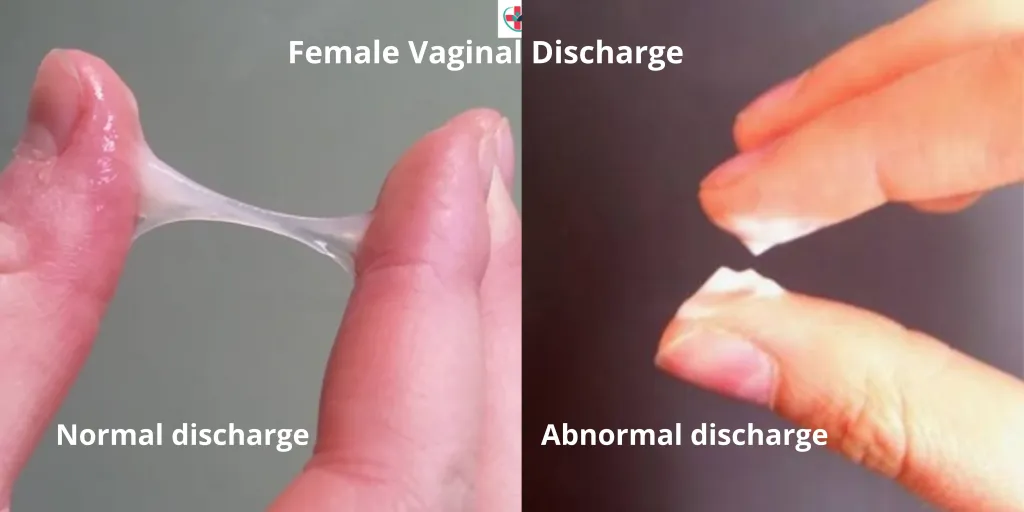
Abnormal Vaginal Discharge Syndrome
Management:
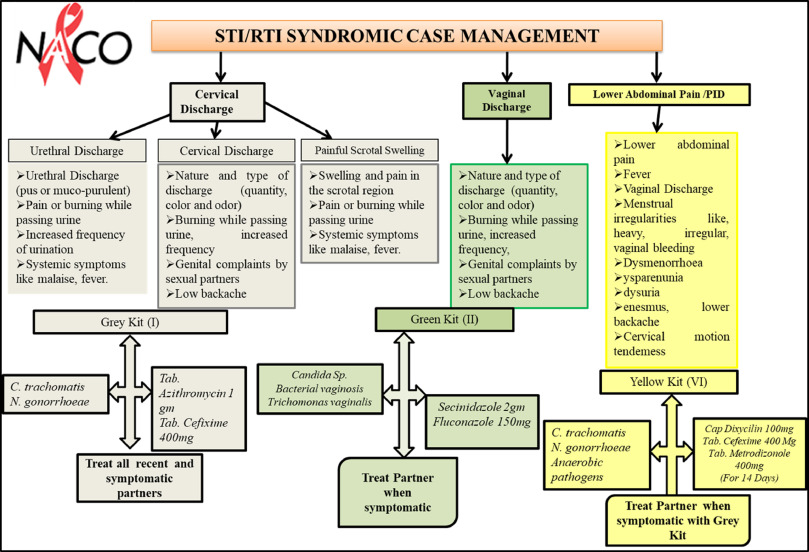
Women with vaginal discharge should be managed according to the flow chart. The flow chart differentiates between candidiasis and other vaginal discharges.

However, all women with abnormal vaginal discharge are treated for bacterial vaginosis and trichomoniasis and candidiasis. At the moment, it is not possible in this country to identify women with cervicitis, and all women with a non- curd like discharge should be treated for cervicitis.
Management Protocol for Abnormal Vaginal Discharge Syndrome:
Initial Assessment:
- Conduct a thorough history and examine for genital ulcers and abdominal tenderness.
- Perform speculum examination to check for cervical lesions.
- Assess the risk for sexually transmitted diseases.
Lower Abdominal Tenderness with Sexual Activity:
- If lower abdominal tenderness is present and the individual is sexually active, treat as per Pelvic Inflammatory Disease (PID) guidelines.
Thick, Lumpy Discharge with Itching and Erythema/Excoriations (Likely Candida):
- Administer Clotrimazole pessaries 100 mg: Insert high in the vagina once daily before bedtime for 6 days or twice daily for 3 days.
- Alternatively, prescribe Fluconazole 200 mg tablets as a single oral dose.
- Consider Metronidazole 2 g stat dose if indicated.
Abundant/Smelly Discharge (Possible Trichomonas or Vaginosis):
- Prescribe Metronidazole 2 g stat dose.
Purulent Discharge, High STD Risk, or Previous Ineffective Treatment:
Treat for Gonorrhea, Chlamydia, and Trichomonas:
- Cefixime 400 mg stat or Ceftriaxone 1g IV stat.
- Doxycycline 100 mg 12 hourly for 7 days.
- Metronidazole 2 g stat dose.
- If pregnant, replace Doxycycline with Erythromycin 500 mg every 6 hours for 7 days or Azithromycin 1 g stat.
- Ensure partner treatment.
Persistent Discharge or Dysuria Despite Partner Treatment:
- Refer the individual for further management.
Key management points include:
Treatment for Vaginal Infections:
- All women are treated for bacterial vaginosis, trichomoniasis, and candidiasis.
- Identification of cervicitis is challenging; hence, all women with non-curd-like discharge are treated for cervicitis.
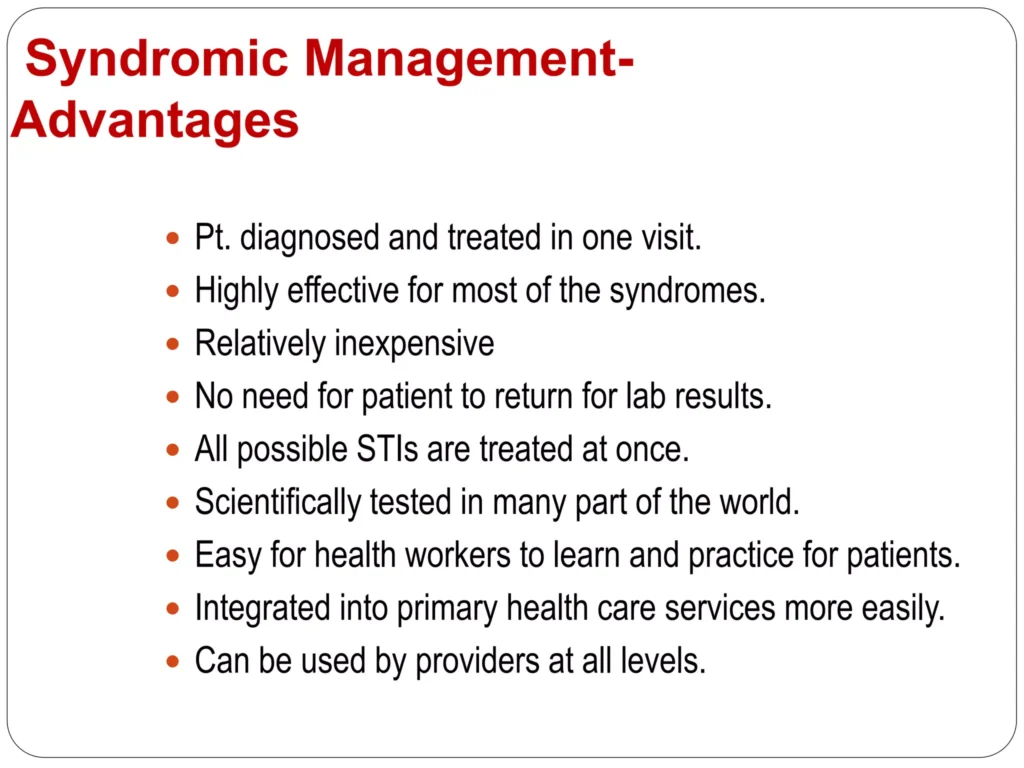
Promotion of Syndromic Management Package:
- Encourage adherence to comprehensive STI management, including partner treatment, preventive measures, and health education.
Communication:
- Explain the endogenous and recurrent nature of vaginitis to patients to prevent marital discord.
- Partners with urethral discharge should be treated for cervicitis.
Evaluation and Referral:
- Persistent abnormal vaginal discharge warrants evaluation to exclude cervical cancer.
- Speculum examination and referral for specialist management may be necessary.
Counsel and educate all clients on:
- Treatment compliance.
- Condom use and provide condoms.
- Partner management.
- Offer or refer for HIV VCT services if necessary.
- Schedule a return visit.
- Abstaining from sex till symptoms resolve.
Abnormal Vaginal Discharge Syndrome Read More »