CONFLICT RESOLUTION
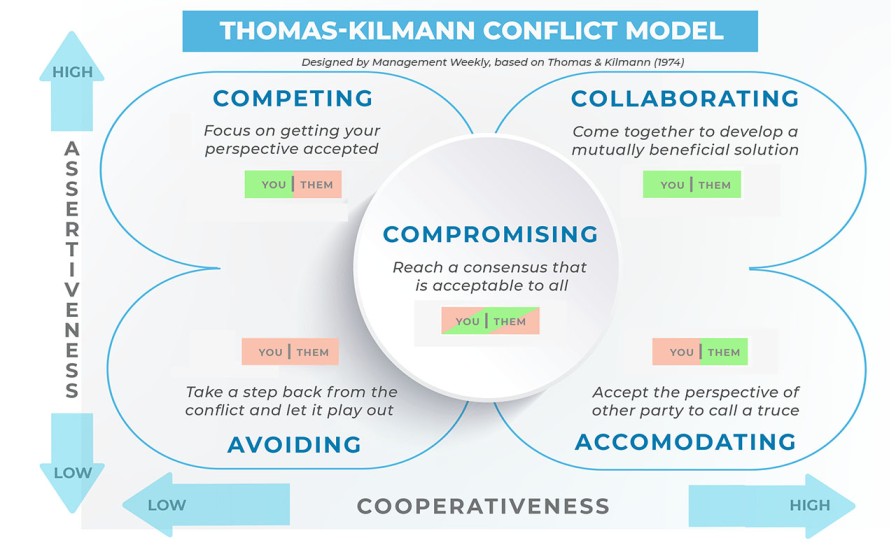
The conflict resolution styles.
1. Competition.(win-lose situation);
Take a firm stand, and know what you want. Operate from a position of power, drawn from things like position, rank, expertise, or persuasive ability. This style can be useful when;
- There is an emergency and a decision needs to be made fast.
- The decision is unpopular.
- Defending against someone who is trying to exploit the situation selfishly.
However it can leave people feeling bruised, unsatisfied and resentful when used in less urgent situations.
2. Collaboration(win-win situation);
Try to meet the needs of the parties involved. Be highly assertive, cooperate effectively and acknowledge that everyone is important. This style is useful
- When you need to bring together a variety of viewpoints to get the best solution.
- When there have been previous conflicts in the group.
- When the situation is too important for a simple trade-off.
3. Compromising:(lose-lose situation);
Try to find a solution that will at least partially satisfy everyone. Everyone is expected to give up something. Compromise is useful,
- When the cost of conflict is higher than the cost of losing ground.
- When equal strength opponents are at a standstill.
- When there is a deadline looming.
4. Accommodating:(lose-win situation);
This style indicates a willingness to meet the needs of others at the expense of the person’s own needs. The accommodator often knows when to give in to others, but can be persuaded to surrender a position even when it is not warranted. This person is not assertive but is highly cooperative. Accommodation is appropriate,
- When the issues matter more to the other party.
- When peace is more valuable than winning.
- When you want to be in a position to collect on this “favour” you gave.
However people may not return favours, and overall this approach is unlikely to give the best outcomes.
5. Avoidance (lose-lose situation);
Seek to evade the conflict entirely, delegate controversial decisions, accept default decisions, and don’t hurt anyone’s feelings. This style can be appropriate,
- When victory is impossible.
- When the controversy is trivial.
- When someone else is in a better position to solve the problem.
However in many situations this is a weak and ineffective approach to take.
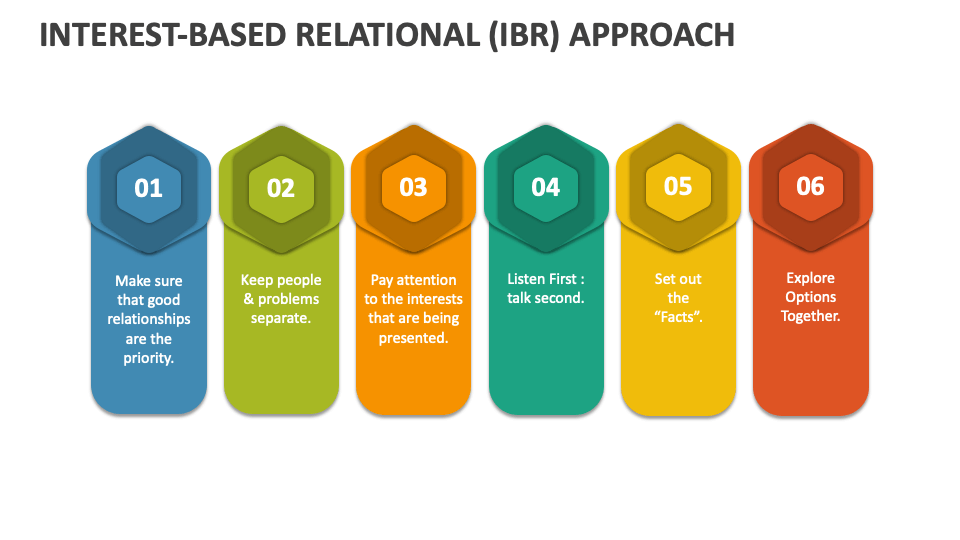
Interest-Based Relational Approach
The Interest-Based Relational Approach (IBRA) is a collaborative conflict resolution method that focuses on building relationships and understanding the underlying interests of all parties involved. It aims to find solutions that meet the needs of everyone involved while preserving and strengthening relationships. It involves;
- Making sure that good relationships are the first priority.
- Keeping people and problems separate
- Paying attention to the interests that are being presented.
- Listening to what both parties have to say.
- Set out the facts
- Explore options and solutions together.
Remember these,
- Assure privacy
- Empathize than sympathize
- Listen actively
- Maintain equity
- Focus on issue, not on personality
- Avoid blame
- Identify key theme
- Re-state key theme frequently
- Encourage feedback
- Identify alternate solutions
- Give your positive feedback
- Agree on an action plan
CONFLICT RESOLUTION Read More »