Questions and Answers
Questions and Answers
Medicine
Hyperglycemia
- Mrs. Loyce a thirty three year old female patient has been admitted with signs and symptoms of hyperglycemia.
(a). Manage Loyce from the time of her admission up to discharge.
(b) Differentiate between hyperglycemia and hypoglycemia.
(c) Explain how you can prevent a diabetic foot.
SOLUTIONS
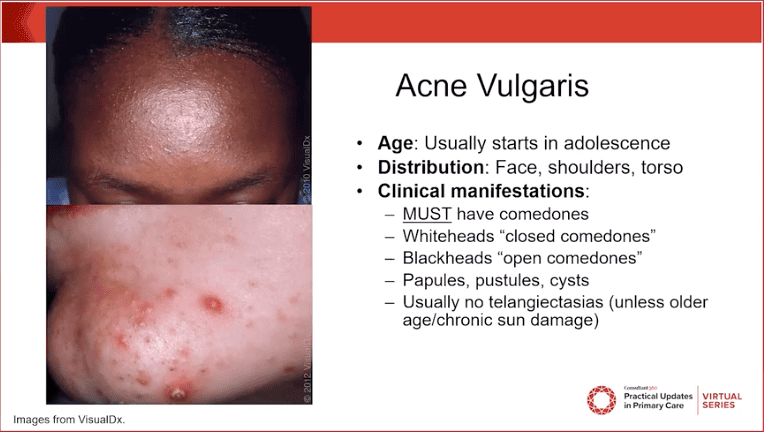
a). Hyperglycemia– refers to chronically high blood glucose level .it is usually over 240mg/dl.
Hypoglycemia– refers to dangerously low blood glucose levels that drop below 70mg/dl
However the sign and symptoms of hyperglycemia includes:-
- Blood glucose over 240mg/dl
- More urine output than normal
- Increased thirst (polydipsia)
- Dry skin and mouth (dehydration)
- Nausea and vomiting
- Decreased appetite
- Easy fatiquability ,drowsiness or no energy
Management of Loyce from the time of admission up to discharge
Aims of management
- To reduce blood glucose level to normal
- To prevent further complication
- To provide basic nursing care
- To alley anxiety
ACTUAL MANAGEMENT
- Mrs. Loyce is received in female medical ward given a seat and rapport created to alley anxiety
- Brief history taking of the patient’s condition including the demographic data
Admission
- The patient is admitted in female medical ward in a clean admission bed with clean linens in a well lit room free from dust and well ventilated
Position
- The patient adopts any comfortable position under nurse’s supervision
Observations
- Vital observations .temperature, pulse respiration and blood pressure of the patient are taken and recorded in the observation chart. So that incase of any deviation from normal, it can be managed appropriately.
- Specific observations .this includes observing the patient for jaundice, anemia ,cyanosis, clubbing, oedema, lymphadenitis, dehydration, urine colour and smell. Findings recorded and reported to the doctor.
General observation
- This is done from head to toe to rule out any abnormalities.
Inform the doctor: As soon as the observations are done the doctor is informed who will come and carry out his assessments (confirm the nurses findings) and may order for the following investigations
Investigations
- Specific investigations
- Haematology
-Blood for random blood sugar
– Renal function test
– Complete blood count
– Blood electrolytes
- Urinalysis to rule out presence of acetone & ketones, urine protein, blood in urine etc
- b) General investigations
– HIV serology
– When results are out, the doctor makes a diagnosis and may prescribe the following supportive treatment
- Intravenous fluids normal saline 3 liters while monitoring blood pressure until blood glucose level is lowered to normal
- Insulin administered intradermal .it can be pre-breakfast or pre- supper depending on doctor’s prescription
- Antibiotics e.g. ceftriaxone 2g in case of any sign of infections
Specific nursing care
- Diet. -The patient is given low sugar diet ,low fats diet and diet rich in vitamins
- Elimination. – Bladder is monitored for urine output using the fluid balance chart (FBC) and recorded on the chart.
- Bowel. Patient is encouraged to empty the bowel whenever necessary
- Exercise:- passive exercise in acute state eg massaging the patients toes and fingers to aid circulation
- Active exercise e.g. deep breathing exercise to prevent hypostatic pneumonia, lower limbs to prevent DVT, the patient is encouraged to move around the ward
General nursing care
- Rest and sleep by restricting number of visitors and noise in the room should be minimized
- Personal hygiene e.g. skin care, oral care and bed linens changed whenever it is soiled.
- Environmental hygiene of the ward .the ward should be maintained clean and free from horrible dour that may discomfort the patient
- Psychotherapy e.g. the nurse allows relatives to stay with the patient and also may invite religious leaders who may update the patients spiritually
Investigations before discharge.
When the patient’s condition has improved, the doctor may order for investigations like:-
- Urinalysis
- Blood for blood sugar & CBC
- Renal function test
When the results are satisfactory, the doctor writes a discharge form and the patient is discharged
Advice on discharge
- Take medications as prescribed
- Come back for review on the schedule date
- Avoid injuries that can cause damage to the skin
- The patient is advised on diet as follows
- Food with reduced sugar
- Fatty food should be limited
- Diet should contain vitamins
- Improve on life style for example cessation of smoking ,alcoholism etc.
- Differences between hyperglycemia and hypoglycemia
Hyperglycemia | Hypoglycemia |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
- Prevention of diabetic foot
Diabetic foot is a neurological condition that occurs during diabetes. However, it can be prevented from occurring through the following ways:-
- Maintain and keep the blood glucose level low in a target range to prevent complications by administering insulin and advising on diet for example reduce on intake of sugar and fatty foods
- Examine and screen the patient’s feet daily for senses, colour, cuts, swelling, pain and temperature for early interventions incase of any.
- Wash and dry feet paying much attention between the toes.
- Turn the patient 2 hourly to prevent excessive pressure on the pressure areas of the foot to prevent pressure sores
- Wash and dry feet paying much attention between the toes.
- Turn the patient 2 hourly to prevent excessive pressure on the pressure areas of the foot to prevent pressure sores
- Wear for the patient shoes and stockings to prevent injury to the feet .the shoes should be of appropriate size. Always check the shoes before wearing.
- Trim the patients nail. This is done using the nail file to prevent under growing nails that can cause infections.
- Keep the skin soft and smooth by rubbing the skin with lotion over the top and bottom to prevent cracks
- Massage the feet to maintain blood circulation and the patient is encouraged not to cross the legs for long time because this can cut off circulation for the feet
- Protect the feet from cold and hot water since this can impair the senses
- Exercise the foot by moving it for about 5 minutes and teach the patient how to do it (physiotherapy)
Health educate the patient (Loyce) on the following;
- Importance of wearing a well fitting pair of shoes
- Not to move bare foot
- Check her foot before putting on shoes
- Seek medical assistance in case of any injury
- Put on gumboots incase of farming activities
Pulmonary Tuberculosis
2. Joseph an adult patient has been diagnosed with pulmonary tuberculosis.
(a) Outline ten signs and symptoms of PTB.
(b) Describe his management using nursing process from the time of admission up to discharge.
(c) List five complications of TB.
SOLUTIONS
Tuberculosis (TB)
This is a chronic lung disease caused by a bacillus called mycobacterium of the genus mycobacterium tuberculosis.
It can also occasionally be caused by other strains of mycobacteria including mycobacterium bovis which is found in animals.
TB is of two types;
- Pulmonary TB
- Extra pulmonary TB
PULMONARY TB:
Type of TB that affects mainly the lungs and is the most common type of TB.
SIGNS AND SYMPTOMS.
- Fever and chills
- Night sweats
- Productive or non productive cough
- Weight loss
- Fatigue
- Cough for more than 3 weeks.
- Coughing up blood (Haemoptysis)
- Chest pain
- Significant figure clubbing may occur
- Lymphdenopathy which is a sign of bacterial infection.
- Aneroxia
- Insomnia
ASSESSMENT | NURSING DIAGNOSIS | PLAN/GOAL∕EXPECTED OUTCOME | INTERVENTION OR IMPLEMENTATION | RATIONALE | EVALUATION |
Chest Pain | A cute chest pain related to inflammatory response secondary to disease process as evidenced by patient coughing out blood and reporting pain. | Relieve pain within 24 hours.
Patient will be free from pain until discharge. | Admit the patient on the medical ward specifically the TB unit.
Take vital observations i.e. TPRIBP and weight.
Position the patient in sit up position.
Re-assure the patient. Inform doctor to prescribe drugs and order for investigations.
Administer prescribed analgesics like 1m diclofenac 75mg stat then later tabs paracetamol 1g tds x 3/7. | For proper management
As baseline and for future reference.
To relieve pressure of the abdominal organs onto the diaphragm.
To allay the patient’s anxiety
For proper assessment and management of the patient.
To relieve pain. | Goal met, patient was relieved from pain after 24 hours and patient was free from pain at discharge. |
Cough | Altered respiratory patterns related to disease process as evidenced by patient having cough for more than 3 weeks. | Patient will have normal respiratory patterns until discharge. | Maintain the patient in the sit up position.
Do investigations as ordered.
Do sputum analysis and chest x – ray, erythrocyte sedimentation rate (ESR).
Complete blood count (CBC)
Administer prescribed anti TB drugs and give the right regimen (6EHRZ + 2EH)
Administer prescribed supportive drugs like multi-vitamins i.e. Folic acid | For comfortibility.
To confirm the causative agent and to rule out the involvement of other organs like the heart and complications.
To help in the re-epithelialisation and boost the patient’s appetite.
To destroy the causative organism | Goal met, patient reports normal respiratory patterns until discharge. |
Fever | Altered thermoregulation / body temperature related to disease process as evidenced by the patient hot on touch also the patient reporting fevers for the last 3 weeks. | To normalize the body temperatures wit in 24 hours and maintain within normal ranges until discharge. | Expose the patient.
Tepid sponge the patient.
Maintain the already prescribed antipyretics.
Take temperature 4 hourly until discharge. | To allow cool air to reach the patient’s skin.
To cool the external body.
To act on the temperature regulating centres in the brain.
As baseline and for future comparison. | Goal met, patient’s temperatures normalized after 24 hours and the patient’s temperatures were maintained with in the normal ranges till discharge. |
Weight loss | Altered nutrition less than body requirements related to loss of appetite as evidenced by the patient reporting having lost weight for the last 3 weeks or months. | To nourish the patient throughout his stay on the ward. | Encourage nourishing diet.
Encourage oral care and continue with prescribed multi-vitamins. | To nourish the patient.
To boost the patient’s appetite. | Goal met, patient was well nourished at discharge. |
Fatigue | Activity intolerance related to disease process as evidenced by patient unable to perform activities of daily life. | Patient will perform activities of daily living throughout his stay on the ward. | Encourage patient to carryout activities of daily living such as bathing, eating, toileting, oral care and going to the urinals by himself | To improve on patient’s general hygiene and improve on the appetite
To avoid complications that may arise as a result of over staying in bed. | Goal met, patient is able to perform activities of daily living at discharge. |
Insomnia | Altered sleeping patterns related to night sweats and irritating cough secondary to disease process as evidenced by the patient reporting not sleeping well. | Patient will have normal sleeping patterns during his stay on the ward. | Minimize noise and visitors on the ward.
Switch off light (bright lights)
Administer prescribed sedatives like tabs diazepam 5mg OD or PRN
Continue re-assuring the patient. | To enable the patient have enough rest. To induce sleep. To alley patient anxiety |
COMPLICATIONS ARE;
- Plueral effusion
- Pericardial effusion
- Empyema (pus in the pleural cavity)
- Pneumothorax
- Lung fibrosis
- Lung collapse (Atelectasis)
- Extra TB due to spread of the infection to other organs.
Nephrotic Syndrome
3. An adult male patient has been brought to medical ward with features of nephrotic syndrome
(a) List five cardinal signs and symptoms of nephrotic syndrome
(b) Describe his management from admission up to discharge.
(c) Mention five likely complications of this condition.
SOLUTIONS
(a) NEPHROTIC SYNDROME.
Is a syndrome caused by many diseases that affect the kidney characterized by severe and prolonged loss of protein in urine especially albumen, retention of excessive salts and water, increased levels of fats.
FIVE CARDINAL SIGNS AND SYMPTOMS.
- Massive protenuria.
- Generalized edema.
- Hyperlipidemia.
- Hypoalbuminemia.
- Hypertension.
(b) MANAGEMENT.
Aims of management
- To prevent protein loss in urine.
- To prevent and control edema.
- To prevent complications.
ACTUAL MANAGEMENT.
- Admit the patient in medical ward male side in a warm clean bed in a well ventilated room and take the patients particulars such as name, age, sex, religion, status.
- General physical examination is done to rule out the degree of oedema and other medical conditions that may need immediate attention.
- Vital observations are taken such as pulse, temperature, blood pressure recorded and any abnormality detected and reported for action to be taken.
- Inform the ward doctor about the patient’s conditions and mean while the following should be done.
- Position the patient in half sitting to ease and maintain breathing as the patient may present with dyspnoea due to presence of fluids in the pleural cavity.
- Weigh the patient to obtain the baseline weight and daily weighing of the patient should be done to ascertain whether edema is increasing or reducing which is evidenced by weight gain or loss.
- Monitor the fluid intake and output using a fluid balance chart to ascertain the state of the kidney.
- Encourage the patient to do deep breathing exercises to prevent lung complications such as atelectasis.
- Provide skin care particularly over edematous area to prevent skin breakdown.
- On doctor’s arrival, he may order for the following investigations.
- Urine for culture and sensitivity to identify the causative agent.
- Urine analysis for proteinuria and specific gravity.
- blood for;
- Renal function test, it will show us the state of the kidney function.
- Cholesterol levels; this will show us the level of cholesterol in blood.
- Serum albumen; this will show us the level of protein or albumen in blood.
- The doctor may prescribe the following drugs to be administered;
- Diuretics, such as spirinolactone 100-200mg o.d to reduce edema by increasing the fluid output by the kidney.
- Antihypertensives such as captoril to control the blood pressure.
- Infusion albumen 1g/kg in case of massive edema ascites and this will help to shift fluid from interstitial spaces back to the vascular system.
- Plasma blood transfusion to treat hypoalbuminemia.
- Cholesterol reducing medication to have the cholesterol levels in blood such as lovastatin.
- Anticoagulants to reduce the blood ability to clot and reduce the risk of blood clot formation e.g. Hepanine.
- Immune suppressing medications are given to control the immune system such as prednisolone if the cause is autoimmune.
- Antibiotics such as ceftriaxone to treat secondary bacterial infections.
- The doctor may order for renal transplant if the chemotherapy fails.
Routine nursing care.
- Continuous urine testing is done to see whether proteinuria is reducing or increasing.
- Encourage the patient to take a deity rich in carbohydrates and vitamins but low in protein and salts.
- Ensure enough rest for the patient as this will reduce on body demand for oxygen and hence prevent fatigue.
- Promote physical comfort by ensuring daily bed bath, change of position, oral care and change of bed linen.
- Re-assure the patient to alley anxiety and hence promote healing.
- Ensure bladder and bowel care for the patient.
ADVICE ON DISCHARGE
The patient is advised on the following:
- To take a deity low in salt and protein.
- Drug compliance.
- Personal hygiene.
- Stop using drugs like heroin, NSAID’s.
- Screening and treating of diseases predisposing or causing the disease.
- To come back for review on the appointment given.
COMPLICATIONS.
- Acute kidney failure.
- Kidney necrosis.
- Ascites.
- Pyelonephrosis.
- Cardiac failure
- Pulmonary embolism.
- Atherosclerosis.
- Deep venous thrombosis.
Surgical Nursing
Fractures
Josephine a thirty year old female patient has been involved in a road traffic accident and sustained a compound fracture.
(a) Outline ten signs and symptoms of fracture.
(b) Discuss the negative factors that can influence healing of a bone.
(c) Describe the healing of a bone.
(d) Mention ten complications of fractures.
SOLUTIONS
- a) History from the patient or the on lookers.
- Pain aggravated by movement
- Tenderness over the fractured limb
- Loss of function of the affected part or the whole limb
- Deformity
- Shortening of the limb
- Abnormal mobility at the affected area
- Creepers or grating of the bone ends as they move each other
- Swelling of the affected part
- Shock may occur
- The bone may be seen out if it’s a compound fracture
b)
- Tissue fragments between bone ends; Splinters of dead bone (sequestrate) and soft tissue fragments not removed by phagocytosis delay healing.
- Deficient blood supply; this delays growth of granulation tissue and new blood vessels. Hypoxia also reduces the number of osteoblasts and increases the number of chondrocytes that develop from there common parent cells. This may lead to cartilaginous union of fracture which results in a weaker repair.
- Poor alignment of bone ends: This may result in the formation of a callus that heals slowly and often results in permanent disability
- Continued mobility of bone ends; Continuous movement results in fibrosis of the granulation tissue followed fibrous union of the fracture.
- Miscellaneous; this include
- Infection; pathogens enter through broken skin, although they occasionally be blood borne, healing will not occur until infection resolves
- System illness
- Malnutrition
- Drugs e.g. Corticosteroids
- Aging
c)
- Following a fracture the broken ends of a bone a joined by the deposition of a new bone. This occurs in several stages
- Hematoma forms between the ends of the bone and in the surrounding soft tissues.
- There follows development of acute inflammation and accumulation of inflammatory exudates, continuing microphages that phagocytosis the hematoma and small fragments of a bone without blood supply(this takes place about five days). Fibroblasts migrate to the site, granulation tissue and the new capillaries develop.
- New bone forms as large numbers of osteoblasts secretes spongy bone, which unit the broken ends, and is protected by the outer layer of the bone and cartilage, this new deposits of bone and cartilage are called callus.
- Over the next few weeks, the callus matures and the cartilage is gradually replaced by new bone
- Reshaping of the bone continues and gradually the medullary canal is re –opened through the callus (in weeks or month). In time the bone heals completely with callus tissue replaced with mature compact bone. Often the bone is thicker and stronger at the repair site that originally, and the second is more likely to occur at a different site.
- d) Complications of fractures are divided in to two.
General complications.
- Local complications
- General complications are;
- Hemorrhage which may lead in to shock.
- Fat embolism
- Infections
- Hypostatic Pneumonia
- Damage to the nearby structures
Local complications
- Keloids
- Loss of function
- Damage to the nerves
- Necrosis
- Delayed union of bones; this may be as a result of incomplete reduction, inadequate immobilization, lack of blood supply to areas, infection which disrupt formation
- Malunion of the bones; this when there’s failure of bone fragments to unit. This as a result of a big gap between the fragment
Hyperthyroidism
1.Define:
(a) Hyperthyroidism:
(b)Hypothyroidism
(c) Thyrotoxicosis
2. Outline the differences between hyperthyroidism and hypothyroidism
3. Describe the management of a patient with hyperthyroidism.
4. Mention seven complications which are likely to occur following a thyroidectomy.
SOLUTIONS
The hub of excellence
a) Hyperthyroidism: this is a condition in which there is high circulating thyroid hormone in blood.
b) Hypothyroidism-this a condition in which there are low circulating thyroxin hormone in blood.
c) Thyrotoxicosis– it is a state of hyper secretion of thyroxin by the thyroid gland.
2. Differences between hyperthyroidism and hypothyroidism
Hyperthyroidism | Hypothyroidism |
It is characterized by excessive thyroxin production. | Characterized by insufficient thyroxin production. |
Characterized by weight loss with increased appetite and diarrhea | Characterized by weight gain |
More commonly caused by an auto immune response to specific anti bodies | Can be of congenital cause |
T4( thyronine ) levels are elevated | The serum Thyroid stimulating hormone is elevated in an attempt to produce more thyroxin |
Commonly occurs in women than men, usually at age of 20 to 40 years | Common in women of ages 30 to 60 years |
Surgery is always indicated incase medication and radio therapy has failed | Primarily managed by hormonal replacement therapy |
3. Management
- Patient is admitted on a medical ward for complete bed rest.
- Reassure patient and relatives.
- Vitals are taken and doctor informed
- Thorough physical assessment is done
Pre operative tests are ordered by the doctor and blood taken for the following tests;
- Serum thyroxin estimation- which levels are elevated in hyperthyroidism
- Serum tri-thyroxin(T3)
- TSH estimation –to rule out hypothyroidism
- Thyroid antibody measurement in cases of autoimmune thyroidism
- Radio active iodine uptake and scan for both diagnosis and treament.
- FNAC- for cytology to rule out any malignancy
- Fibre optic laryngoscopy-to view the vocal cords
Pre operative preparation(immediate)
- Patent’s HB is checked
- Cross match and book 2 units of blood
- x-ray chest thoracic inlet
- Shaving of the neck skin, upper part of the chest, the axilla and the upper arms
Pre operative drugs are also given as ordered by the doctor to bring patient to euthyroid state including;
- Carbimazole 10-20mg start 8hourly,several weeks then stopped 10days to surgery
- Propranolol 120-160 mg daily in divided doses. this is continued up to operation day
- Lugol’s iodine 0.3-0.9mls T.D.S. for 10 days-to reduce vascularity
- Diazepam 5mg 12 hourly to sedate the patient
- Digitalis incase of atrial fibrilation
Meanwhile, specific pre operative nursing care includes;
- Daily measuring of the neck circumference to monitor progression of thyroid enlargement
- Monitor serum electrolyte levels and check for hyperglycaemia
- Monitor for signs of heart failure e.g date dyspnoea
- Ensure nutritious diet with adequate calorie, proteins
- Minimize physical and emotional stress
- Re assure patient and family that mood swings will disappear with Rx.
- Monitor frequency and characteristic of stool and give anti diarrhaels as ordered
Post operative management
- Post operative bed is prepared and patient put in lateral position till recovery, then propped up supported by back rest.
- Monitor vitals including BP, Respirations. Give oxygen incase respirations are fast, shallow
- Report any respiratory difficulty for prompt management
- Ensure little fluid intake to clean the mouth.
Specific nursing care
- Ensure constant drainage in a drainage bottle or dressing
- Intubation if there is respiratory edema.
- Closely observe for hemorrhage.
- Ensure a calm environment, and possibly give drugs to encourage sleep.
- Care of drain and sutures; change drainage 24 hourly and sutures removed on third day or fourth day.
- Minimize patient’s neck movement to minimize neck pain.
- Give analgesics 1g start to reduce pain.
- 2 hourly vitals’ taking including temperature, respiration and blood pressure to monitor for any complications like thyroid storm or infections.
- Give antibiotics; ceftriaxone 2g 24 hourly
4. Complications of thyroidectomy
- Hemorrhage due to hyper ventilation of the thyroid gland
- Thyroid crisis (thyroid storm); characterized by rapid pulse, raised temperature, profuse, sweating, and confusion.
- Tetany; due to removal or trauma to parathyroid glands- it’s characterized by tingling and numbness of the face, lips and hands.
- Soreness of the throat.
- Hoarseness –due to damage to the recurrent laryngeal nerve
- Hypothyroidism due to thyroid removal
- Recurrent thyrotoxicosis
- Respiratory obstruction –due to laryngeal edema.
- Wound infection
Shock
1.An adult male patient has been brought to S.O.P.D with featured of shock.
(a)Define shock
(b) Explain seven types of shock that you know.
(c) Describe how you would manage a patient with hypovolemic shock.
SOLUTIONS
a). shock.
Is the failure of the circulatory system to maintain adequate tissue perfusion of the vital organs like the heart and kidney, brain?
PATHOPHYSIOLOGY
- Heart:-due to the reduced fluid volume in the body(blood) caused by vaso constriction leads to inadequate blood supply to the heart which decreases cardiac output hence less amount of blood reach the brain leading to hypoxia eventually shock occurs.
- B) . seven types of shock.
- Hemorrhagic shock.
It occurs due to severe blood loss causes are as follows:- Obstetric emergencies e.g. post partum heamorrhage, abortion etc, Trauma i.e. RTA, gun shot
- Septic shock
It occurs as result of bacteria multiplying in the blood and releasing toxins in the circulation leading to pooling of blood in the capillaries and blood vessels. It occurs in diabetic wounds, crutch wounds, burns.
- Carcinogenic shock ; this is when the heart fails to maintain tissue perfusion leading to shock. It results from the following; Heart attack, Myocardial infarction
- Neurogenic shock.
This is generalized vasodilatation due to stimulation of Vegas nerve e.g. due to strong pain.
- Anaphylactic shock.
This is due to hypersensitivity reaction which results from exposer to allergens leading to sudden cardiac arrest or respiratory distress. It can be due to reaction to drugs, foods.
- Hypovolemic shock.
This is due to loss of body fluids through diarrhea, vomiting, burns etc.
- Ologenic shock.
This is due to either receiving of good or bad news: – emotional upset
C). management
- It’s a surgical emergency that requires immediate intervention
Aims of management
- To maintain functions of the vital organs like the brain and heart
- To improve circulation
- To prevent complications
- To promote patients comfort
Admission
- The patient is received and quickly admitted in surgical ward in warm well ventilated room
- The relatives of the patient are reassured
- Patient is put in semi porn Position with the head turned to one side for easy drainage of secretions and to prevent the tongue from falling back
- The foot of the bed is elevated to aid return of blood to the circulatory center
- Quick assessment done
Assess the consciousness of the patient using Glasgow coma scale. This is performed as follows .
PARAMETERS | SCORE |
Eye opening
| 4 3 2 1 |
Best verbal response
| 5 4 3 2 1 |
Best motor response
| 6 5 4 3 2 1 |
Total response for 3 is 15 |
Observations i.e.
- Vital observations like temperature, pulse, respiration and BP (blood pressure).
- General observations such as level of dehydration, skin color for cyanosis.
- Doctor is informed
Specific management
Air way:-
- Artificial air way is put in position and sanction is done whenever necessary to avoid blockage of the air way with secretion and falling back tongue
- Air way piece is insitu to prevent back flow of the tongue.
Breathing:–
- Patient is administered oxygen 5-8 liters per minute in order to ventilate the lungs and increase tissue perfusion.
Circulation:-
- Plan c of management of dehydration applies
- An intravenous line is established to re hydrate patient with intravenous fluids like normal saline 0.9% and ringers lactate(se) allows it to run faster at a drop /rate of 40drops per minute
- Continue monitoring the patient’s condition for over flow
Investigations
Doctor orders for the following investigations below.
Blood
- Hb, grouping and cross matching
- CBC (complete blood count, Ph of the blood showing decreased Ph (acidic Ph)
ECG (Electrocardiogram)
- To check for the activities of the heart.
EEG (.electro encephalogram):-
- To check for the activities of the brain.
Urinalysis: –
- To determine kidney function
Specific nursing care
- Patient is provided with warmth by adding additional blanket but not to overheated transfuse the patient incase patient is anemic with whole blood and to improve blood volume in the circulation
- Foot of the bed is elevated to aid return of blood into the circulatory center.
- Continue monitoring vitals that is TPR/BP, to detect deviation from the normal.
General nursing care
Hygiene:-
- Ensure patient s hygiene by daily oral care, care of the skin , finger nails, patients hair, daily bathing of patient if able and if patient unable to bath by self carry out bed bath for patient as well much attention is on the pressure areas.
Diet:-
- The patient is feed on well balanced diet and light diet which can digest easily. Feeding is done using naso gastric tube, when patients condition improves give patient food orally.
Rest and sleep:-
- Adequate rest is ensured by limiting visitors; minimize noise in the room or ward etc.
Psychotherapy:-
- This includes care of mind by counseling, give adequate information about the illness to the patient and the relatives or family members
Physiotherapy: –
- This is done by helping and encouraging the patient to carry out some light exercise that is passive and active exercise such as deep breathing exercise.
Elimination
- Care of the bladder and bowel check if patient is passing urine out normally and avoid constipation by encouraging plenty of fluids and light diet is suitable
- Pass catheter incase of incontinence to prevent wetting of the bed or soiling of the bed linen
- Give bed pan to the patient if passing out stool normally.
- Establish fluid balance chart in order to monitor fluid input and output.
Tracheostomy
A male patient aged 40 yrs has been brought to S.O.P.D with features of an airway obstruction, upon assessment the surgeon recommended for a tracheotomy.
- Define tracheotomy.
- Mention 10 indications of a tracheotomy.
- Describe the pre and post operative management of the patient up to discharge.
- Mention 5 likely complications which may occur following a tracheotomy.
SOLUTIONS
Tracheotomy is the artificial opening through the neck into the trachea to relieve sudden airway obstruction
Indications of a tracheotomy
These are divided into two i.e. obstructive conditions of the larynx and paralysis or spasm of the respiratory muscles or respiratory failure.
- Obstructive conditions of the larynx
- Acute laryngitis e.g. in diphtheria
- Carcinoma of the larynx
- A cute oedema of the glottis
- Foreign body in the airway
- Trauma to the trachea
- Severe burns of the mouth or involving the larynx
- Severe neck or mouth injuries
- Paralysis or spasms of the respiratory muscles failure
- Paralysis of the respiratory muscles
- Respiratory failure
- Tetanus
- Following thyroidectomy
- Surgery around the box (larynx) that prevents normal breathing and swallowing
Pre-operative management of the patient for tracheostomy
Aims
- To relieve sudden airway obstruction
- To alley patient’s anxiety
- To prevent likely complications to occur .
Admission: The patient is admitted to the surgical ward in a well ventilated room and all procedures are done within this time.
Nurse patient relationship / rapport: A positive nurse patient relationship is created to alley patients, anxiety; explain the nature of condition is having to the patient and what is going to be done.
Observation: Both general and vital observations are done to know the state of condition in which the patient is in starting with general observations then vital observations that is temperature, tube, respiration and pressure monitor patients conditions
Investigation: The doctor will order for investigation i.e. Hb, biopsy
Consent form: It’s obtained from the patient after through explanation towards what is going to be done in theatre to relieve airway obstruction
Shaving: This is done immediately before the patient being taken to theatre for operation
Theatre gown: The patient is offered with a theatre gown before going in for operation, all other items like bangle and dentures are removed there and then
Premedication: Will be administered to the patient if any was prescribed by the doctor
Informing of theatre staffs: They are informed before the patient is taken for theater for the operation
Patient taken of theatre: The patient will then be taken to theatre for operation by two nurses who will handle the patient to theatre staff
Post – operative bed: After the nurses have handled over the patient in theatre they will come and make a postoperative bed and all its accompaniments
In theatre : A patient well be positioned in a supine position with the neck hyper extended over the shoulder which brings the tracheal orifice closer to the surface. An incision is made on the trachea and the tracheal tube inserted into the opening and secured in position with tapes tied around the neck
Post operative management
Prepare an emergency tray at the bed side with tapes tied around the neck
- Sterile tracheal dilators,
- Sterile suction catheters
- Sterile gloves
- Suction machine with half an inch of savlon in the suction bottle
- Bowl of savlon
- Gallipot with saline to act as a lubricant
After completion of the operation, the theatre team will inform ward nurse s to come all collect the [patent taken to the ward
On the ward
Position: The patient should lie flat in bed had turned on one side hourly for easy drainage, when patient a wakens he should be probed up and kept in this position for 48 hours
Observations: Vital observations are done ½ hourly for ½ hourly for 2 hours , 1 hourly , 2 hourly for 6b hours then when the patient stabilizers they are done twice a day , much emphasis is put on the respiration rates , observe the tube to see if its not blocked.
Medication: Drugs like antibiotics to treat or prevent any infections like – IV ceftriaxone1-2 gms o.d for 5-7 days
Analgesics e.g. in diclofenac 75 mg IM 8hry for 24 hours then paracetamol tablets 1gm tds for 3 days
Oxygen may be administered via the tracheotomy mask or tube
Care of the tubes: Frequent suction is very important at least 2 hourly then later PRN , it’s done by anesthetist and a nurse , the inner tube is washed with sodium bicarbonate , sterilized and replaced as required a supply of sterile tubes be readily available
Keep the tube covered loosely with gauze to prevent entry of cockroaches and other insects especially at night
Care of the incision wound: It should be cleaned daily using a suitable antiseptic and new dressings replaced, key hole dressing is used
Exercises: Deep breathing exercises are carried out under the direction by a physiotherapist, suction must be readily available for the nurse to suck the secretions
Provide a bell, book and pen for easy communication in acute phase
Diet: Swallowing may be very difficult especially in the acute phase but small amounts of fluids can usually be taken and if the patient fails to tolerate intravenous fluids are given , when the condition improves they are stopped
Hygiene : Is should be observed throughout to prevent respiratory infections, hands scrubbed and worn to prevent cross infection. Tubes must be stylized before re use
Psychological care: This is maintained throughout the patient’s stays on the ward to alley anxiety
Bowel and bladder care: By taking of plenty of oral sips and roughages to prevent constipation
Rest and sleep: Ensure that the patient facts enough reset a sleep by minimizing noise, dimming lights during the night and covering the tube to prevent entry of insects into the tube
Discharge : When the patient’s condition is satisfaction will be discharged home and follow up date given
N.B
In case the tracheostomy is permanent like in cases of career , the patient will be returning for reviews and increase where its temporarily when the obstruction has resolved the tube is removed and the wound left to close
Advice on discharge
- Take drugs as prescribed
- Maintain proper hygiene
- Maintain / keep follow up dates
Complications
- Haemorrhage
- Shock
- Infections
- Respiratory failure
- Emphysema
- Nerve injury including paralysis
- Scarring
- Damage to the thyroid gland
Pharmacology
Malaria
Opio aged 10 years with a body weight of 18 kg was diagnosed with severe malaria. The doctor prescribed IV artesunate and requested the nurse to calculate the right dose.
- State any four cardinal symptoms of severe malaria.
- Calculate the dose of IV artesunate you would give to Opio.
- Outline the steps you would take as you administer IV artesunate.
- Mention any 3 drugs used in the prevention of malaria.
SOLUTIONS
Malaria: Is an acute illness characterized by fever and other clinical features which is caused by infection with the malaria parasites of the genus anopheles mosquito.
TRANSMISSION: Malaria is transmitted from one person to another through the bite of an infected anopheles mosquito.
Plasmodium species
- P. Falciparum
- P. Malarie
- P. Vivax
- P. Ovale
No.1
- Altered mental state / confusion.
- Convulsions.
- Severe anemia.
- Prostration.
- Difficulty in breathing.
No.2
Artesunate dosage =3.0mg × body weight
=3mg ×18
= 54mg
Therefore: The dosage of Artesunate to be given to Opio is 54mg.
No. 3
- Identify the patient.
- Create a rapport and weigh the patient.
- Identify the drug and check for the expiry date.
- Reconstitute the drug by mixing Sodium bicarbonate with Artesunate powder.
- Shake approximately for 2 minutes until the dissolved solution will be cloudy.
- The reconstituted solution will be clear in about 1 minute. Discard if not clear.
- Insert the needle to remove air.
- Inject the required volume of saline in to the reconstituted solution.
- Artesunate solution is now ready for use.
- With draw the required dose in m/s according to the route of administration.
- Give slow IV injection 3-4 minutes per minute or injection in the appropriate site by deep IM.
No.4
- Chloroquine
- Sulphurdoxine.
- Doxycycline.
- Mefloquine.
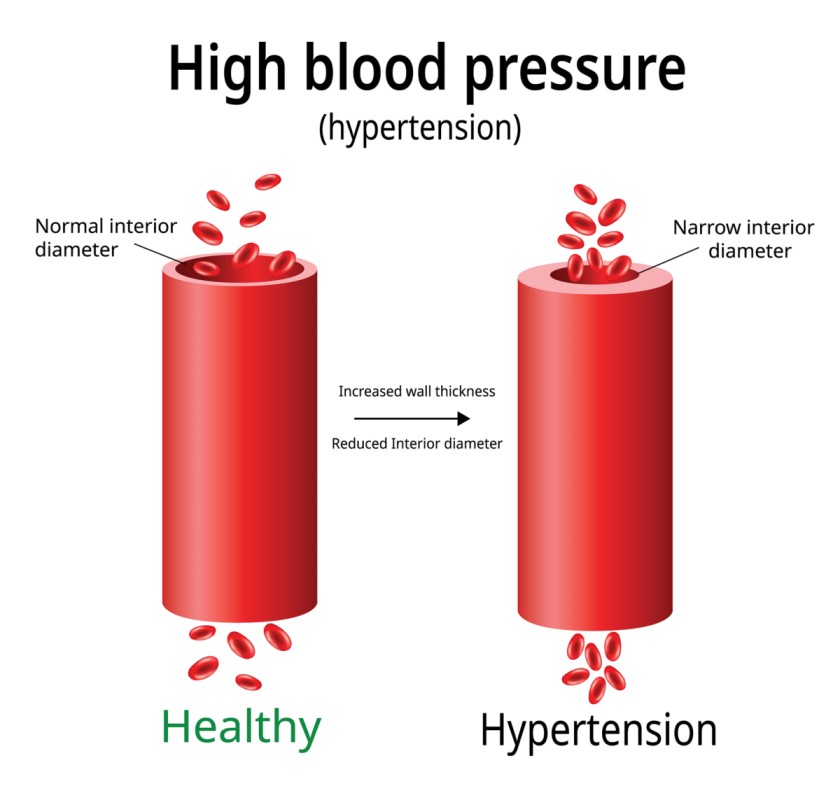
Hypertension
MN, a 44 year old truck driver was diagnosed with hypertension by his doctor after registering a BP of 160/ 95 mmhg on 3 separate clinic visits. MN weighs 107 kgs and his height is 1.7 M tall. He smokes an average of 16 cigarettes per day and drinks 4 bottles of beer every evening. The doctor prescribed Nifedipine 20mg 12 hourly for 30 days.
- To which class of anti hypertensive does Nifedipine belong?
- Name any other 3 drugs that belong to the same class as Nifedipine.
- Give 4 common side effects associated with the use of Nifedipine.
- Besides drug treatment, give any 5 advices you would give to Opio in order to effectively control his blood pressure.
- Mention any 4 complications associated with poorly managed hypertension.
SOLUTIONS
- Nifedipine belongs to a group of antihypertensive called calcium channel blockers
Calcium channel blockers act by decreasing calcium uptake into cardiac and smooth muscles by blocking slow calcium channels which reduces on the vascular tone that results into reduction in peripheral resistance thus controlling blood pressure
2. Examples of other calcium channel blockers
- Amlodipine Tablets 10mg, 5mg
- Nicardipine Capsules 20mg, 30mg
- Felodipine Tablets 2.5mg, 5mg, 10mg
- Nimodipine Tablets 30mg
3. Side effects associated with the use of Nifedipine
- Peripheral edema
- Flushing
- Hypotension
- Visual disturbances
- Headache
- Dizziness
- Fatigue
- Fast heart rate
4. Advises which can be given to Mr. Opio to effectively control his blood pressure
- Health educating Opio about dangers of smoking
- Health educating him about the dangers of excessive alcohol consumption
- Eating much less than usual to reduce the weight
- Eating fat free foods
- Doing enough exercises
- Visiting the clinic regularly for blood pressure checking
- Teaching him about the warning signs of elevated blood pressure
5. Complications of poorly managed hypertension
- Renal failure
- Glomeronephritis
- Heart failure
- Retinopathy
- Un explained abortions
- Intra uterine growth retardation i.e. in pregnant mothers
- Cerebral vascular accident
- Hypertensive encephalopathy
- Impotence
- Brain damage
Mental Health
Causes of Mental Illnesses
- Mental illness is very common in Uganda, Write down the general causes of mental illness.
SOLUTIONS
CAUSES OF MENTAL ILLNESS.
The chief cause of mental illness is unknown i.e. it is idiopathic.
However research states a number of factors responsible for causing mental illness.
These factors are either;
- Predisposing factors
- Precipitating factors
- Perpetuating factors.
PREDISPOSING FACTORS
- These factors determine an individual’s susceptibility to mental illness. They interact with triggering factors resulting into mental illness. Examples include; Genetic risk factor, physical damage to the central nervous system (the brain and spinal cord).
PRECIPITATING FACTORS.
- These are events that occur shortly before the onset of the disorder. I.e. they trigger the onset of the disease. Examples include; physical stress and psychosocial stress.
PERPETUATING FACTORS.
- These factors are responsible for aggravating or prolonging the disease already existing in an individual. Examples include; psychosocial stress.
Thus, etiological factors of mental illness can be;
- Biological factors
- Physiological factors
- Psychological factors
- Social factors
BIOLOGICAL FACTORS
- Genetic risk factor; According to research individuals born in families with parents and relatives who have suffered from mental illness, are susceptible to developing mental illness once exposed stressful conditions. This is because the predisposition gene is passed on from the parents to the offspring.
- Biochemical; This regards the neurotransmitters (provide medium for transmission of impulses). Any imbalances in the levels of the neurotransmitters in the brain may result into mental illness as shown below.
Neurotransmitter related state | Mental disorder |
Increased in dopamine level | Schizophrenia |
Decrease in nor epinephrine level | Depression |
Decrease in serotonin level | Alzheimer’s disease |
Decrease in gamma amino butyric acid | Anxiety |
Decrease in glutamate level | Psychotic thinking |
Brain damage; This may be as a result of;
- Infections e.g. HIV infection, neurosphilis, encephalitis etc.
- Injury that involves loss of the brain tissue.
- Intoxication; toxins that can damage the brain tissue e.g. alcohol.
- Vascular damage; damage to blood vessels leading to poor blood supply to the brain, subdural hemorrhage, intracranial hemorrhage, etc.
- Tumors; brain tumors
- Degenerative diseases; dementia.
Physiological factors; The functioning of the body changes at certain critical periods in life i.e., puberty, pregnancy, menstruation, peurperium and delivery. Coupling these physiological changes with maladaptive psychological capacity makes an individual susceptible to mental ill health.
Psychological factors;
- Personality; It has been observed that specific personality types are more prone to certain psychological disorders, e.g. Schizoid personality (unsocial and reserved) are vulnerable to schizophrenia under stressful situations.
- Strained interpersonal relationships at home, school and work.
- Childhood insecurity due to parent’s over strictness, rejection and unhealthy comparisons.
- Social and recreational deprivation; which may result into boredom, isolation and alienation.
- Marriage problems e.g. forced bachelorhood, childlessness and many children.
- Sexual difficulties.
- Stress and frustrations.
Social factors;
- Poverty.
- Unemployment.
- Injustice.
- Insecurity.
- Migration.
- Urbanization.
- Gambling.
- Alcoholism.
- Prostitution.
- Divorce.
- Religions.
- Traditions.
Psychiatric Emergencies
Psychiatric emergencies are very common in the community.
- Mention all the psychiatric emergencies.
- How can we prevent psychiatric emergencies?
- Nakimbugwe, a psychiatric patient has completely refused to eat food and she wants to starve herself to death, How can you manage such a patient?
SOLUTIONS
- The psychiatric emergencies.
- Aggression and violence; Aggression is an intended behavior that can cause pain, harm directly to one self or others either physically or verbally whereas violence is an intention to use physical force/power to threatened action against one’s self, other person or group resulting into injury.
- Suicidal attempts; This is a type of deliberate self-harm and is defined as an intentional human act of killing oneself.
- Delirium tremens; A type of delirium caused by abrupt withdraw from excessive taking of alcohol or substance of abuse
- Status Epilepticus; This is said to occur when a seizure lasts too long or when seizures occur close together and the person doesn’t recover between seizures.
- Catatonic stupor; This refers to decreased motor activity or being emotionless or being unresponsive to the environment stimuli although he or she is conscious
- Hysterical attacks; This personality disorder due to the upbringing. Individual of this category present with exaggeration, attention seeking, want over protection, very sensitive to pain and also want to be cared about
- Furor Epilepticus; The sudden unprovoked attacks of intense anger and violence to which individuals with psychomotor epilepsy are occasionally subject.
- Panic attacks; This is a psychiatric emergency characterized by periods of intensive fear, which occurs suddenly without accompanying danger but person thinks or perceives that there is danger
- Total insomnia; Sleeping disorder characterized by loss of sleep of an individual
- Food refusal; Psychiatric eating disorder characterized by abandoning of oneself to eat food
- Severe depression; Excessive type of depression characterized by persisted low mood or sadness
2. How we can prevent psychiatric emergencies.
Psychiatric emergencies are life threatening and therefore they should be attended to urgently to prevent complications and save life. I.e. the ways include;
- Proper counseling and guidance of patients with stress disorders
- Proper management of psychiatric conditions
- Early diagnosis and treatment of psychiatric conditions
- Health education of the people about the predisposing factors to severe mental illness
- Equipping heath skilled workers on how to manage the psychiatric conditions by regular CME’s.
- Ensuring drug compliance to prevent relapses and progression to severity
3. Management of food refusal
On admission
Patient is hospitalized in a psychiatric unit and a rapport is created in order to gain confidence of the patient in the health unit and the healthy worker
Assessment
- Subjective data; Here history is obtained of any chronic illness, and any history about mental illness in the family
- Objective data; physical examination from head to toe and general appearance of the patient to rule out any underlining conditions
- Mental data; This involves the emotional response, concentration, orientation , memory and perception.
Investigation
- Do an FBC to rule out any infection
- VDL test to rule out syphilis
- Do an RBS to check the amount of sugar levels of the patient
- Do a urinalysis for ketones
Nursing care
- Daily weighing of the patient is paramount
- Monitor status of skin and mucous membranes
- Encourage the patient to verbalize feelings of not wanting food.
- Maintenance of a strict output and input chart
- Avoid discussions that focus on food and weight gain
- Allow patient to take packed foods and fluids
- Encourage family to participate in education regarding connection between family process and the patient’s disorders
- Control vomiting by making the bathroom inaccessible for at least 2hours
- Eating must be supervised by the nurse and a balanced diet of atleast 3000 calories should be provided in 24hours
Drugs
- Give appetite stimulants like multivitamins
- Give antidepressants like Amitriptyline 25mg-75mgs
Family therapy; Educate and counsel the family to accept the patient
Psychotherapy; If the patient’s condition improves, assist the patient to sit and move around and encourage her by respecting her suggestions
Individual therapy; Talk politely to the patient and make him aware that she is important by respecting her decisions
Bi-Polar
Bipolar Affective Disorder is one of the common conditions patients present with.
- What is bipolar affective disorder?
- Mention the signs and symptoms of Bipolar Affective Disorder?
- How would you manage a patient with bipolar affective disorder?
SOLUTIONS
- Bipolar affective disorder– is an affective/ mood disorder characterized by alternating attacks of Mania and Depression separated by episodes of normal mood
- Signs and symptoms of Bipolar affective disorder
Manic episode
- Persistently elevated mood
- Increased psychomotor activity
- Flight of ideas
- Poor judgement
- Pressure of speech
- Lack of insight
- Delusions of grandeur and persecution
- Decreased food intake due to over activity
- Dressed in flamboyant clothes. In severe cases, there is poor self care
- Decreased need for sleep (less than 3hrs)
- Increased libido
- Decreased attention and concentration
- High risk activity
- Irritability
- Increased sociabilities
- Impulsive behavior
- High risk activities e.g. reckless driving, foolish business investment, distributing money or articles to unknown people
Depressive episode
- Decreased psychomotor activity
- Persistent low mood/ sadness
- Social withdrawal
- Loss of energy
- Hopelessness, unworthlessness and powerlessness
- Fatigue
- Delusion of persecution, sin, control, unworthiness, hypochondriasis
- Decreased food intake due to lack of appetite
- Auditory hallucinations
- Avolition i.e. lack of will to act
- Ambivalence i.e. two opposing ideas
- Anhedonia i.e. inability to experience pleasure
- Insomnia
- Physiological symptoms e.g. headache, backache, chest pain, amenorrhea, decreased libido, abdominal pain
- Tearfulness
- Pessimistic
- Recurrent thoughts of death
- Slow speech/ poverty of ideas
- Negativism
3. Management of Bipolar affective disorder
Manic phase
Aims of management
- To alleviate delusions and hallucination
- To alleviate hyperactivity
- To prevent possible injury and aggression
- To calm down the patient
- To restore normal food intake
- To restore normal sleep pattern
Management
- Assessment to obtain baseline data and the basis for evaluation. It focuses on the severity of the disorder, causes, patients’ resources, mood and affect, thinking, perceptual ability, sleep disturbance, changes in energy level.
Obtain both objective and subjective data from the patient
Objective data
- Disturbed speech
- Rapid speech
- Loud pressured speech
- Over activity
- Mood lability
- Weight changes
Subjective data
- Feelings of joy
- Rapid mood swing
- Sleep disturbance
- Delusions and hallucinations
- Admit the patient on an acute non-storeyed psychiatric ward with minimum furniture, free from harmful objects with reduced environmental stimuli to prevent possible harm to self or others.
- Form a positive nurse-patient relationship to win the patients’ trust and confidence
- Encourage patient to verbally express his feelings to relieve tension and hostility
- Have sufficient staff to show strength to the patient and convey contrl over the situation
- Reassure patients and relatives to allay anxiety
- Encourage performance of planned activities to channel excess energy into socially acceptable behaviours
- Formulate a contract and set limits on manipulative behavior, explain the consequences if limits are violated
- Stay with the patient as hyperactivity increases to offer support and provide a feeling of security
- Keep the patient occupied most of the time during day, discourage day sleep eliminate uncomfortable stimuli at bed time, avoid caffeine containing drinks at bed time, administer prescribed hypnotics to promote sleep and rest of the patient
- Teach the patient relaxation techniques e.g. deep breathing exercise, diversion techniques e.g. listening to music to cope with anxiety
- To restore normal food intake:
- Serve the patient meals on time
- Involve patient in food preparation
- Serve meals in clean and attractive dishes
- Fruits should be provided unpeeled
- Provide patients with foods that the patient can eat while moving
- Encourage patient to sit down and eat
- Provide a balanced diet
- Ensure adequate fluid intake
- Monitor fluid intake and output
- Weigh the patient regularly
12. Encourage the patient to interact with others to promote communication
13. Positive reinforcement for desired behaviours
14. Involve family members in the management of this patient
15. Administer prescribed drugs i.e.
- Major tranquilizers such as Chlorpromazine 100-600mg daily in divided doses, Haloperidol 5-60mg daily
- Mood stabilizers such as carbomazepine200-1000mg daily, Lithium carbonate300-1500mg daily in divided doses, Sodium valporate600-2600mg daily
- Anxiolytics and sedatives such as Diazepam 5-20mg daily in divided doses
16. Monitor side effects of drugs
17. ECT
18. Health educate patient and family members about side effects and how to manage them, increased fluid intake, drug compliance
19. Advice on discharge
Depressive episode
Aims of management
- To promote possible harm self and others
- To restore normal nutritional status
- To restore normal sleep pattern
- To restore normal communication
Interventions
- Assessment to obtain baseline information and determine the basis for evaluation. It focuses on severity, risk for suicide, causes, resources available, Mood, affect, thinking, somatic complaints. Obtain both objective and subjective data
Objective data
- Alteration of activity
- Poor personal hygiene
- Apathy
- Altered social interaction
- Impaired cognition
- Delusions
Subjective data
- Anhedonia
- Worthlessness, hopelessness, helplessness
- Suicidal idea
- Admit the patient on a non-stored open psychiatric ward with limited furniture, free from dangerous objects to prevent possible harm to self
- Form a therapeutic nurse- patient relationship to win patients’ trust and confidence
- Closely supervise the patient during meals and medication time
- Form a contract with the patient not to harm self. This gives a degree of responsibility of his safety
- Explore feelings of anger and help the client direct them towards intended object
- Accept the clients’ feelings, spend time with the patient, focus on the strengths and accomplishments and minimize failures to build patients’ self esteem
- Teach patient assertive and communication skills to promote self esteem
- Allow the patient to participate in goal setting and decision making regarding own core to increase his or her feelings of control
- Positive reinforcement for desired behavior
- Close supervision is always required when recovering from the disease
- Involve patient in groups as he improves to promote communication
- Ensure quiet and peaceful environment, give warm bath to the patient, do not allow patient to sleep during day, sedatives, plan day activities basing on patients’ interest to improve night sleep
- Closely monitor food and fluid intake, maintain input and output chart, record patients’ weight regularly, serve patient with the food he likes, feed the patient on small but frequent meals, encourage more fluid intake to restore normal nutrition. Feed patient on roughage diet and green vegetables to prevent constipation
- Administer prescribed drugs i.e.
- Antidepressants such as
- SSRI’s e.g. Fluoxetine 20-60mg daily, Paroxetine, Sertraline, Citalopram
- Tricyclic antidepressants e.g. Amitriptyline 25-75mg Nocte, Imipramine 25-150mg
- MAOIs’ e.g. Phenelzine
- Others e.g. Maprotiline
Mania
Nakibirye, a mentally ill is presenting with a provisional diagnosis of mania.
- Define the term mania.
- What are the causes of mania?
- Mention the signs and symptoms of mania.
- What medical treatment will be given to this patient with mania?
SOLUTIONS
- Mania is a mood disorder characterized by self important ideas, mood changes consisting of elation, irritability and over activity sustained over a long period of time
2. Causes of mania
The actual cause is idiopathic but however there are factors that are believed to contribute to its occurrence.
They include:
- Predisposing factors
- Precipitating factors
- Perpetuating factors/ maintaining factors
(I) PREDISPORSING FACTORS
These are factors that may operate from early life or people are born with them.
- Hereditary: Mania is believed to have been passed on from the parents/ relatives who suffered from it to children
- Uterine environment: This includes factors like maternal drug abuse while pregnant which can be transplacental and causes effect to the fetus
- Personality: People with difficult personalities like the paranoid are predisposed to mania due to their irritative mood
- Biochemical factor: This includes the abnormal secretion of neuro transmitters and hormones like over secretion of serotonin, dopamine, acetylcholine, adrenaline hormone stimulates the hyperactivity of the body.
(II) PRECIPITATING FACTOR
These are factors which occur shortly before the onset of the illness and appear to have induced the disorder for example:
- Physical and social factors like upbringing of children: Which can be due to too much freedom/ permissiveness given to children by parents when growing up?
- Maternal deprivation: This creates a depressive mood at early childhood due to inadequate maternal love provided to the child but later mania may be developed as denial to the depression.
- Anxious parents: For example parents who expect much from the child and hence drive child’s mind to go for bigger positions (like in leadership if at school) in order to sustain the parents.
- Physical stressors: These include changes that which occur for example during adolescents
- Psychological situations: Financial achievements like acquiring a job, winning money/prizes. Fulfilled goals in life like education at higher levels like masters degree, PHD.
- Marriage and partnership: Being wedded/ introduced especially among women by their husbands. Becoming pregnant for example among women once pronounced infertile by community.
- Drug abuse like alcohol abuse marijuana, khaki etc: Trauma to the brain for example through accidents involving the head. Brain tumor like brain cancer can precipitate mania. Infections like syphilis, meningitis that affect the brain tissues may precipitate mania .
(iii) PERPECUATING FACTOR
- Continuous drug abuse during the illness.
- Poor drug compliance during the illness.
- Loss of a job due to the disorder.
- Difficulty personality maintaince for example psyclothemic who have mood swing
4. What medical treatment will be given to this patient with mania?
- Mania can be managed with/ without treatment depending on the cause.
- The patient is admitted on psychiatric ward in a side room with no furniture’s, open sealing or an y other metals to avoid injuries to the patient.
- She is given the following medical treatment as prescribed by the psychiatric doctor.
- Anti-psychotic drugs- to control psychotic features like hallucination for example chlorpromazine initially 100-200mg 8hourly,then daily doses of up to 300mg are given as a single dose at night.
OR.
- Iv sterazine 5-10mg every 12hours;then adjust according to the response up to 40mg or more daily may be required in severe or persistent cases..
OR.
- IV haloperidol 5-10mg for every 12 hours; then assessment is made according to response.
- An additional dose of diazepam 5-20mg 12hourly for 3/7 its given with chlorpromazine (above)
- If patients condition improves is given tablets diazepam 10mg once at night to allow patient rest.
- She can also be given a mood stabilizer for example.
- Carbamezapine 200mg once a day until a condition stabilizers
OR
- Tabs: sodium valporate 200-500mg 12 hourly
OR
- Tabs: lithium carbonate 300mg once a day till condition stabilizers.
- In case of extra pyramidal side effects, tablets artane is given 2mg-5mg once daily.
Supportive treatment
- Family planning is initiated for example IM depoprouera 150mg for every 3 months since she has a high libido.
- I.V fluids like normal saline/ dextrose 10% for rehydrating the patient.
- A nutritious diet is provided to the patient to boast the immunity.
- Psychotherapy like counseling incase patient gains insight.
- And investigations are carried out to find out the underlying cause for example rapid plasma reagent (RPR) to R/O for syphilis , serology to R/O HIV/AIDS , and a CT-scan to R/O brain tumors.
Pediatrics
Immunisation, Cold chain
- Define the term immunization.
- Outline the current immunization schedule.
- Describe the cold chain system.
SOLUTIONS
Definition.
Immunization is the process of introducing a weakened or killed vaccine into the body in an attempt to increase the body’s ability to fight against immunizable diseases.
UGANDA NATIONAL EXPANDED PROGRAMME ON IMMUNIZATION (UNEPI)
Vaccine | Doses | No of dosage | Interval between dosage | Minimum age to start. | Route of administration. | Site of administration. | Storage temperature. | Remark | ||||||||||
BCG | -0.05mls up to 11months -0.1mls after 11months. | 1 | None | -At birth -At 1st contact. | I M | -Right upper arm. | +2-+8 | -Use diluents provided for BCG ONLY. Not to be given to children with symptomatic HIV/AIDS. -Discard reconstituted vaccine after 6 hrs. Use sponge method. | ||||||||||
DPT+ Hep B – Hip | 0.5mls | 3 | 1 month | At 6 weeks. | I M | -Outer aspect of the left thigh. | +2-+8 | -Don’t freeze -Don’t place directly on ice. Use sponge method. | ||||||||||
PCV | 0.5mls | 3 | 1 month | At 6 weeks. | I M | -Outer aspect of the thigh. | +2-+8 | -Don’t freeze Use sponge method. | ||||||||||
Polio O.P.V | 3 drops | 0+3 | 1 month | -At birth OPV -First contact. | Orally | Mouth | +2-+8 | -Use diluents provided. -Discard used vial. Use sponge method. | ||||||||||
Measles | 0.5mls | 1 | None | At 9 months 1st contact. | S/C | -Left upper aspect of the arm. -Outer aspect of the thigh. | +2-+8 | -Use diluents provided. Use sponge method. | ||||||||||
Tetanus toxoid | 0.5mls | 5 | TT1-TT2=1mnth TT2-TT3=6mnth TT3-TT4=1yr TT4-TT5=1yr. | -At child bearing age 1st contact Pregnant mother | I M | -Upper arm or -Outer aspect of the thigh. | +2-+8 | -Don’t freeze -Don’t place vial directly on the ice pack. Use sponge method. | ||||||||||
HPV | 0.5mls | 2 | HPV 1:At first contact with a girl in primary 4 or aged 10 years for those in the community HPV2; 6 months after HPV1. | Girls in primary 4 or 10 years old girls who are out of school. | IM | Left upper arm. | +2 to 8 | Don’t freeze Use conditioned ice packs Use sponge method | ||||||||||
| ||||||||||||||||||
b). Cold chain – Refers to the set of equipments or containers in which vaccines are stored at specified temperatures and transported from the moment of manufacture to the time of administration. It is essential to ensure an unbroken cold chain for vaccines right from the manufacturer (producer) to the person being vaccinated. The specified temperature range is 35° F (2°C) to 45°F (8°C),the system involves personnels, equipments, vaccines, supplies and procedures.
If the vaccines get warm, their potency (effectiveness) is lost, especially those containing live organisms such as polio and measles. On the other hand, vaccines made from toxoids such as Tetanus and diphtheria, and suspended dead organisms such as whooping cough (pertussis) must not be frozen as this will make them loose potency. Vaccines must be stored at their own correct temperatures all the time. The cold chain must not be broken. If the cold chain is broken, Vaccines may loose potency and become useless.
DIAGRAMATIC REPRESENTATION OF THE COLD CHAIN.
|
Airport |
Central vaccine store |
Regional or District store | ||
Mobile or Outreach post | ||
Health centre |
Immunization post |
Recipient (Mothers, children) |
The chain travels in this way;
- From the manufacturer to the airport, vaccines are carried in deep freezers in the aeroplane.
- From the airport, to the general medical vaccines stores and they are carried in freezers or cold boxes.
- From the general medical vaccines stores to the regional (Districts). They are carried in a refrigerated van, in a refrigerator, cold boxes or vaccine carriers.
- From the district to the health units, they are carried in the vaccine carriers or cold boxes.
- From the health unit to the outreach site, the vaccine should be wrapped in black polythene bags and carried in a well packed vaccine carrier with ice packs.
In the chain vaccines should be separated into those that can be frozen and those that must not be frozen.
The temperature monitoring devices used in the cold chain are; Thermometers and vaccine vial monitors (VVMS).
The equipments used in the cold chain are;
- Cold rooms
- Freezers and Refrigerators
- Vaccine carriers
- Ice packs.
- Thermometers.
COLD ROOMS
Cold rooms are large, specially constructed rooms or self- contained buildings located at national and in some cases regional levels for storage of large quantities of vaccines that last for 12 months or more.
They have a 24-hour temperature monitoring system with an alarm, a recorder, and a back up generation that will turn on automatically when the regular power is interrupted.
FREEZERS AND REFRIGERATORS
Freezers and refrigerators are used at the district, regional and central stores.
Freezers are used for freezing icepacks and storing some vaccines, particularly OPV that need to be kept at temperatures below 0°c. Other vaccines are stored in refrigerators, which are also used for chilling diluents before mixing with freeze- drained Ice lined refrigerations, which are used at the central and regional levels, are capable of maintaining temperatures below =8°c even when electricity fails as many as 16 of every 24 hours, day after day.
HOW TO CARE FOR REFRIGERATORS.
COLD BOXES
Cold boxes are insulated containers that are lined with icepacks to keep vaccines and diluents cold. They are normally used to transport vaccines from the central level to the regions, regions to districts, and sometimes from districts to the service delivery levels (immunization posts). In some developing countries, Refrigerated vehicles are used instead of cold boxes.
However, these vehicles are expensive to buy, and are subject to frequent mechanical breakdowns, a good cold box works as well, or even better.
Cold boxes are used for temporary storage of vaccines when a refrigerator is out of order, or being defrosted.
VACCINE CARRIERS
These are insulated containers that are lined with icepacks to keep vaccines and diluents cold. They are more portable, are commonly used to transport vaccines from distinct stores to smaller health facilities and to outreach sessions (immunization posts).
ICE PACKS
An icepack is a flat rectangular plastic container designed to be filled with clean water, frozen and then used to keep vaccine. Icepacks must be placed in a cold box or vaccine carrier in a precise way, So their size is important. One extra set of ice packs should be available so that while one set is being frozen at a temperature of (-) 25°C, the other is being used. Freezing icepacks is a process that usually takes at least 24 hours. The icepacks are different from vaccine carriers and should be as per the guide of the manufacturer.
THERMOMETERS
Health unit staffs use alcohol thermometers to monitor the temperature of vaccines in refrigerators, cold boxes and vaccine carriers.
VACCINES
- It is stored at a temperature of +2°C to+8°C.
- Restricted BCG and Measles vaccine should not be used beyond 6 hours.
Only use the diluents supplied and packaged by the manufacturer with the vaccine since the diluents is specifically designed for the needs of that vaccine, with respect to volume, HP level and chemical properties.
The diluents may be stored outside the cold chain as it may occupy the space of the fridge but keep diluents for at least 24 hours before use in the fridge to ensure that the vaccine and diluents are at +2°C to 8°C when being reconstituted. Otherwise, it can lead to thermal shock that is, the death of some or all the essential live organisms in the vaccine. Store all the diluents and droppers with the vaccine in the vaccine carrier during transportation. Diluents should not come in contact with the ice packs.
Any vials that are expired or frozen or with VVMS beyond the discard point, should not be kept in the cold chain.
Questions and Answers Read More »