drugs lower the production of aqueous fluid, thereby reducing IOP. Examples include Timolol mealate: (2.5-5 mg B.D), Betaxolol 25mg B.D, Levabunolol 2.5-5% B.D it has a longer effect
- Dorzolamide(2%): It lowers IOP by decreasing the production of aqueous fluid.
- Latanoprost(0.5): It decreases the flow of aqueous fluid.
- Pilocarpine: It contracts the ciliary muscle and opens the trabecular meshwork, allowing increased outflow of aqueous humor.
- Adrenergic group: Drugs like epinephrine hydrochloride decrease aqueous production through vasoconstriction.
Surgical treatment: Surgery is considered when there is a failure to respond to maximal medical therapy.
- Laser therapy: Laser trabeculoplasty (ALT) may be performed if the patient does not respond to medical treatment
- Filtering surgery: Trabeculectomy is a surgical procedure that creates an opening in the white of the eye to allow fluid to leave the eye.
- Drainage tubes: Small tubes may be inserted in the eye to drain excess fluid and lower IOP.
- Minimally invasive glaucoma surgery (MIGS): These procedures have less risk and require less postoperative care compared to traditional surgeries


The os simplified and easily red
Thank you for the wonderful work done by providing us with the Note
Kindly we request you to produce books for easy accessibility
To put in the library for students to study
WOW the content is wonderful 👏 bravo, though it was so detailed but we appreciate your efforts, you have made Studying Nursing an Easy thing 😊