STINGS AND BITES
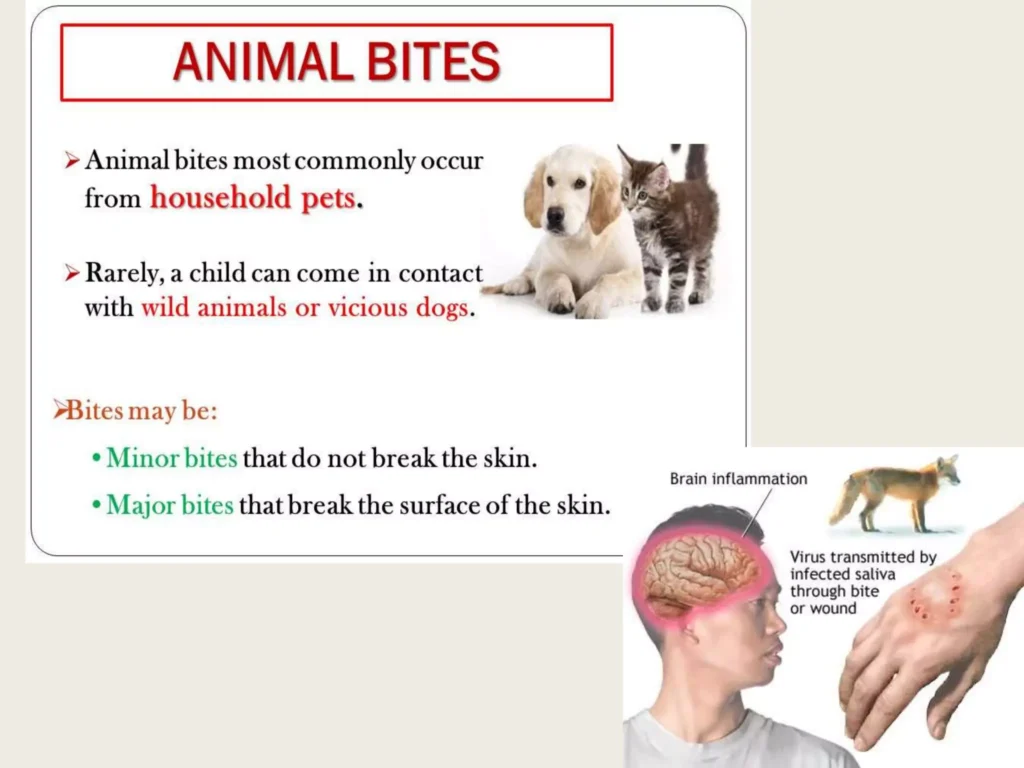
ANIMAL BITES
Animal bites, especially in children, are a common occurrence and can result in puncture wounds. It is important to properly manage these bites to prevent complications such as infection and the transmission of diseases like rabies.
General Wound Care:
- Rinse the wound with saline water or sterile water under pressure to remove any dirt or debris.
- Wash the surrounding skin with soap and water to reduce the risk of infection.
- Apply a clean dressing to protect the wound and promote healing.
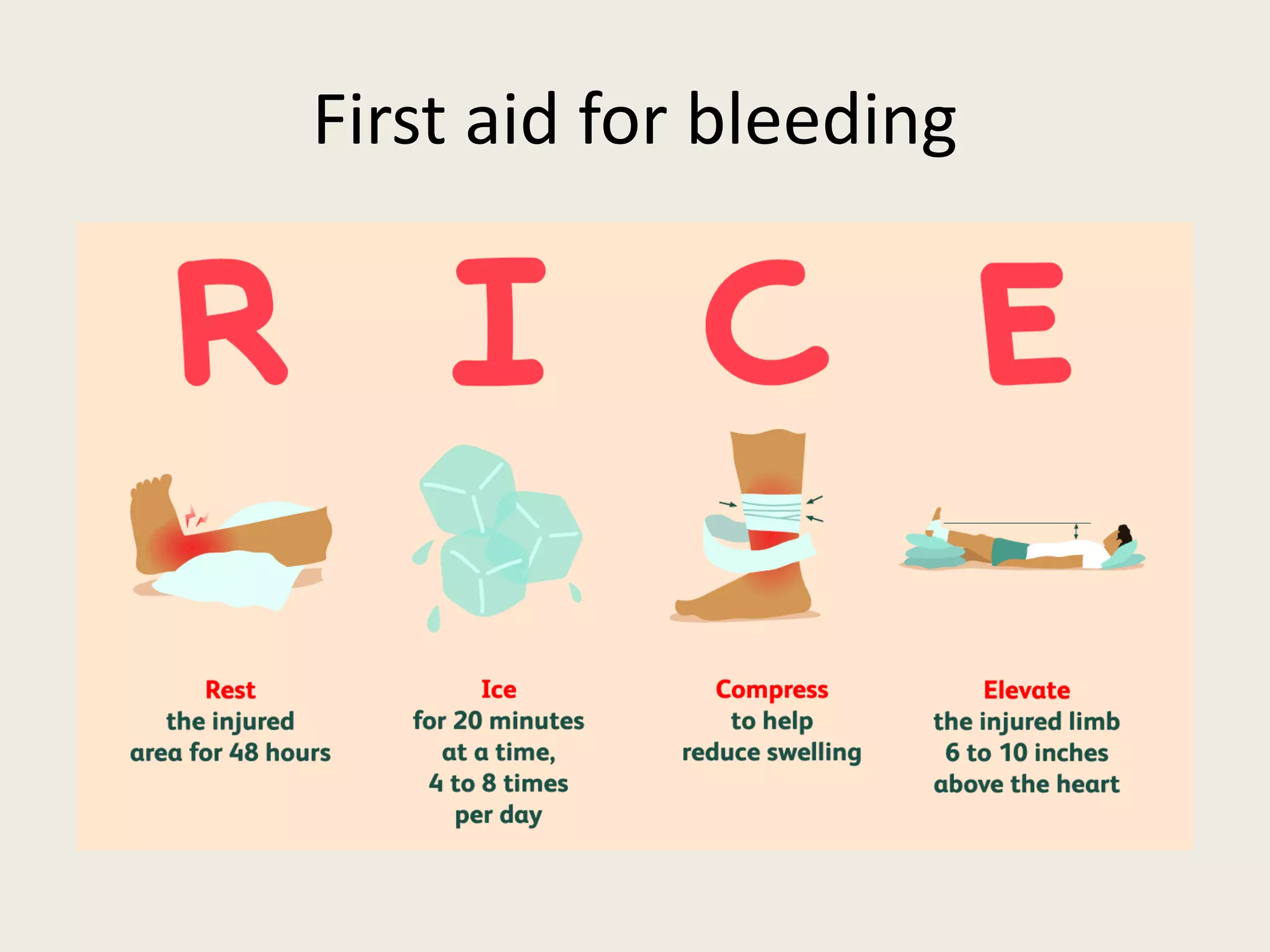
- If possible, elevate the affected body part to help control bleeding.
Medical Interventions:
- Tetanus toxoid should be administered if the person has not been adequately vaccinated against tetanus.
- Prophylactic antibiotics may be prescribed to prevent infection, especially in high-risk wounds or individuals with immune deficiencies.
- Debridement of lacerations may be necessary to remove damaged tissue and promote healing.
Suspected Rabies Infection:
- If there is a suspicion of rabies infection, immediate medical attention is crucial.
- Anti-rabies immunoglobulins, such as inactivated rabies vaccines, may be administered to induce an active immune response.
- Rabies Ig (preformed antibodies) may also be given to provide immediate protection against the virus.
Animal Safety:
- Teach children how to prevent interactions with unfamiliar animals.
- Vaccinate your pets regularly to protect them against diseases and reduce the risk of bites.
- Avoid teasing or provoking animals, as this can lead to aggressive behavior.
- Do not make direct eye contact with a threatened animal, as it may perceive it as a challenge.
- Never pull an animal’s tail or take away its food, as this can agitate them.
- Approach restrained animals with caution and respect their space.
- Avoid running in front of a dog, as it may trigger their instinct to chase.
- Do not allow inexperienced individuals to feed dogs, as they may not understand proper handling techniques.
- Alert animals to your presence before approaching them to avoid surprising or startling them.
- Consider spraying your pets with appropriate insect repellents to prevent bites from insects like fleas and ticks.
- Socialize your animals to ensure they are comfortable and well-behaved around people.
- Do not allow children to lead dogs, as they may not have the necessary control or understanding of the animal’s behavior.