Alcohol Abuse
ALCOHOLISM
Alcoholism is a chronic condition characterized by excessive and prolonged alcohol consumption, leading to severe physical, social, and mental adverse effects, and an increased physical and social dependency on alcohol.
Key Terms and Definitions:
- Drug (Substance): Any chemical agent that, once ingested, can cause physiological and psychological changes.
- Alcoholic: An individual who excessively consumes alcohol, leading to mental, social, physical, and psychological problems.
- Substance Intoxication: A reversible, substance-specific syndrome that develops due to recent ingestion or exposure to a drug.
- Alcohol Intoxication: A temporary mental disturbance following heavy drinking, where blood alcohol levels are high enough to affect activity, mood, and consciousness.
- Tolerance: The need for increasing amounts of a drug to achieve the same effect previously obtained with a lower dose.
- Dependency: A compulsion to continuously take a drug to experience its effects and avoid the discomfort of its absence. This can be physical (bodily response) or psychological.
- Addiction: A psychological and physical inability to stop consuming a drug despite it causing psychological and physical harm, characterized by continued use despite negative consequences.
- Misuse: Incorrect, excessive, or non-therapeutic use of mind-altering substances.
Causes of Alcohol Abuse:
- Availability: Easy access to alcohol and societal acceptance of drinking (e.g., at social gatherings).
- Genetic Factors: A family history of excessive drinking suggests a genetic predisposition.
- Poor Coping Strategies: Individuals struggling with stress may resort to alcohol as a coping mechanism.
- Psychiatric Disorders: Co-occurring conditions like depressive, anxiety, or phobic disorders can lead to alcohol abuse.
- Social Disorders: Factors such as isolation, unemployment, loss, bereavement, or injustice.
- High-Risk Groups: Includes those with chronic physical illnesses, business executives, traveling salespersons, industrial workers, hostel students, and military personnel.
- Age: Most common between late adolescence and early adulthood.
Process of Alcoholism:
The development of alcoholism often follows a progression:
- Experimental Stage: Initial consumption due to peer pressure, influences, or curiosity.
- Recreational Stage: Enjoyment of alcohol during weekends or holidays. In small amounts, it may relieve tension, relax the mind, or promote well-being.
- Compulsive Stage: Regular, heavy drinking to achieve pleasure or avoid withdrawal discomfort.
Stages of Alcoholism:
The text outlines distinct stages:
- Early Stage:
- Increased Tolerance: Needing more alcohol for the desired effect.
- Blackouts: Inability to recall events while intoxicated.
- Preoccupation: Constant thoughts about drinking.
- Middle Stage:
- Loss of Control: Inability to limit amount or frequency of drinking.
- Cycles of Abstinence: Brief periods without alcohol, followed by obsessive drinking.
- Chronic Stage:
- Low Tolerance: Getting drunk on small amounts.
- Prioritizing Alcohol: Alcohol takes precedence over family or job; willingness to lie, beg, borrow, or steal for supply.
Types of Drinkers:
- Mild Drinkers: Rarely and occasionally consume small amounts, or large amounts infrequently, with minimal problems.
- Moderate Drinkers: Consume in moderation, without excess, generally avoiding significant health issues.
- Problem Drinkers: Consume large amounts daily, often with high concentrations, leading to impaired health, mental distress, family disruption, loss of reputation, and poor performance.
Effects and Complications of Alcohol:
A. Physical or Medical Effects:
- Hepatitis and Liver Cirrhosis
- Pancreatitis
- Peptic Ulcers and Gastritis
- Cardiomyopathies and Heart Failure
- Epileptic-like Fits (RUM Fits - alcohol withdrawal seizures)
- Tuberculosis
- Weight Loss
- Alcoholic Dementia
- Anemia
- Malnutrition
- Lowered Immunity
B. Psychiatric Effects:
- Depression
- Pathological Intoxication: Maladaptive behavioral effects (e.g., fighting, impaired judgment, slurred speech, mood changes, irritability, impaired attention).
- Delirium Tremens (DTs): Severe withdrawal syndrome with confusion, hallucinations, and autonomic instability.
- Alcoholic Hallucinosis: Vivid hallucinations shortly after reducing or stopping alcohol.
- Alcoholic Psychosis: Psychotic disorder resembling paranoid schizophrenia (delusions, hallucinations, primary mental function impairment) after prolonged, heavy drinking.
- Alcohol Amnestic Disorder: Impairment in short and long-term memory, disorientation, and confabulation.
- Alcoholic Dementia: Chronic organic mental disorder resulting in irreversible memory and orientation impairment.
- Suicide
- Anxiety
- Paranoia: Persecutory ideation and self-hate.
- Morbid or Pathological Jealousy: Irrational jealousy, often directed at a partner.
- Hallucinations
- Wernicke’s Encephalopathy: Acute deficiency of Vitamin B1 (Thiamine) in alcoholics, causing neurological symptoms.
- Korsakoff Syndrome: Gradual depletion of thiamine, leading to severe memory problems and confabulation.
C. Social Problems:
- Decreased work performance and productivity (due to chronic absenteeism).
- Family problems (e.g., divorce).
- Increased accidents (e.g., drunk driving).
- Legal effects (e.g., rape, theft).
- Violence and aggression.
Diagnosis of Alcoholism:
- History Taking: Comprehensive assessment of upbringing, family background, duration of abuse, etc.
- Clinical Presentation: Observable signs like curly hair, swollen cheeks, red lips, poor hygiene, etc.
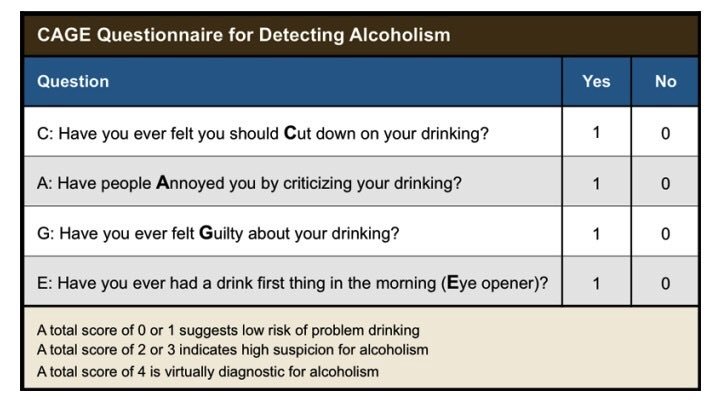
- CAGE Questionnaire: A screening tool:
- C - Have you ever felt you should Cut down on your drinking?
- A - Have people Annoyed you by criticizing your drinking?
- G - Have you ever felt Guilty about your drinking?
- E - Have you ever had an Eye-opener first thing in the morning to get rid of a hangover or calm your nerves?
- Interpretation: Two or more "yes" answers are highly suggestive of alcoholism.
Concentration of Alcohol in Blood and Effects:
- 80-150 mg/100ml: Intoxication
- 150-300 mg/100ml: Fatal (high risk of death)
- 300-500 mg/100ml: Very Fatal (extremely high risk of death)
- 500 mg/100ml and above: Leads to death
- Note: These effects can vary based on individual tolerance.
Management of Alcoholism:
A. Aims of Management:
- Detoxify the patient (in acute stages).
- Improve social relationships and support.
- Develop confidence and ability to change.
- Identify reasons for change.
- Develop alternative activities.
- Learn to prevent relapse.
B. Admission:
- Hospitalization is crucial to prevent alcohol access; often 6-8 weeks initially.
- Admit to a psychiatric hospital in a well-lit, quiet, open room to reduce fear and illusions.
- Establish a good nurse-patient relationship.
- Remove potentially harmful objects to prevent self-harm.
- Keep the bed dry, clean, and warm due to possible incontinence.
- Monitor vital signs every 15 minutes initially, including physical and mental behavior.
- Investigations: Urine for sugar, blood for hemoglobin level and sugars, blood alcohol level.
C. Medication:
- Minor Tranquilizers (Anxiolytics): Librium (chlordiazepoxide) and Diazepam (Valium) parenterally for anxiety, insomnia, agitation, and tremors (these are benzodiazepines, crucial for withdrawal management).
- Anticonvulsants: For withdrawal seizures ("rum fits").
- Vitamins: Plenty of B vitamins (especially Thiamine B1, B6, B12 – 100-300mg BID for 7 days), B complex, and Vitamin C.
- Antacids: To relieve gastritis.
- Fluid & Electrolyte Correction: Intravenous infusions, fluid balance chart.
- Disulfiram (Antabuse): Administered under close supervision. It causes severe adverse reactions (nausea, vomiting, headache, palpitations, blurred vision, hypotension, dyspnea) if alcohol is consumed. Initial dose 1g, tapering down to 0.1g for maintenance (up to a year).
- Aversion Therapy (Apomorphine): Injectable emetic; causes vomiting when alcohol is smelled. The text notes this is discouraged.
- Yeast Tablets: Twice daily to induce appetite.
- Stemetil (Prochlorperazine) / Avomine (Promethazine): 5-10mg to control vomiting.
- Sedation: May be required.
- Avoid Barbiturates: Alcoholics can easily become addicted to them.
D. General Nursing Care:
- Treat Associated Conditions: Address malnutrition, vitamin deficiencies, hallucinations, delirium, gastritis, or liver diseases.
- Nutrition: Small, frequent, nutritious, and appetizing meals.
- Hygiene: Oral care, general body, and bed hygiene.
- Nurse-Patient Relationship: Acceptance by the nurse is essential to encourage socialization and participation, reducing inferiority and low self-esteem.
- Psychiatric Social Workers: Involvement in addressing social problems.
- Religious Commitment: Encouraged.
- Familial Therapy: Encouraged to help the patient stay sober.
- Social Circle Change: Encourage changing friends and associates to remove triggers.
- Alcoholics Anonymous (AA): Prepare the patient for AA, a self-help group where ex-addicts provide mutual support and guidance for sobriety.
- Discharge Planning: Plan for the patient's discharge and resettlement into the community.
Therapeutic Modalities for SUDs
Therapeutic modalities form the backbone of behavioral treatment for Substance Use Disorders (SUDs). They address the psychological, social, and behavioral aspects of addiction, helping individuals develop coping strategies, improve interpersonal relationships, and maintain abstinence.
I. Individual Therapies
Individual therapy provides a private and confidential setting for patients to explore their substance use, underlying issues, and recovery goals with a trained therapist.
- Core Principle: Based on the idea that thoughts, feelings, and behaviors are interconnected. CBT helps patients identify and change problematic thinking patterns and behaviors that contribute to substance use.
- Techniques:
- Identifying Triggers: Recognizing situations, thoughts, or feelings that lead to craving and substance use.
- Coping Skills Training: Developing healthy ways to manage stress, cravings, and high-risk situations (e.g., relaxation techniques, distraction, problem-solving).
- Relapse Prevention: Learning to anticipate and cope with potential setbacks, developing a plan for managing a "slip."
- Cognitive Restructuring: Challenging and changing irrational or unhelpful thoughts (e.g., "I can't cope without alcohol").
- Role in SUDs: Highly effective for many SUDs, helping patients develop self-control and build skills for long-term recovery.
- Core Principle: Developed for individuals with severe emotion dysregulation (originally for Borderline Personality Disorder), but highly effective for SUDs, especially when co-occurring with trauma or personality disorders. Emphasizes balancing acceptance and change.
- Skills Modules:
- Mindfulness: Learning to be present and aware without judgment.
- Distress Tolerance: Developing strategies to cope with intense emotions and crises without resorting to substance use or other maladaptive behaviors.
- Emotion Regulation: Learning to identify, understand, and manage intense emotions.
- Interpersonal Effectiveness: Improving communication skills and building healthier relationships.
- Role in SUDs: Helps patients manage intense cravings, cope with emotional triggers, and develop healthier interpersonal boundaries.
- Core Principle: A person-centered, directive method for enhancing intrinsic motivation to change by exploring and resolving ambivalence.
- Key Elements (OARS):
- Open-ended questions: Encourage detailed responses.
- Affirmations: Recognize patient strengths and efforts.
- Reflective listening: Show understanding and empathy.
- Summaries: Consolidate understanding and highlight key points.
- Role in SUDs: Often used as an initial intervention to help patients move from precontemplation/contemplation to preparation/action stages of change, increasing readiness for treatment. Nurses frequently use MI techniques.
- Core Principle: Explores unconscious conflicts, past experiences (especially childhood trauma), and relationship patterns that may contribute to substance use.
- Role in SUDs: May be useful for individuals whose substance use is deeply rooted in unresolved psychological issues, often as a long-term approach.
II. Group Therapies
Group therapy provides a supportive environment where individuals can share experiences, receive feedback, and learn from peers in recovery.
- Focus: Provide information about SUDs, relapse prevention, coping skills, and healthy lifestyle choices.
- Role in SUDs: Informative and foundational for understanding the disease and recovery process.
- Focus: Explore interpersonal dynamics, emotions, and behaviors within the group setting. Members provide support and challenge each other.
- Role in SUDs: Helps individuals develop social skills, address isolation, and practice new behaviors in a safe environment.
- Focus: Utilize CBT principles to identify high-risk situations, develop coping strategies, and review relapse warning signs.
- Role in SUDs: Critical for maintaining long-term abstinence by equipping patients with proactive strategies.
III. 12-Step Programs
(e.g., Alcoholics Anonymous (AA), Narcotics Anonymous (NA))
- Core Principle: A mutual-help, peer-led program based on spiritual principles (though not necessarily religious). Emphasizes abstinence, working through the 12 steps, making amends, and service to others.
STEPS OF ALCOHOLICS ANONYMOUS:
- We admitted we were powerless over alcohol – that our lives had become unmanageable. AA firmly believes that individuals cannot overcome alcoholism on their own. They are unable to exercise willpower or personal strength that could prevent them from drinking
- Came to believe that a Power greater than ourselves could restore us to sanity. Alcoholics Anonymous is based on the belief in a higher power. For some, this higher power may be God; for others, it may be a belief in the universe itself. The point is that recovery begins, in part, by looking to an entity greater than yourself.
- Made a decision to turn our will and our lives over to the care of God as we understood Him.
- Made a searching and fearless moral inventory of ourselves. During this step, many participants make a list of poor decisions or character flaws. They outline hurt they caused to others, as well as feelings, like fear and guilt, that motivated some of their past actions. Once the individual has acknowledged these issues, the issues are less likely to serve as triggers to future alcohol abuse.
- Admitted to God, to ourselves and to another human being the exact nature of our wrongs. As AA members work this step, they sit down with someone – often their sponsor – and confess everything they identified in Step 4. This step requires the recovering individual to put aside their ego and pride to acknowledge shameful past behavior. The step is also empowering, as the alcoholic no longer has to hide behind guilt and lies.
- Were entirely ready to have God remove all these defects of character. In this step, the recovering alcoholic acknowledges that he or she is ready to have a higher power – again, whatever that may be – take away the moral shortcomings identified in
- Humbly asked Him to remove our shortcomings. This step requires the person to focus on the positive aspects of his or her character – humility, kindness, compassion and a desire for change – as well as step away from the negative defects that have been identified.
- Made a list of all persons we had harmed, and became willing to make amends to them all. During this step, recovering alcoholics write down a list of all the people they have hurt. Often, this list includes people they hurt during their active alcoholism; however, it may go back further to include anyone they have hurt throughout their entire lives
- Made direct amends to such people wherever possible, except when to do so would injure them or others. Paired with Step 8, Step 9 gives recovering alcoholics the opportunity to make things right with those they have hurt. One’s sponsor can be a big source of help during this process, helping the recovering alcoholic to determine the best way to go about making amends.
- Continued to take personal inventory and when we were wrong promptly admitted it. Linked to Step 4, this step involves a commitment to continue to keep an eye out for any defects of character. It also involves a commitment to readily admit when one is wrong, reinforcing humility and honesty.
- Sought through prayer and meditation to improve our conscious contact with God as we understood Him, praying only for knowledge of His will for us and the power to carry that out. Step 11 commits the recovering alcoholic to continued spiritual progress. For some, this may mean reading scripture every morning. For others, it may mean a daily meditation practice. Alcoholics Anonymous doesn’t have stringent rules on what form spiritual growth takes. It simply involves a commitment to take time to reassess one’s spiritual and mental state.
- Having had a spiritual awakening as the result of these steps, we tried to carry this message to alcoholics and to practice these principles in all our affairs practice these principles in all our affairs. The final step involves helping others and serves as motivation for many to become sponsors themselves. By going through the 12 steps, individuals have a major internal shift and part of that shift is a desire to help others.
IV. Family Therapy
- Core Principle: Recognizes that SUDs affect the entire family system. Focuses on improving family communication, establishing healthy boundaries, and addressing enabling or dysfunctional patterns.
- Approaches:
- Family Behavioral Therapy (FBT): Focuses on teaching family members communication skills, problem-solving, and contingency management to support the patient's recovery.
- Multisystemic Therapy (MST): Intensive, family- and community-based treatment for adolescents with serious substance use and other behavioral problems.
- Role in SUDs: Essential for healing family dynamics, creating a supportive home environment, and preventing relapse. It also provides support and education for family members, who often suffer secondary effects of the SUD.
V. Other Emerging Therapies
- Mindfulness-Based Relapse Prevention (MBRP): Integrates mindfulness practices with CBT for relapse prevention.
- Contingency Management (CM): Uses positive reinforcement (e.g., vouchers, prizes) to reward abstinence and treatment adherence. Highly effective, especially for stimulant use, but can be resource-intensive.
VI. Nursing Role in Therapeutic Modalities
- Referral: Identify appropriate therapeutic modalities based on patient needs and preferences, and facilitate referrals.
- Support: Encourage participation in therapy and support groups.
- Integration: Reinforce therapeutic concepts (e.g., coping skills, trigger identification) in daily interactions with patients.
- Psychoeducation: Provide basic information about different therapy types and what to expect.
- Advocacy: Advocate for access to these vital services.