Theories of Growth and Development
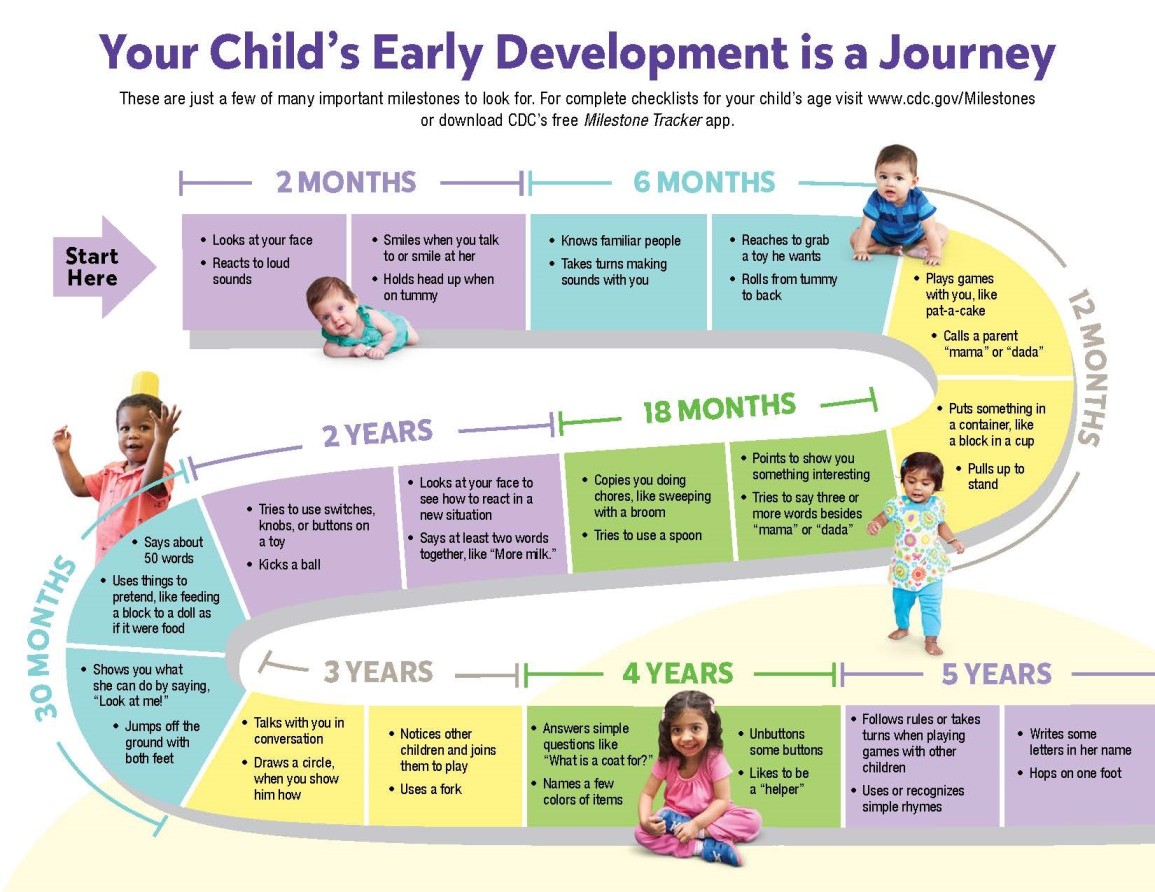
Growth involves physical changes in height and weight and appearance of the body, while development refers to a change in functional ability, such as cognitive, motor, and psychological aspects of the client.
Growth and development start from the time of conception and progress until a person dies. Growth and development theories provide a framework to understand this wide array of changes, and they help healthcare providers plan individualized care for clients based on their stage of development, and to provide anticipatory guidance for parents and caregivers.
Major growth and development theories include biophysical developmental theory by Gesell, psychosocial development theory by Erikson; cognitive development theory by Piaget; moral development theory by Kohlberg; and finally, the psychoanalytic development theory by Freud.
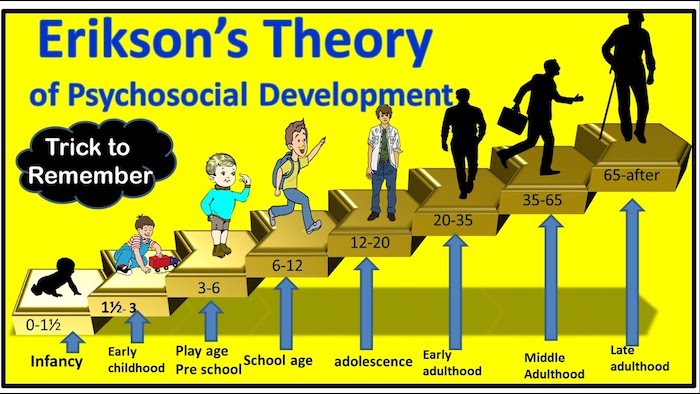
Erikson's Theory of Psychosocial Development
Erikson described development as a series of psychosocial crises that must be resolved at each stage for healthy personality development. The theory describes the major developmental issues or problems Erikson identified for each of the stages of development.
Infancy (Birth-1 year): Basic Trust vs. Mistrust
The central task is to establish a sense of basic trust in predominance to mistrust. Infants who find that their needs for food and comfort are constantly and effectively met, learn that the world is a safe and predictable place and that they can trust others. In contrast, a sense of mistrust may predominate in infants who do not receive constant care and those who experience long spells of discomfort. Mistrust creates formation barriers to interpersonal bond and interferes with the development of confidence, security, and assertiveness.
Example: A baby who is consistently fed when hungry and comforted when crying learns to trust their caregivers and the world around them. Conversely, a baby whose needs are inconsistently met may develop a sense of mistrust, becoming anxious or withdrawn, and hesitant to form secure attachments.
Toddlerhood (1-3 years): Autonomy vs. Shame and Doubt
A child must establish a sense of autonomy in this phase rather than shame & doubt. Autonomy is a kind of self-trust, a growing awareness that their behavior is under their control. This is the desired outcome, usually resulting in feelings like “I can do it”. Shame manifests as "I can do it but that is not nice," while doubt signifies "I cannot do it." It is hazardous when self-mistrust is carried on from infancy onwards, hindering their willingness to try new things.
Example: A toddler who is encouraged to choose their own clothes and pour their own juice (even if some spills) develops a sense of autonomy and pride in their growing independence. If caregivers are overly critical or controlling, the toddler might feel shame and doubt about their abilities, becoming hesitant to try new things or asserting their will.
Preschool (3-6 years): Initiative vs. Guilt
The central task is to develop a sense of initiative in predominance to the sense of guilt. Children explore what they can create and do with their developing motor, language, interpersonal, and social skills. Behavior is characterized by intrusiveness manifested in endless questions, noise, physical and intellectual exploration. Guilt is a major developmental hazard because what they try to do is difficult or unacceptable to people they wish to please, leading to feelings of unworthiness or inhibition.
Example: A preschooler who enthusiastically proposes a game of "hide-and-seek" and organizes their friends to play is demonstrating initiative and a growing sense of purpose. If their attempts to initiate play or ask questions are constantly dismissed, criticized, or punished, they might develop guilt over their desires and become less proactive or curious.
School Age (6-12 years): Industry vs. Inferiority
The central task is a sense of industry in predominance to a sense of inferiority. Industry means the child uses physical, cognitive (intellectual), and social skills and turns his attention to learning what he must know in preparation for success in the adult world. They learn self-worth as workers and producers. Inferiority is a negative self-concept that comes when children have difficulty in school, interpersonal relationships, or other expectations. They get discouraged and consider themselves inadequate, leading to a lack of motivation and self-esteem.
Example: A school-aged child who diligently works on a science project and feels proud of their completed work is developing industry and a sense of competence. If they consistently struggle in school despite effort, face constant criticism from peers or adults, or are told they are "not good enough," they may develop feelings of inferiority, leading to withdrawal or a reluctance to engage in new challenges.
Adolescence (12-19 years): Identity vs. Role Confusion
The central task is developing a sense of identity with the undesirable alternative being role confusion. Attachment of identity is a process of young people coming to feel that they are consistent with others, in terms of views (own views in relation to other people’s views). The major hazard is role confusion, which arises from rapid changes in the experience of self and from sometimes overwhelming numbers of possible ways to behave and roles to select, leading to an unstable self-concept.
Example: An adolescent who tries out for various sports teams, joins different clubs, and explores different academic subjects to discover their interests and values is forming their identity. Conversely, an adolescent who struggles to find their place, drifts between different social groups without a strong sense of belonging, or adopts an identity without personal reflection (e.g., simply conforming to peer pressure) may experience role confusion, feeling uncertain about who they are or where they are headed.
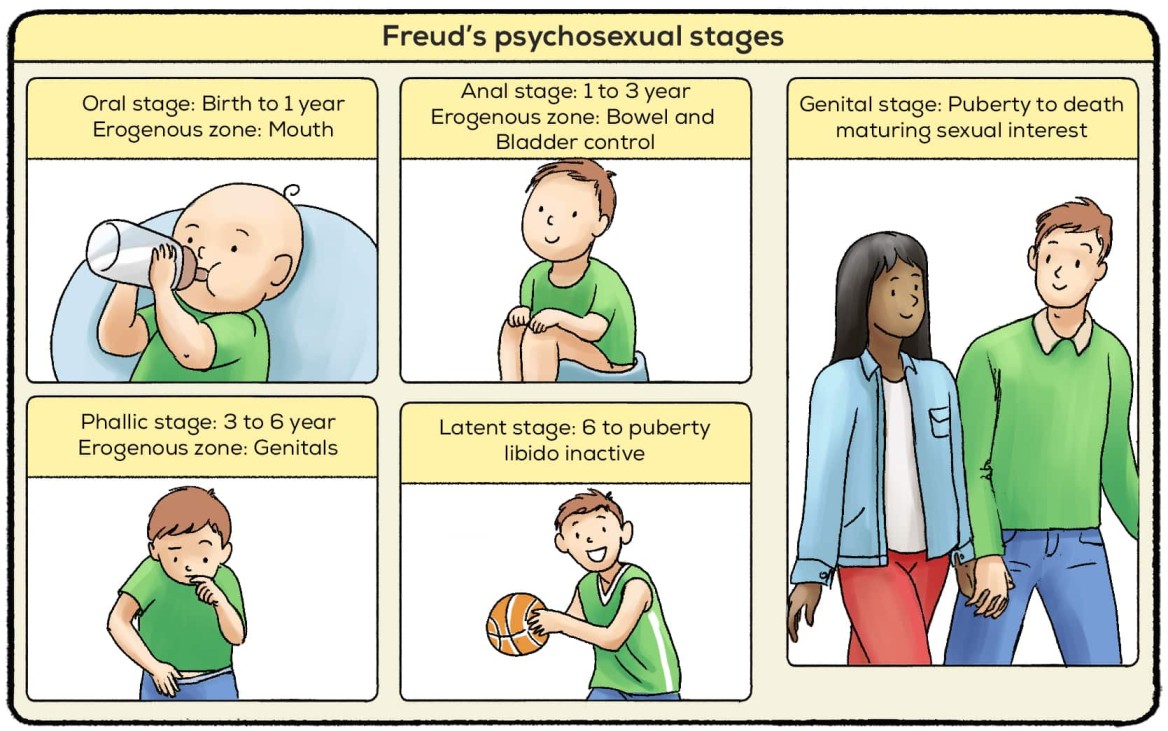
Freud's Theory of Psychosexual Development
Freud's theory revolves around sexual pleasure and has five stages: oral, anal, phallic, latency, and genital. It centers on the idea that personality develops through a series of stages where pleasure-seeking energies (libido) are focused on different erogenous zones.
Oral Stage (Birth-1 year)
This starts from birth until 1 year. During this stage, the primary source of pleasure and gratification is through the mouth, such as sucking and feeding. Freud believed that unresolved conflicts during this stage, such as weaning issues or oral fixation, could lead to oral-related behaviors in adulthood, such as overeating, smoking, excessive talking, or nail-biting, as an unconscious attempt to seek oral gratification.
Example: A baby putting everything in their mouth to explore their environment and soothe themselves is typical of the oral stage. An adult who constantly chews on pens, struggles with overeating when stressed, or smokes excessively might be experiencing an oral fixation due to unresolved issues from this stage.
Anal Stage (1-3 years)
The anal stage occurs between the ages of 1 and 3 years. This stage focuses on the child's pleasure and control over their bowel movements. It's associated with toilet training, where the child learns control. Freud believed that conflicts related to toilet training during this stage (e.g., overly strict or lenient approaches) could lead to fixation, resulting in anal-retentive behaviors (being overly neat, organized, punctual, and controlling) or anal-expulsive behaviors (being messy, disorganized, rebellious, and defiant).
Example: A toddler who insists on using the potty themselves and is very proud of their ability to control their bladder and bowels is demonstrating control related to the anal stage. An adult with an anal-retentive personality might be excessively neat, punctual, and controlling in their daily life, while an anal-expulsive person might be notoriously messy and disorganized, reflecting unresolved control issues.
Phallic Stage (3-6 years)
The phallic stage takes place between the ages of 3 and 6. During this stage, children develop a strong attachment to their opposite-sex parent (Oedipus complex for boys and Electra complex for girls) and become aware of gender differences. Freud believed that unresolved conflicts during this stage could lead to sexual and gender identity issues, difficulties with intimate relationships in adulthood, or issues like vanity and exhibitionism.
Example: A young boy expressing a strong attachment to his mother and showing some jealousy towards his father, characteristic of the Oedipus complex. Fixation from this stage could manifest in adulthood as vanity, exhibitionism, or difficulty forming stable, intimate relationships due to unresolved conflicts around gender roles and sexuality.
Latency Stage (6 years-Puberty)
The latent stage occurs from around 6 years old until the onset of puberty. During this stage, sexual desires and impulses are repressed, and the focus of the child's energy is channeled into developing social and intellectual pursuits like school, sports, and friendships with same-sex peers. Freud believed that this stage is relatively calm and that there are no significant conflicts or fixations, allowing for crucial skill development.
Example: A child focusing on developing friendships, excelling in school, and participating in extracurricular activities, with little overt interest in romantic relationships. This period allows for the development of social skills, learning, and the strengthening of non-sexual bonds.
Genital Stage (Puberty Onward)
The genital stage begins at the onset of puberty and continues into adulthood. This stage marks the reawakening of sexual desires and the development of mature sexual relationships. The focus of pleasure is on sexual intercourse and forming intimate relationships. Freud believed that successful resolution of previous stages' conflicts leads to healthy sexual development and the ability to form intimate, loving, and productive relationships.
Example: An adolescent beginning to explore romantic relationships and developing a sense of attraction towards others, leading to the formation of mature, loving relationships based on mutual respect and intimacy, rather than solely on self-gratification.
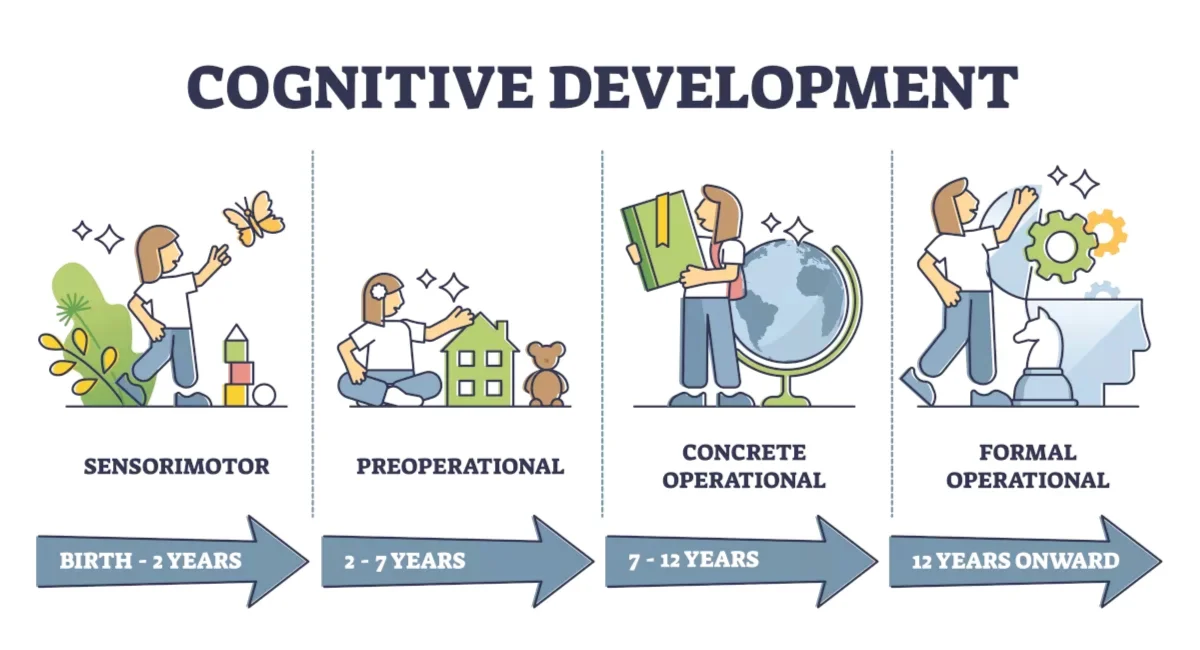
Piaget's Theory of Cognitive Development
Piaget's theory focuses on cognitive development and stages, including sensorimotor, preoperational thought, concrete operational, and formal operational. It explains how a child's thinking and intelligence progress through distinct stages, building on previous learning.
Sensorimotor Period (Birth-2 years)
The sensorimotor stage occurs from birth to around 2 years of age. During this stage, infants primarily learn about the world through their senses and motor actions. They develop object permanence, the understanding that objects continue to exist even when they are out of sight. Infants also engage in trial-and-error experimentation and begin to demonstrate intentional actions, moving from reflexive behaviors to goal-directed activities. Thinking is initially egocentric, focused on their own immediate perceptions.
Example: A baby crying when a toy is hidden under a blanket, then pulling the blanket away to find it, demonstrates developing object permanence. Prior to this, if the toy is out of sight, it's out of mind. They might also repeatedly drop a toy to see where it lands (trial-and-error experimentation).
Preoperational Period (2-7 years)
The preoperational stage typically occurs between the ages of 2 and 7. During this stage, children become more adept at using symbols, such as words and images, to represent objects and events. They engage in pretend play and develop language skills. However, children in this stage often struggle with logical reasoning, exhibiting egocentrism (difficulty understanding other people's perspectives), magical thinking (believing their thoughts can cause events), and animism (attributing life to inanimate objects). They also cannot yet grasp the concept of conservation (e.g., that a quantity of liquid remains the same in a differently shaped glass).
Example: A child believing their doll feels sad when it falls (animism), or insisting that a tall, narrow glass has more juice than a short, wide one, even if both contain the same amount (lack of conservation). They might also cover their eyes and think if they can't see you, you can't see them (egocentrism), demonstrating their inability to decenter their thinking.
Concrete Operational Period (7-11 years)
The concrete operational stage takes place between the ages of 7 and 11. During this stage, children become capable of concrete, logical thinking. They can understand conservation, the idea that certain properties of objects remain the same despite changes in appearance. Children also develop the ability to classify objects into different categories, understand reversibility (actions can be undone), and engage in more systematic problem-solving, but their reasoning is still tied to concrete, tangible objects and events. They struggle with abstract concepts.
Example: A child understanding that if you pour water from a tall, thin glass into a short, wide glass, the amount of water remains the same (conservation). They can also sort objects by multiple features (e.g., color and size) and solve simple math problems mentally, but might struggle with hypothetical questions like "What if humans had wings and could fly?"
Formal Operational Period (11 years Onward)
The formal operational stage begins around the age of 11 and extends into adulthood. During this stage, individuals develop abstract thinking and can reason hypothetically. They can engage in deductive reasoning (drawing specific conclusions from general principles), logical thinking, and hypothetical-deductive reasoning (forming hypotheses and testing them systematically). They can also think about multiple possibilities, engage in more complex problem-solving, and consider moral, philosophical, and social issues in depth.
Example: A teenager debating complex social issues like climate change or justice, considering different perspectives and hypothetical scenarios, or planning a multi-step science experiment by thinking through all possible variables and outcomes. They can also understand metaphors and abstract mathematical concepts.
Piaget believed that individuals progress through these stages in a fixed sequence, with each stage building upon the previous one. He proposed that cognitive development occurs through a process of assimilation (integrating new information into existing mental structures or schemas) and accommodation (modifying existing schemas to fit new information or creating new ones).
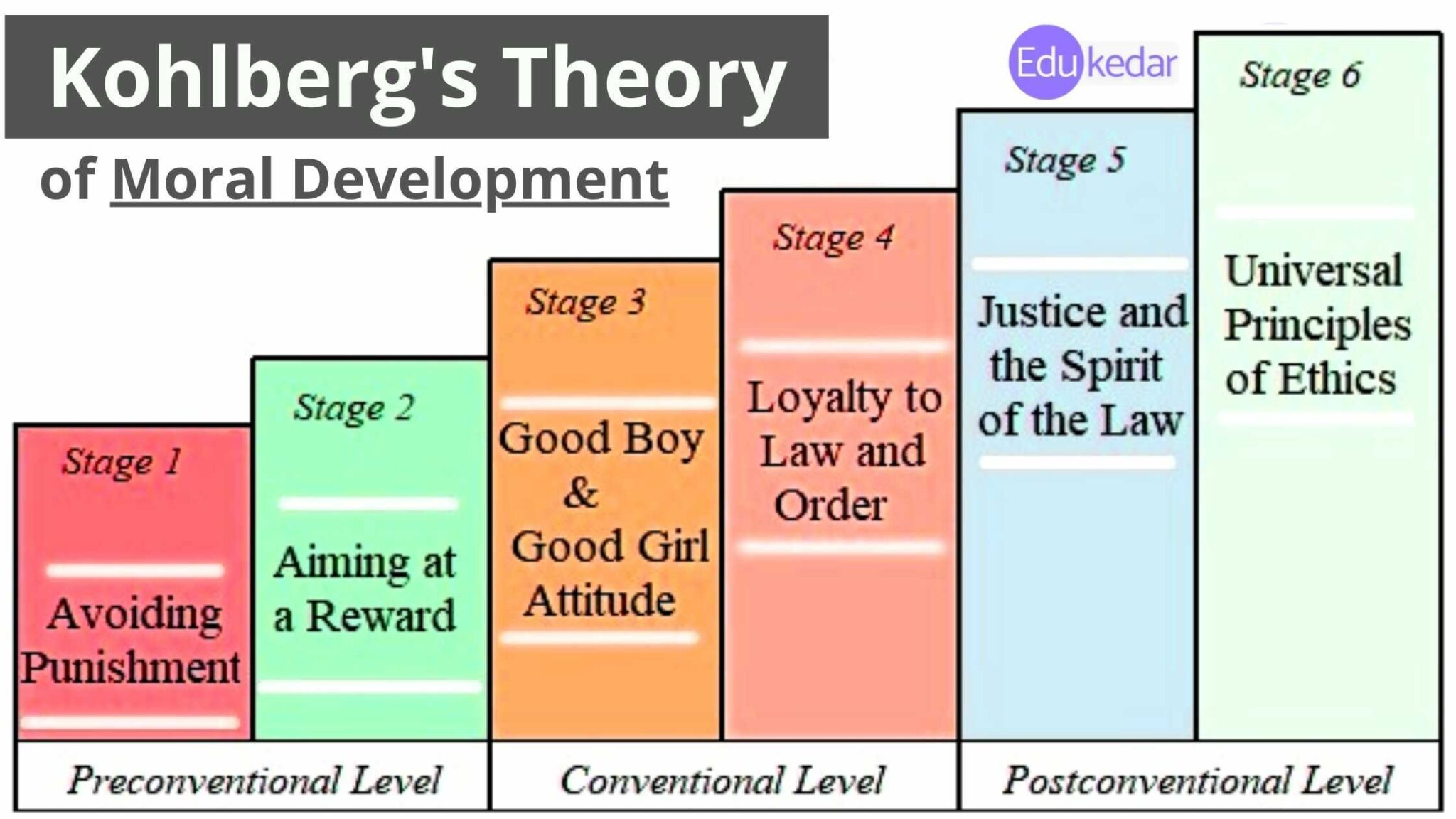
Kohlberg's Theory of Moral Development
Kohlberg's theory explores moral development through stages of moral reasoning, focusing on how people think about right and wrong and the justifications they use for their moral decisions.
Level 1: Preconventional Morality (Toddler to School Age)
Morality is externally controlled. Rules are obeyed to avoid punishment or receive rewards. This level is characteristic of young children, but adults can also exhibit this type of reasoning.
- Stage 1: Obedience and Punishment Orientation: At this stage, individuals focus on avoiding punishment and obeying authority figures. They make moral decisions based on the direct consequences of their actions and the fear of being punished. Morality is about "might makes right."
Example: A child not stealing a cookie because they know they will get a time-out if caught, or a child refraining from hitting another child solely to avoid being punished by a parent, regardless of whether hitting is inherently wrong.
- Stage 2: Individualism and Exchange: In this stage, individuals start to consider their own interests and begin to understand that others have their own needs and desires. Moral decisions are driven by self-interest and the expectation of receiving something in return, often characterized as "you scratch my back, I'll scratch yours."
Example: A child sharing their toy with another child because they expect the other child to share their toy in return, or a child offering to help with chores only if they get paid, viewing morality as a transaction.
Level 2: Conventional Morality (School Age to Adolescence)
Conformity to social rules is important, but not for self-interest. The focus is on maintaining social order, fulfilling duties, and fostering positive relationships within a group or society. Most adolescents and adults reason at this level.
- Stage 3: Good Interpersonal Relationships: The "good boy/good girl" orientation. At this stage, individuals value social harmony and seek approval from others. They make moral decisions based on the desire to be seen as a good person by their family, friends, or community, and to maintain positive relationships.
Example: A student following classroom rules because they want to be seen as a "good student" by their teacher and peers, or a teenager refraining from cheating because they want their friends to see them as honest and trustworthy, valuing social approval.
- Stage 4: Maintaining the Social Order: In this stage, individuals focus on following rules and maintaining social order. They make moral decisions based on a sense of duty, respect for authority, and the need to uphold societal norms and laws for the greater good of society. Laws are seen as fixed and necessary for stability.
Example: A citizen paying their taxes because they understand it is their duty to uphold the laws of their country and maintain societal order, or a driver obeying traffic laws because it is the rule and necessary for public safety, even if no one is watching.
Level 3: Postconventional Morality (Adolescence and Adulthood)
Morality is defined in terms of abstract principles and values that apply to all situations and societies. Individuals at this level think beyond societal conventions and consider universal ethical principles. Not everyone reaches this level of moral reasoning.
- Stage 5: Social Contract and Individual Rights: At this stage, individuals recognize that different societies may have different moral standards, and they begin to question and evaluate these standards based on democratic principles. Moral decisions are based on principles of fairness, justice, and the protection of individual rights, understanding that laws are social contracts that can be changed if they no longer serve the common good.
Example: An individual advocating for changes to a law they believe is unfair, even if it is currently legal, because it violates fundamental human rights and the societal contract for justice, such as participating in peaceful protests against discriminatory policies or advocating for legal reform.
- Stage 6: Universal Principles: In this final stage, individuals develop their own set of moral principles that are based on universal ethical principles, such as justice, equality, and respect for human dignity. Moral decisions are guided by these principles, which are considered valid for all humanity, even if they conflict with societal norms or laws, and even if it means personal risk.
Example: An activist dedicating their life to fighting for human rights globally, even in the face of personal risk or legal consequences, because they believe in the universal principle of justice for all, like a civil rights leader who non-violently resists unjust laws based on deep moral convictions and a commitment to equality.