HAEMORRHAGE: Nursing Lecture Notes
HAEMORRHAGE: Nursing Lecture Notes
Haemorrhage, commonly known as bleeding, is the loss of blood from the circulatory system, specifically from blood vessels. It is a critical medical condition that, if uncontrolled, can lead to severe physiological compromise and death. The body possesses intrinsic defence mechanisms, primarily through the process of clotting (hemostasis), to prevent excessive blood leakage. However, these mechanisms can be deficient due to underlying diseases, absence of essential clotting factors, or the use of anticoagulant medications.
Types of Haemorrhage
Haemorrhage is classified based on several key characteristics to aid in diagnosis, prognosis, and management. These classifications include:
- The type of blood vessel involved.
- The location or situation of the haemorrhage.
- The time of occurrence or duration of the haemorrhage.
Classification by Blood Vessels Involved
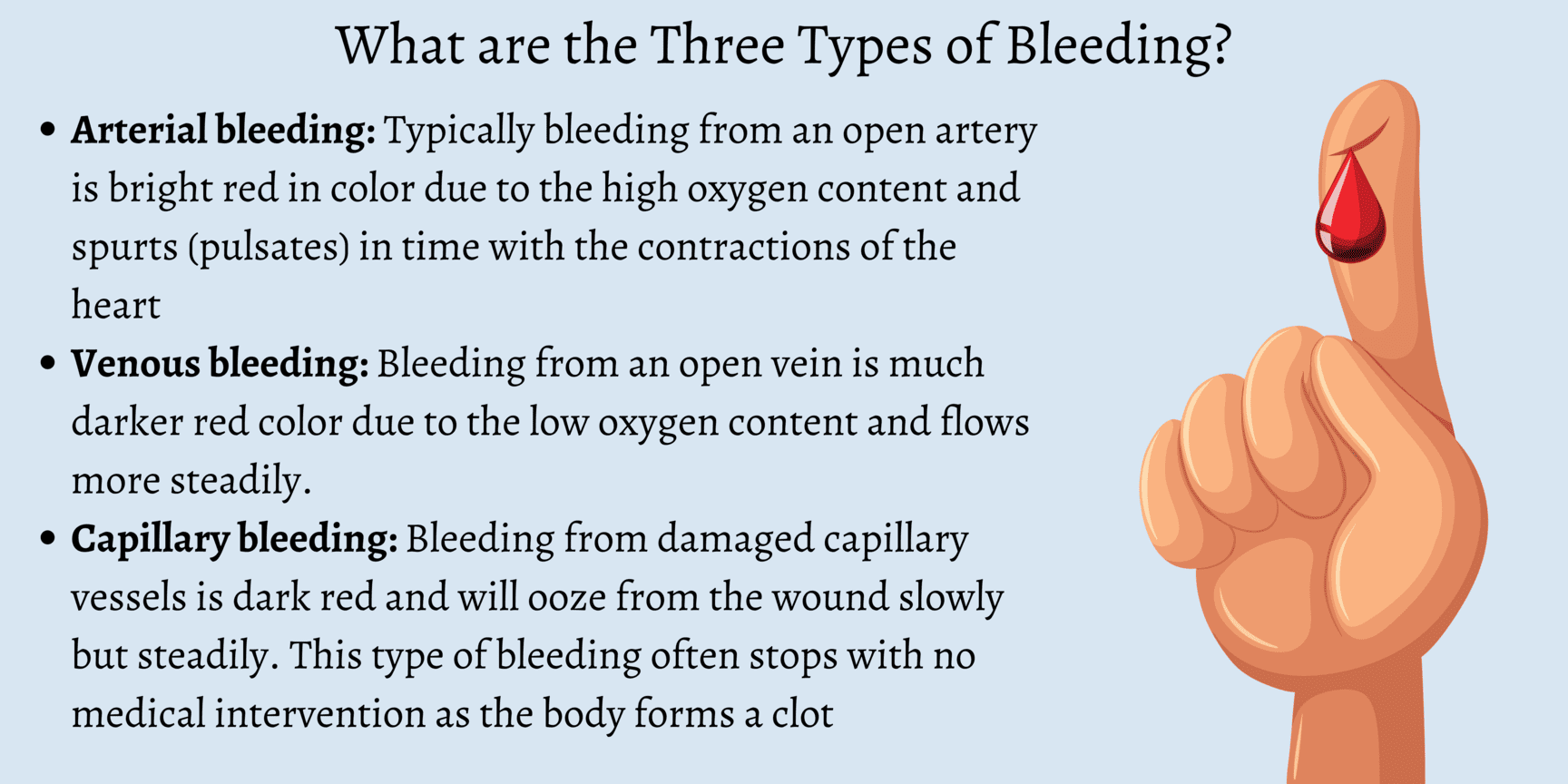
The characteristics of bleeding often provide clues as to which type of blood vessel has been compromised:
1. Arterial Haemorrhage:Classification by Time or Duration of Haemorrhage
The timing of haemorrhage relative to an injury or surgical procedure provides important diagnostic and prognostic information:
1. Primary Haemorrhage:- Increased intravascular pressure due to actions such as coughing or vomiting.
- Increased venous pressure.
- Physical excitement or administration of stimulant drugs.
- Sepsis: Bacterial infection leading to inflammation and enzymatic destruction of vessel walls.
- Enzymatic Action: For example, the action of pepsin on a bleeding peptic ulcer, eroding the vessel.
- Mechanical Pressure: Persistent pressure from a drainage tube or foreign body (e.g., bone fragment) eroding a vessel.
- Presence of Carcinoma: Malignant tumors can erode blood vessels, leading to chronic or acute bleeding.
Classification by Situation or Location of Haemorrhage
This classification distinguishes whether the blood loss is visible externally or contained within body cavities:
1. External or Revealed Haemorrhage:- Definition: This is bleeding that is directly visible, either from an open wound on the body surface or from a natural body orifice (e.g., epistaxis from the nose, hematemesis from vomiting blood, melena/hematochezia from the rectum).
- Visibility: Blood is immediately apparent and can be quantified relatively easily.
- Definition: This refers to bleeding that occurs into an internal body cavity or tissue space, where the blood loss is not immediately visible externally.
- Locations: Common sites include the peritoneal cavity (e.g., ruptured spleen), pleural cavity (e.g., hemothorax), retroperitoneal space, lumen of hollow organs (e.g., intestines, stomach, bladder), or within the tissues of a limb (e.g., large hematoma).
- Diagnosis: Since the bleeding is concealed, diagnosis relies heavily on the patient's symptoms and signs of hypovolemia and shock. It may be "revealed" later if the blood exits the body (e.g., vomited blood, blood passed per rectum) or by the formation of bruising and swelling on the surface of the body.
Clinical Picture: Signs and Symptoms of Haemorrhage
The clinical presentation of haemorrhage varies depending on the amount, rate, and duration of blood loss. Symptoms and signs reflect the body's compensatory mechanisms attempting to maintain vital organ perfusion, followed by the failure of these mechanisms as blood loss becomes severe. The progression is often categorized into stages of shock.
Early Symptoms and Signs (Compensatory Stage / Class I & II Haemorrhage)
These signs indicate the body's initial attempts to compensate for blood loss (up to 15-30% of blood volume). The sympathetic nervous system is activated.
Neurological/Mental Status:- Restlessness and Anxiety: Often one of the earliest signs, resulting from cerebral hypoperfusion and increased catecholamine release.
- Increased Thirst: Due to fluid shifts and activation of the renin-angiotensin-aldosterone system.
- Slightly Increased Pulse Rate (Mild Tachycardia): The heart beats faster to maintain cardiac output despite reduced blood volume.
- Blood Pressure (BP) Maintained or Slightly Lowered: Due to peripheral vasoconstriction attempting to shunt blood to vital organs. Orthostatic hypotension may be present.
- Pallor (Paleness): Due to vasoconstriction and reduced blood flow to the skin.
- Coldness: Skin feels cool to the touch (subnormal temperature, e.g., 36.9°C), also due to peripheral vasoconstriction.
- Slightly Clammy Skin: Due to increased sweating from sympathetic activation.
- Oliguria (Reduced Urine Output): The kidneys conserve fluid and blood flow is shunted away from them.
Symptoms and Signs of Severe Haemorrhage (Decompensatory & Irreversible Stages / Class III & IV Haemorrhage)
These signs manifest when compensatory mechanisms are overwhelmed, and blood loss exceeds 30-40% of total blood volume. This leads to profound organ hypoperfusion and cellular dysfunction.
Neurological/Mental Status:- Lethargy, Drowsiness, Confusion: Progressive worsening of cerebral hypoperfusion.
- Decreased Responsiveness: Leading to stupor and eventually coma.
- Blindness, Tinnitus (Buzzing in the Ears): Severe cerebral ischemia.
- Extreme Pallor: Face becomes ashen white, indicating severe cutaneous vasoconstriction and lack of circulating blood.
- Profound Coldness: Core body temperature may drop significantly (e.g., 36°C or lower), indicating severe hypothermia and circulatory collapse.
- Pulse: Very rapid in rate (severe tachycardia, >120 bpm), thready in volume (barely palpable), and often irregular in rhythm, indicating a severely compromised cardiac output.
- Blood Pressure: Extremely low (severe hypotension), indicating failed compensation and impending circulatory collapse.
- Low Venous Pressure: Due to severely depleted intravascular volume.
- Air Hunger: The patient gasps for breath, with respirations becoming rapid and sighing (Kussmaul-like breathing), as the body attempts to compensate for metabolic acidosis resulting from anaerobic metabolism.
- Dyspnea: Difficult or labored breathing.
- Diminished Urine Volume: Progressing to anuria (no urine production), which may result in acute renal failure due to prolonged renal ischemia.
- Extreme Thirst: Persists and worsens.
- Metabolic Acidosis: Due to widespread anaerobic metabolism and lactic acid accumulation.
- Eventual Multi-Organ Dysfunction Syndrome (MODS): Leading to irreversible organ damage and death.
Management of Haemorrhage: Principles of Care
Effective management of haemorrhage is time-sensitive and aims to stop the bleeding, restore circulating blood volume, optimize tissue perfusion, and treat any underlying coagulopathy.
Immediate Priorities (The "ABCDE" Approach):
- Airway: Ensure a patent airway. If the patient's consciousness is compromised, intubation may be necessary to protect the airway and facilitate ventilation.
- Breathing: Assess respiratory effort and oxygenation. Administer high-flow oxygen (e.g., via non-rebreather mask) to maximize oxygen delivery to tissues. Provide ventilatory support if needed.
- Circulation: This is paramount in haemorrhage.
- Direct Pressure: Apply direct pressure to any visible external bleeding site.
- Large-Bore IV Access: Establish at least two large-bore intravenous (IV) lines for rapid fluid and blood product administration.
- Fluid Resuscitation: Begin rapid infusion of crystalloid solutions (e.g., 0.9% Normal Saline, Lactated Ringer's) while awaiting blood products.
- Blood Transfusion: Initiate blood product transfusion (e.g., packed red blood cells, fresh frozen plasma, platelets) as soon as possible, especially for significant haemorrhage. Consider massive transfusion protocols if appropriate.
- Identify and Stop Bleeding: Promptly identify the source of bleeding and take definitive steps to control it (e.g., surgical intervention, endoscopic intervention, interventional radiology embolization, tourniquet for severe limb trauma).
- Disability (Neurological Status): Assess the patient's level of consciousness (e.g., AVPU scale, GCS) to monitor cerebral perfusion.
- Exposure and Environment: Fully expose the patient to identify all injuries and bleeding sites. Prevent hypothermia by covering the patient with warm blankets, as hypothermia exacerbates coagulopathy.
Ongoing Management and Monitoring:
- Continuous Monitoring: Continuously monitor vital signs (heart rate, blood pressure, respiratory rate, oxygen saturation), ECG, and urine output. An arterial line may be used for continuous blood pressure monitoring.
- Laboratory Monitoring: Serial blood tests, including complete blood count (CBC), electrolytes, coagulation profile (PT, PTT, fibrinogen), blood type and cross-match, and lactate levels (to assess tissue perfusion and acidosis).
- Temperature Control: Maintain normothermia; hypothermia can worsen coagulopathy and acidosis.
- Correct Coagulopathy: Administer specific clotting factors, cryoprecipitate, or prothrombin complex concentrates (PCCs) as indicated, especially if the patient is on anticoagulants or has a pre-existing coagulopathy. Consider tranexamic acid (TXA) as an antifibrinolytic.
- Pain Management: Administer analgesia cautiously, considering its potential effects on blood pressure and mental status.
- Prevent Complications: Implement strategies to prevent acute kidney injury, acute respiratory distress syndrome (ARDS), disseminated intravascular coagulation (DIC), and multi-organ dysfunction syndrome (MODS).
- Definitive Treatment: Address the underlying cause of the haemorrhage once the patient is stabilized.
Management and Interventions
Effective management of haemorrhage is time-sensitive and requires a multi-faceted approach. The primary goals are to:
- Arrest the haemorrhage: Control and stop the bleeding at its source.
- Restore blood volume: Replenish lost blood and fluids to maintain adequate circulation.
- Manage the extravasated blood: Address the consequences of blood accumulating outside the vessels, and support the body's physiological responses.
I. Arrest of Haemorrhage: Controlling the Bleeding Source
The methods to control bleeding depend on whether the haemorrhage is revealed (external) or concealed (internal).
A. Arrest of Revealed (External) Haemorrhage
Most forms of external haemorrhage can be controlled by applying pressure directly or indirectly to the bleeding site. The choice of method depends on the severity and nature of the bleeding:
Direct Pressure (Pad & Bandage):- Method: This is the simplest, most effective, and often the first line of treatment. Apply a clean, sterile pad directly to the bleeding wound and secure it firmly with a bandage.
- Mechanism: Direct pressure compresses the bleeding vessels, allowing clots to form.
- Advantages: Highly effective, causes minimal damage, and can be performed quickly.
- Method: Fingers are used to apply firm pressure over the pressure point of an artery that supplies the wounded area, proximal to the injury.
- Mechanism: Temporarily occludes the main arterial blood supply to the limb or area.
- Application: Commonly used in areas where direct pressure might be difficult or less effective, such as on the neck (e.g., carotid artery pressure point in severe facial bleeding). It provides temporary control until definitive measures can be taken.
- Method: Raising the injured limb above the level of the heart.
- Mechanism: Reduces hydrostatic pressure in the veins, which can help control venous bleeding.
- Application: A classical method for controlling bleeding from ruptured varicose veins of the leg or other venous injuries.
- Method: A constricting band applied proximally to an injury on a limb. Tourniquets include devices like the Samway anchor, Esmarch’s Elastic bandage, or inflatable cuffs.
- Application: **Use ONLY for the control of heavy, life-threatening bleeding from a limb when other methods have failed or are not feasible.**
- Dangers: If left on for more than 30 minutes, it carries significant risks such as gangrene, nerve damage, and reperfusion injury upon removal. Requires careful application and monitoring.
- Method: Surgically tying off the bleeding vessel with sutures.
- Application: Necessary if bleeding continues despite less invasive measures or for larger vessels.
- Method: Application of heat (via electrical current) to the bleeding point to seal small vessels.
- Application: Commonly used in surgical settings for precise haemostasis.
- Method: Deliberate occlusion of bleeding blood vessels by introducing embolic materials (e.g., coils, particles, glues) through an angiographic catheter under imaging guidance.
- Application: Common in controlling bleeding from internal sources like oesophageal varices, gastric ulcers, or arterial bleeds in inaccessible locations. Examples of emboli include lyophilized human dura mater.
- Method: Insertion of sterile gauze or specialized hemostatic dressings into a wound or cavity to apply internal pressure.
- Application: A temporary measure for very severe bleeding, often used in theatre to control sudden haemorrhage or for diffuse bleeding that is difficult to ligate.
- Method: Substances capable of causing bleeding to stop when applied locally.
- Examples: Include topical thrombin, collagen, gelatin sponges, oxidized regenerated cellulose (Oxycel). Some natural substances like snake venom or adrenaline can also act as styptics.
- Application: Used locally in certain cases for low-pressure bleeding from capillaries and venules.
B. Arrest of Concealed (Internal) Haemorrhage
Controlling internal haemorrhage is more challenging as direct pressure is often not possible. Management focuses on internal pressure, addressing the underlying cause, and enhancing coagulation.
Surgical Ligation/Repair:- Method: Direct surgical intervention to identify and ligate or repair the bleeding vessel.
- Application: Often the definitive treatment for ruptured organs (e.g., ruptured spleen, liver laceration) or major vessel injuries.
- Method: Removing blood clots from a hollow organ can allow it to contract and seal bleeding vessels.
- Application: For severe bleeding from the bladder, passing a catheter and emptying it of clots can help the bladder contract and tamponade bleeding.
- Method: Administration of medications that promote vasoconstriction.
- Examples:
- Adrenaline (Epinephrine): Can be added to saline or sodium bicarbonate for washing out an organ to encourage vessel constriction (e.g., in some urological procedures, often done two-hourly).
- Ergometrine: Used post-partum to stimulate uterine contractions and reduce bleeding after the birth of the placenta.
- Vasopressin (Pitressin): Can be used effectively in the control of bleeding from oesophageal varices by causing splanchnic vasoconstriction.
- Method: Administering agents that correct clotting factor deficiencies.
- Application: Very valuable when the mechanism of clotting is deficient.
- Vitamin K (IM): Important in jaundiced patients or those with liver dysfunction who are bleeding due to impaired synthesis of Vitamin K-dependent clotting factors.
- Factor VIII Concentrate: Indicated in patients with Haemophilia A.
- Fresh Frozen Plasma (FFP), Platelets, Cryoprecipitate: Administered to provide clotting factors or platelets as needed.
- Method: Using specialized materials to provide internal pressure or promote clotting.
- Examples:
- Gauze soaked in adrenaline can be effective in certain sites (e.g., nasal packing for epistaxis).
- Oxycel (oxidized regenerated cellulose), Fibrin glue, or a piece of the patient’s own crushed muscle can be used to promote local haemostasis in surgical beds.
- Method: Systemic antibiotic administration.
- Application: Essential in secondary haemorrhage, especially when caused by infection, to control sepsis which contributes to vessel wall breakdown.
- Method: Applying pressure from within a lumen using an inflatable balloon.
- Application: Applied by the balloon of a triluminal tube (e.g., Sengstaken-Blakemore tube) in bleeding oesophageal varices or by the balloon of a Foley catheter in a post-prostatectomy cavity.
- Method: Use of medications that inhibit the breakdown of blood clots.
- Example: Achieved by the use of Tranexamic Acid (TXA), which stabilizes clots and reduces bleeding in various conditions.
II. Restoration of Blood Volume and Oxygen Carrying Capacity
Replacing lost fluid and blood is crucial to maintain adequate circulation and tissue perfusion.
- Airway: Ensure a patent airway. Intubation may be necessary if consciousness is compromised to protect the airway and facilitate ventilation.
- Breathing: Assess respiratory effort and oxygenation. Administer high-flow oxygen (e.g., via non-rebreather mask) to maximize oxygen delivery to tissues. Provide ventilatory support if needed.
- Circulation: This is paramount.
- Large-Bore IV Access: Establish at least two large-bore intravenous (IV) lines (e.g., 14-16 gauge) for rapid fluid and blood product administration. Central venous access may be needed in severe cases.
- Fluid Resuscitation: Begin rapid infusion of crystalloid solutions (e.g., 0.9% Normal Saline, Lactated Ringer's) as initial volume expanders while awaiting blood products. Monitor response.
- Blood Transfusion: Initiate blood product transfusion (e.g., packed red blood cells to increase oxygen-carrying capacity; fresh frozen plasma for clotting factors; platelets for thrombocytopenia) as soon as possible, especially for significant haemorrhage. Consider massive transfusion protocols (MTP) for severe, ongoing bleeding.
- Disability (Neurological Status): Assess the patient's level of consciousness (e.g., AVPU scale, GCS) to monitor cerebral perfusion and detect neurological changes.
- Exposure and Environment: Fully expose the patient to identify all injuries and bleeding sites. Prevent hypothermia by covering the patient with warm blankets, as hypothermia significantly exacerbates coagulopathy and metabolic acidosis.
- Continuous Monitoring: Continuously monitor vital signs (heart rate, blood pressure, respiratory rate, oxygen saturation), ECG for cardiac rhythm, and hourly urine output via an indwelling urinary catheter (a sensitive indicator of renal perfusion). An arterial line provides continuous and accurate blood pressure monitoring.
- Laboratory Monitoring: Frequent serial blood tests are essential:
- Complete Blood Count (CBC): To monitor hemoglobin and hematocrit.
- Electrolytes and Renal Function Tests: To assess fluid and electrolyte balance and kidney function.
- Coagulation Profile: PT, PTT, fibrinogen to assess clotting status.
- Blood Type and Cross-match: For blood product compatibility.
- Lactate Levels: To assess tissue perfusion and severity of acidosis.
- Arterial Blood Gases (ABGs): For oxygenation, ventilation, and acid-base balance.
- Temperature Control: Actively maintain normothermia using warming blankets and warmed fluids.
- Correct Coagulopathy: Actively manage any identified clotting factor deficiencies by administering specific factor concentrates, cryoprecipitate, or prothrombin complex concentrates (PCCs), especially if the patient is on anticoagulants or has a pre-existing coagulopathy.
A. Nursing Diagnoses for Patients with Haemorrhage (Examples)
Nursing diagnoses are clinical judgments about individual, family, or community responses to actual or potential health problems/life processes. For haemorrhage, they often focus on perfusion, fluid balance, and anxiety.
- Deficient Fluid Volume related to active blood loss, as evidenced by hypotension, tachycardia, decreased urine output, cool/clammy skin, and altered mental status.
- Ineffective Tissue Perfusion (specify: Cerebral, Cardiopulmonary, Renal, Gastrointestinal, Peripheral) related to hypovolemia and decreased oxygen-carrying capacity, as evidenced by altered mental status, oliguria, delayed capillary refill, weak pulses, or abnormal ABGs.
- Decreased Cardiac Output related to reduced preload (due to blood loss), as evidenced by hypotension, tachycardia, and signs of hypoperfusion.
- Risk for Shock related to uncompensated blood loss.
- Anxiety/Fear related to threat to health status, perceived loss of control, and critical illness.
- Risk for Imbalanced Body Temperature (Hypothermia) related to hypovolemia, decreased metabolic rate, and rapid fluid resuscitation.
- Acute Pain related to injury or invasive procedures, as evidenced by patient report, guarding behavior, or vital sign changes.
B. Nursing Interventions for Haemorrhage
Nursing interventions are actions designed to achieve patient outcomes related to the nursing diagnoses. These are broad categories and require specific adaptation based on the individual patient's condition and the type of haemorrhage.
- Prioritize ABCs and Rapid Response:
- Immediately assess and maintain airway patency, breathing effectiveness, and circulation.
- Activate rapid response team/code team according to facility protocol for acute haemorrhage.
- Stay with the patient; do not leave an acutely bleeding patient unattended.
- Control Bleeding (Nursing Actions):
- Apply direct, firm pressure to any external bleeding site using sterile dressings. Elevate the affected limb if appropriate.
- Prepare and assist with tourniquet application if indicated for life-threatening limb haemorrhage (monitor time).
- Prepare for and assist with surgical or interventional radiology procedures for definitive bleeding control.
- Ensure all lines, drains, and tubes are securely in place to prevent accidental dislodgement.
- Fluid and Blood Volume Resuscitation:
- Establish and maintain multiple large-bore IV access sites.
- Administer prescribed IV fluids (crystalloids) and blood products (PRBCs, FFP, platelets) rapidly, using rapid infusers if available, and monitor patient response.
- Monitor for signs of fluid overload or transfusion reactions.
- Ensure warmed fluids and blood products are used to prevent hypothermia.
- Continuous Assessment and Monitoring:
- Monitor vital signs (BP, HR, RR, SpO2, Temp) continuously (e.g., every 5-15 minutes or more frequently in acute phase).
- Assess level of consciousness (LOC) and neurological status frequently for signs of cerebral hypoperfusion.
- Monitor hourly urine output via indwelling catheter; report output less than 0.5 mL/kg/hour.
- Assess skin color, temperature, and capillary refill for signs of peripheral perfusion.
- Monitor dressing for increasing saturation and measure blood loss (e.g., weigh pads, assess drainage in collection devices).
- Review and trend laboratory results (Hgb, Hct, lactate, coagulation studies, electrolytes).
- Assess for signs of internal bleeding if concealed haemorrhage is suspected (e.g., increasing abdominal girth, distension, pain, bruising, changes in bowel sounds, persistent hypotension despite fluid resuscitation).
- Oxygenation and Respiratory Support:
- Administer oxygen as prescribed to maintain SpO2 >94%.
- Monitor respiratory effort and patterns; prepare for ventilatory support if respiratory distress or failure occurs.
- Maintain Normothermia:
- Use warming blankets, warmed IV fluids, and control room temperature to prevent and treat hypothermia.
- Pain and Anxiety Management:
- Administer analgesics as prescribed, carefully monitoring for effects on vital signs.
- Provide emotional support, calm reassurance, and clear, concise explanations to the patient and family. Address their fears and anxiety.
- Create a calm environment as much as possible.
- Prevent Complications:
- Maintain strict asepsis for all invasive procedures (IV insertion, catheter care) to prevent infection.
- Implement measures to prevent pressure injuries due to immobility and hypoperfusion.
- Initiate DVT prophylaxis as soon as appropriate and ordered.
- Monitor for signs of acute kidney injury or multi-organ dysfunction.
- Documentation and Communication:
- Accurately and timely document all assessments, interventions, and patient responses.
- Communicate effectively and frequently with the interdisciplinary team (physicians, respiratory therapists, lab, blood bank) regarding patient status and changes.
- Handover critical information thoroughly.
HAEMORRHAGE: Nursing Lecture Notes Read More »
BURNS LECTURE NOTES
BURNS
Burns are injuries to the skin due to extremes of temperature i.e cold or hot, chemicals or radiations. Burns occur when there is injury to the tissues of the body caused by heat, chemicals, electric current or radiations.
Anatomical review of the skin.
- Skin is the largest organ of the body that protects against injury, loss of fluid and from infection.
- It also maintains a constant body temperature with sebum, hair follicles. The skin has got two layers;
- -Epidermis (outer layer) and -Dermis (inner layer).
- Under the skin is sebaceous tissue mainly fat.
- The top part of the skin (epidermis) is made up of fat cells which are constantly shed and are replaced by new cells which come from underneath the layer.
- The epidermis has got an oily layer called sebum produced by sebaceous gland. It prevents heat loss (it thickens when it’s cold).
- Sebum makes the skin water proof, makes skin supplies plethoric.
- The dermis contains blood vessels, nerve, muscles, sweat glands, hair follicles, sebaceous glands; the ends of the sensory nerves in the dermis register sensation from the body surface.
TYPES OF BURNS
Thermal burns
These can be caused by flame, flash, scald, or contact with hot object.
Chemical burns
These are the result of tissue injury and destruction from necrotizing substance. Chemical burns are most commonly caused by acids; however alkalis can also cause a burn e.g. cleaning agents, drain cleaners and lye’s.
Electrical burns
These result from coagulation necrosis that is caused by intense heat generated from an electrical current. It can also result from direct damage to nerves and vessels causing tissue anoxia and death. The severity of the electrical injury depends on the amount of voltage, tissue resistance, current pathways, and surface area in contact with the current and on the length of time the current flow was sustained.
Smoke and inhalation injury
It results from inhalation of hot air or noxious chemicals that can cause damage to the tissues of the respiratory tract. Smoke inhalation injuries are an important determinant of motility in the fire victims.
- Carbon monoxide poisoning.
- Inhalation injury above the glottis, it is thermally produced and above is chemically produced.
- Inhalation injury below the glottis is related to the length of exposure to smoke or toxic fumes.
Cold thermal injury
These are due to extreme cold temperatures e.g. frost bite, freezing metals.
Irradiations
I.e. sun burn, radiation therapy, medical therapy e.g. treatment of cancer of the cervix.
SCALDS
Are injuries caused by moist heat, and hot liquids?
CLASSIFICATION OF BURN INJURY
Burns are classified according to;
- Depth of the burn.
- Extent of the burn.
- Location of the burn.
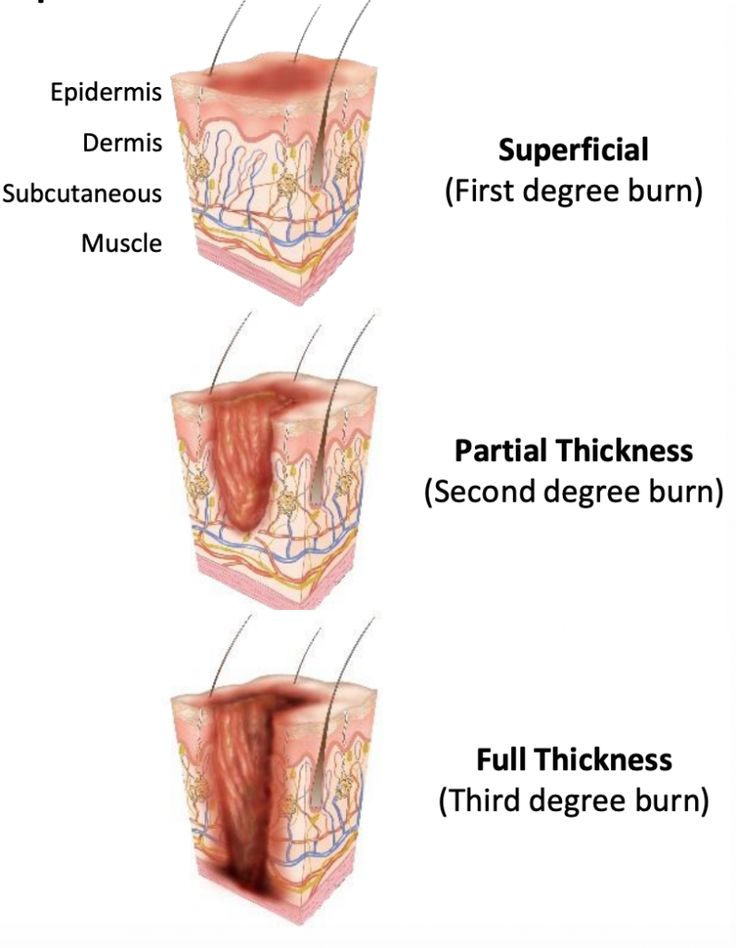
DEPTH OF THE BURN
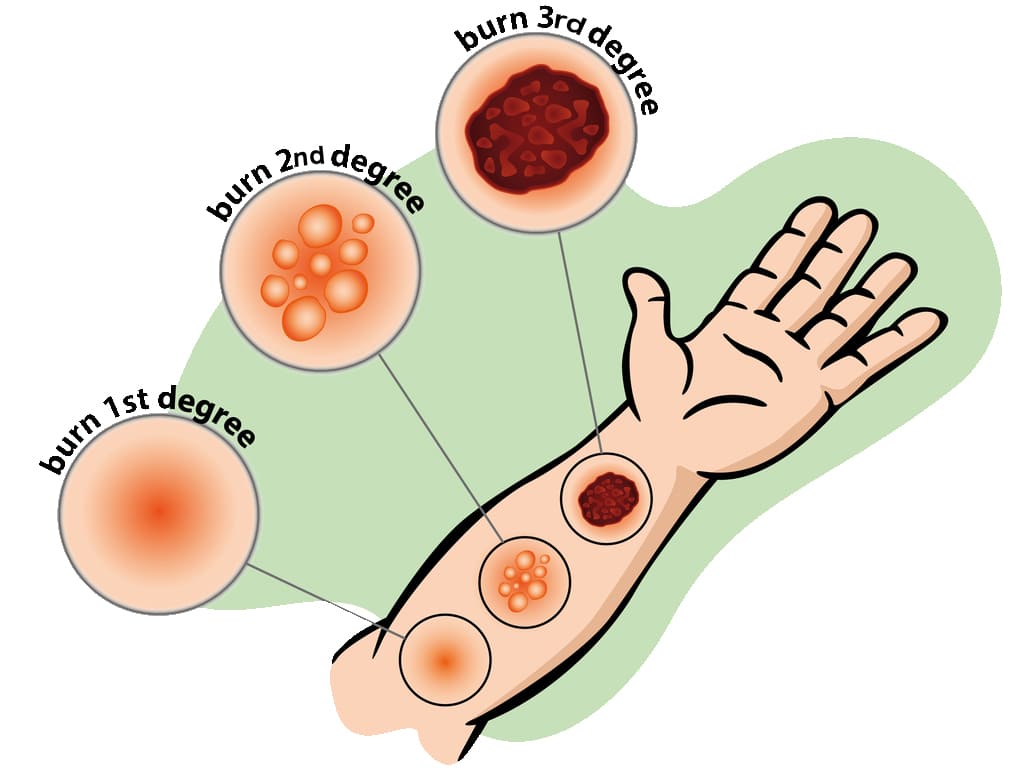
In the past, burns were defined by degrees; first degree, second degree and third degree burns. They now advocate more explicit definition categorizing the burn according to the depth of skin destruction.
- SUPERFICIAL BURNS: Involves only the outer most skin layer. They have redness, swelling, and tenderness. It usually heals well, if first aid is given promptly and if blisters don’t form. Burns from sun, charcoal stove. Are also known as first degree burns.
- PARTIAL THICKNESS BURNS: The damage to epidermis is severe, we almost always have blister formation and very painful. Completely destroys the epidermis. Blisters form because of fluid released from the damaged tissue, usually heal well but may be fatal if more than 30% of skin is involved. Also known as second degree burns.
- FULL THICKNESS/DEEP BURNS: The dermis is involved including other structures like muscles, bones. All layers involved blood vessels, fat and nerves. There is either no pain or minimal. This may mislead that the burns are not severe. You need immediate help; the skin is pale and charred (like toasted meat).
LOCATION OF BURN
- The location of the burn wound is related to the severity of the burn injury. Burns to the face and neck and circumferential burns of the chest may inhibit respiratory function by virtue of mechanical obstruction secondary to edema or scar formation.
- These injuries may also indicate the possibility of inhalation injury and respiratory mucosal damage.
- Burns of the hands, feet, joints, and eyes are of concern because they make self-care very difficult and may jeopardize future function.
- The ears and nose, composed mainly of cartilage, are susceptible to infection because of poor blood supply to the cartilage.
- Burns of buttocks and genitalia are highly susceptible to infection.
- Circumferential burns of the extremities can cause circulatory compromise distal to the burn with subsequent neurologic impairment of the affected extremity.
- Patient may develop compartment syndrome from direct heat damage to the muscles, multiple intravenous access attempts or pre burn vascular problems.
EXTENT OF A BURNT AREA.
Two commonly used guides for determining the total body surface area (TBSA) affected or the extent of a burn wound are the Lund-Browder chart and rule of nines. Only partial thickness burns and full thickness burns are included when calculating the burnt area because it is more accurate. The patient’s age, in proportions to relative body area size, is taken into account. For irregular or odd-shaped burns, the palmar surface of the patient’s hand is considered to be approximately 1% of the TBSA.
USES OF WALLACE’S RULE OF 9 (for Adults)
- Head and neck is 9% (NB. The head alone is 8% and the neck is 1%).
- Each arm is 9% (both arms carry 18%).
- Anterior trunk-18% (chest and abdomen).
- Posterior trunk-18% (from neck to symphysis, coccyx).
- Each lower limb-18% (both limbs 36%).
- Perineal/genital area-1%.
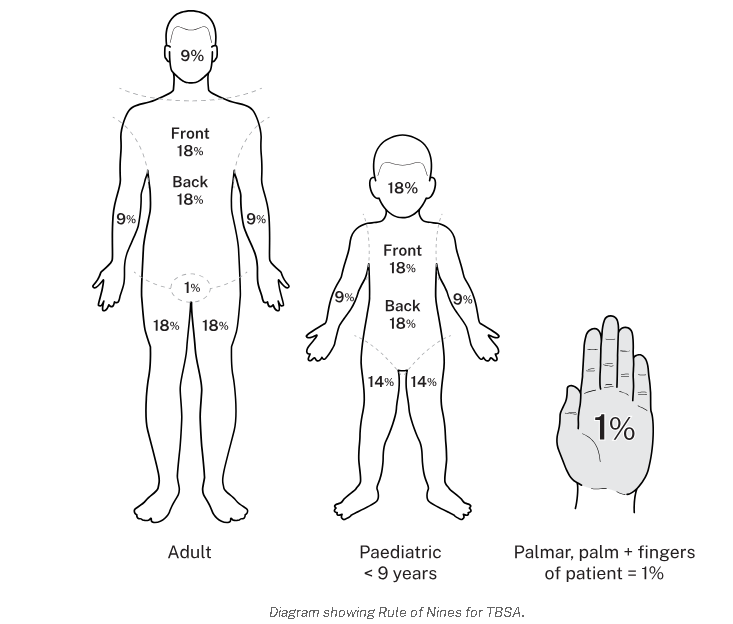
WALLACE’S RULE IN CHILDREN (slight difference)
- Head -18%
- Arms -9%
- Chest and trunk -18%
- Back of trunk -18%
- Legs -14%
- Perineal and genital area -1%
Use of Lund Browder’s chart
| Head | 7% |
| Neck | 2% |
| Anterior trunk | 13% |
| Posterior trunk | 13% |
| Rt buttock | 2.5% |
| Lt buttock | 2.5% |
| Genitalia | 1% |
| Rt upper arm | 4% |
| Lt upper arm | 4% |
| Rt lower arm | 3% |
| Lt lower arm | 3% |
| Rt hand | 2.5% |
| Lt hand | 2.5% |
| Rt thigh | 9.5% |
| Lt thigh | 9.5% |
| Rt leg | 7% |
| Lt leg | 7% |
| Rt foot | 3.5% |
| Lt foot | 3.5% |
| Total | 100% |
PREDISPOSING FACTORS & ASSESSMENT
PREDISPOSING FACTORS
- Age, children and old (weak)
- Disease-commonly epilepsy, leprosy
- alcoholism, and cigarette smoking
- Occupation-e.g. electricians, industrial workers, alcohol brewers
- Poverty e.g crowded kitchen.
- Fights (wrangles and conflicts)
- Race e.g. frost bite common in whites
- Skin bleaching.
SIGNS AND SYMPTOMS OF BURNS
- History of involvement with any of the cause of burns.
- Blistering due to vasodilation hence collection of serum between the dermis and epidermis.
- Necrosis due to coagulation of proteins.
- Functional impairment of the temperature regulation process of the burnt area.
- Shock due to fluid loss and blood loss (hypovoleamic shock).
- Shock can also occur due to severe pain (neurogenic shock).
- Toxaemia depending on the type and cause of burns. Histamines and adenocytes produced are released from the burnt surface and they find their way into the blood stream.
ASSESSMENT OF BURNS
- Circumstances and cause of burns i.e. where and when did it occur.
- Was the airway affected? Assess whether it was in closed spaces (inhaled hot gases).
- Assess the extent, location and depth. The bigger the burn, the higher the extent (%) the greater the surface area.
CRITERIA FOR ADMISSION OF BURNT PATIENT.
- Burns involving the airways
- Full thickness.
- Admit all children for observation
- The bigger the surface area above 5% superficial burns.
- Special areas involved e.g. face, hands, joints, neck, and genitalia.
- Circumferential burns give a tourniquet effect may cause gangrene.
- Electric burns because all electric burns are said to be deep until proved otherwise.
- Chemical burns, can continue burning for several days.
- If you are not sure; below 15% burns, GIT absorption is intact, oral route work in fluid replacement.
FIRST AID FOR BURNS.
AIMS
- Maintain an open airway.
- Minimize the risk of infection
- Treat any other associated injuries
- Make sure you watch for signs of shock.
- Make sure you check for signs of respiratory distress.
ACHIEVING THE FIRST AID MANAGEMENT
- Decrease temperature /stop fire if possible.
- Call for help.
- Evacuate the patient; pour water on the affected area.
- Undress the patient.
- Assume the airway has been affected until proved otherwise continue pouring water on the burnt area for minimally 20min to reduce injury i.e neutralized heat.
- Lie patient down but avoid the burnt area touching the ground.
- Pour water on burns for 20mins.
- Continue pouring water until pain stops.
- Put on gloves.
- Remove rings, shoes, watches, necklace, belts, stockings and clothes before tissue damage.
- Cover the injured area with sterile cloth or sterile dressing.
- Record details of injuries.
- Regularly monitor and record the vital signs and the level of consciousness, urine output.
- Treat shock if present.
- Re-assure and give words of hope.
- Avoid over cooling the patients especially children and elderly because they may get hypothermia.
- Do not remove anything stuck on the burnt wound to prevent spread of infections and more injuries.
- Do not touch the burnt area with your fingers.
- Do not apply lotions on the burn apart from anti-septic.
- Do not burst any blisters.
- If burns are on the face do not cover them for easy assessment of respiratory distress.
FOR AIRWAY BURNS
Burns of the face, mouth, throat, nose, airway passages, are serious because the airway passage rapidly becomes swollen because of inflammation.
How to assess for airway burns.
- History taking.
- Respiratory rate increased.
- Examine the nostrils i.e there is no soot.
- Examine the nasal hair i.e if they are burnt, short with a Taft.
- There would be damaged to the skin around the nose and mouth.
- Has difficulty in breathing.
- Has hoarse voice due to inflammation of vocal cords.
AIMS OF MANAGEMENT
- To recognize the airway burns.
- To maintain the airway and after take the patient to hospital management.
First Aid Management for Airway Burns
- Open the mouth (airway) and check whether he is breathing.
- Sweep the tongue.
- If not breathing, give rescue breaths, mouth to mouth. Put patient in a recovery position and call for help.
- Take the steps to improve the airway e.g remove clothes or unbutton, clear the place.
- Re assure the patient.
- Monitor and record vital observations until help arrives.
Interventions in the hospital
Put patient on oxygen therapy. Intubate the patient with endotracheal tube, connected to oxygen cylinder.
FOR CHEMICAL BURNS
The commonest cause of chemical burns in Uganda are domestic fights and it’s commonly women to women.
FIRST AID
- Ensure your safety.
- Disperse the powerful chemical by wiping away the chemical, pouring water (plenty) for about 30min. This dilutes the chemical.
- Arrange to transfer patient to hospital but label the chemical if you have identified it.
- Do not attempt to neutralize the chemical with another chemical.
- Ensure that you remove contaminated clothing.
- If the face has been burnt, expect the burns of the airway. Make sure that the airway is open and functioning.
How do you recognize chemical burns
- There may be chemicals in the vicinity.
- The pain is intense and stinging (itching).
- Later discoloration, blistering and peeling of the skin forming wound.
- Supportive treatment with anti-inflammatory drugs, anxiolytics, painkillers.
- Re-assure the patient.
FOR ELECTRIC BURNS
These occur when electricity passes through the body, person a conductor through which electricity passes. Most of the visible damage occurs at points of entry and exit of the current. You may have an internal tract where wounds are mainly concentrated. The current follows mainly muscle, nerves and blood vessels. If it follows the nerves, it can cause cardiac arrest which is the commonest cause of death in electric burns.
NOTE:
The current will cause muscle spasms which may prevent patient from breaking contact with electric source hence continues electric shock. Switch off the main switch. Do not touch a patient with live hands or metallic materials to break the contact. Assess the ABC immediately. Shout for help. Be safe, do something and waste no time.
FIRST AID {AIMS}
- Ensure your safety first.
- Ensure that electric source is disconnected or blocked i.e you may use your shoes or clothes to disconnect the source from patient.
- Flood the exit and entry points with water to cool the burn and prevent further burning process.
- Protect the burn from infection.
- Re-assure
- Give treatment for shock.
ASSESSMENT FOR BURNS TO THE EYE.
Patient is usually unconscious or semi-conscious. If eyes are burnt with chemicals, it will cause scarring and blindness so gets water and wash the eyes to dilute and disperse the acid. Let them not rub the eyes (don’t touch the eyes), continue pouring water in the eyes.
SIGNS AND SYMPTOMS OF EYE BURNS.
- Continue watering the eyes
- Swollen
- redness
Treatment
- Have gloves on.
- Lie the patient with the affected eye low and most so that water does not affect the rest of the face.
- Open that eye and run cold water for more than 30 minutes.
- Make sure that the water is penetrating into all parts of the eye. Open eye with your hands if they cannot open.
- Get a clean bandage and close the eye until the opthalmist comes.
- Try to identify the chemical and record or label.
GENERAL MANAGEMENT OF BURNS
Aims of management
- To arrest bleeding.
- To prevent the condition from worsening.
- To preserve life.
- To correct electrolyte imbalances. Etc
N.B Burns with a TBSA greater than 15% the following is done. It is a surgical emergency so quit assessment and immediate care is needed plus quick admission. (Immediate nursing care).
Airway maintenance
Through opening and clearing the airway, In case of a suspected cervical spine, keep movements of the neck to a minimum and never hyperflexion or hyperextend to head or neck. If smoke inhalation is suspected intubate before oedema makes it difficult. The head of the bed is elevated and nasal pharynx suction is done incase of excessive secretions.
Breathing and ventilation.
Expose the chest and make sure that chest expansion is adequate. Always provide oxygen in severe burns or when inhalation injury is suspected give 4-8 hr/min. Assess breathing sounds and respiratory rate. Monitor for hypoxia. Encourage aggressive pulmonary care e.g. turning, coughing and deep breathing.
Circulation and hemorrhage control
Stop bleeding with direct pressure. Check capillary if greater than 2secs it means hypovolaemia. Monitor pulse and check pallor which occurs with 30%. Insert 2 large bore peripheral IV lines in superficial burns.
Assessment of the neurological status.
This is done through using a glasgowcoma scale. This helps to check the levels of consciousness that is checking;
- Alertness (A)
- Response to vocal stimuli (V)
- Response to painful stimuli (U)
- Unresponsive.
Examine the pupils for light reaction. Hypoxia can cause reduced levels of response. Keep the patient flat and covered with a sterile sheet to relieve the pain induced by circulatory air currents. Keep the patient warm and check for any adherent clothing, cut around it, when removing the cloth i.e cut around the edges of the clothes disturbing the wound as little as possible.
GENERAL NURSING CARE OF A BURN PATIENT
Maintenance of an aseptic environment.
All attendants must wear capes, gowns, masks and cover shoes. Hands should be washed thoroughly. Cleaning should consist of sloughing skin and use of aseptic solution like hibitane or savlon, the surface is then dried with warm air or sterile dressing (gauze). Afterwards the burnt area is treated by either the exposure method or closed of dressing.
Management of wounds.
- Nurse the patient in a special room to prevent infections (burns are normally sterile). Make sure that you maintain asepsis as much as possible.
- Avoid touching the wound with bear hands i.e. use sterile gloves and use a disinfectant after attending to the patient.
- You must have a mask while examining the patient.
- Use the mosquito net to protect the patient from flies.
- Limit visitors as these increase the risk of infection we give definitive treatment (dress) after resuscitation for burns involving the eyes attend to airway then the burnt eyes and resuscitation later.
FLUID REPLACEMENT
Always replace the lost fluids, can be IV or orally since fluid absorption in the GIT is now very poor. IV fluids are recommended. If an adult loses 15% of the body fluid or as little as 10% in a small child, this will lead to shock. Replacement needs to be continued for at least 48hours.
In deep burns, plasma is given as this is what the patient is losing in 48hours. Towards the end of 48hours, whole blood is given to replace RBCs destroyed, later N/S to replace electrolytes. Glucose to replace energy loss.
Fluid Replacement Calculation (Parkland Formula basis)
The volume of fluid replacement (Y) = (weight in kg X surface area of burns) mls / 2. This volume is given over 8 hours.
Example: Y = (70kg X 20%) / 2 = 700mls. Y=700mls in 4 hours so multiply it by 2 = 1400mls in first 8hours.
- Y=1400mls in the next 16hours
- Y=1400mls in the next 24hours
But adults require 3 liters in 24hours with or without burns (normal physiological fluid requirement). How much is needed Z = (3000x1)/24 = 125mls per hour.
The rate of fluid loss in children below 6yrs is twice that of adults hence double the fluids to be replaced.
Management of Wounds
- Nurse the patient in a special room to prevent infections (burns are normally sterile).
- Avoid touching the wound with bear hands i.e. use sterile gloves and use a disinfectant after attending to the patient.
- You must have a mask while examining the patient.
- Use the mosquito net to protect the patient from flies.
- Limit visitors as these increase the risk of infection.
EXPOSED METHOD
Nothing touches the burn except air and anti-bacterial agent e.g. hibitane, ghee and honey. This indicates for burns of the face especially scalds. It is good for areas that are difficult to dress e.g. perineum, buttocks, face, Axilla.
OCCLUSIVE / CLOSED METHOD.
This method keeps the wound sterile, also aims at applying anti-bacterial agents. E.g. ghee, honey, neomycin cream, tetracycline, hibitane etc.
PROCEDURE FOR BURN DRESSING APPLICATION
This procedure emphasizes a "no-touch" sterile technique to prevent infection.
- Ensure Sterility: Utilize a number touch technique, meaning no human hand shall directly touch the burn or the dressing materials, except when sterile. All instruments used must be sterile.
- Consider Sedation: Administer appropriate sedation if required, to ensure patient comfort and cooperation during the procedure.
- Clean the Area: Gently clean the burn wound and the surrounding healthy skin with Chlorhexidine solution.
- Manage Blisters: Leave any blisters intact; do not puncture them, as they provide a natural protective barrier against infection.
- Apply Impregnated Gauze: Using a sterile spatula, carefully apply the impregnated gauze directly onto the burn wound.
- Apply Dry Gauze: Cover the impregnated gauze with at least 2cm of dry gauze.
- Add Cotton Wool: Place approximately 3cm of cotton wool over the dry gauze layer.
- Secure with Crepe Bandage: Apply a crepe bandage to secure all layers of the dressing.
- Extend Dressing Margins: Ensure the entire dressing extends beyond the wound margin by about 10cm to provide adequate coverage and protection.
Prevention of Burns
- Treat the epileptics, teach them, and mobilize the community about epileptics with burns.
- Raised fire places.
- Keep flues out of the houses e.g. petrol.
- Keep chemical in raised places and out of reach of children.
- Avoid bleaching.
- Keep children out of hot or fire places.
COMPLICATIONS OF BURNS
- Shock.
- Excessive oedema, quite dangerous if burns are of the face, neck as it causes obstruction of the airway and oesophagus.
- Renal failure; due to failure to give adequately fluids.
- Toxaemia and infections; infection of the burnt area causing sepsis resulting in septicaemia, gas gangrene and tetanus.
- Depression of the bone marrow.
- Contractures.
- Keloid formation
- Electrolyte imbalance
- Anaemia due to haemolysis.
- Thrombosis due to plasma loss.
- GIT bleeding, ulcers develop due to increased production of gastric acid.
- Paralytic ileus.
- Sepsis.
- Neuromas
- Cosmetic disfigurement
- Mal-function of the body part
BURNS LECTURE NOTES Read More »
Surgical Shock
COMMON SURGICAL CONDITIONS
SHOCK
Definition
- Shock is a state of poor perfusion with impaired cellular metabolism manifesting with severe pathophysiological abnormalities. It is due to circulatory collapse and tissue hypoxia. Shock is meant by ‘inadequate perfusion` to maintain normal organ function.
- The condition associated with circulatory collapse when the arterial blood pressure is too low to maintain an adequate supply of blood to the tissues.
- The failure of the circulatory system to adequately supply oxygen to the tissues.
Shock is a life-threatening medical condition characterized by inadequate tissue perfusion and oxygenation, leading to cellular dysfunction, widespread organ damage, and if uncorrected, irreversible organ failure and death. It's not simply low blood pressure, but rather a critical imbalance between the demand for oxygen and nutrients by the cells and the body's ability to deliver them.
ETIOLOGY AND PATHOPHYSIOLOGY
Shock has a multitude of causes. The most common cause of shock is severe blood loss i.e. if it exceeds 1.2 liters.
The circulation may fail because of the following:
Sudden malfunction of the heart. This may occur as a result of:- Coronary arterial occlusion with acute myocardial ischaemia.
- Trauma with structure damage to the heart
- Toxaemia – bacterial or viral
- Effects of drugs
- Postoperative atelectasis and pneumonia
- Thoracic injuries, particularly tension pneumothorax, bruising and laceration of the lungs
- Obstruction of the pulmonary artery by an embolus.
- Disturbances of lung function following surgery and anesthesia.
- Whole blood – haemorrhage
- Plasma – significant in burns
- Water and electrolyte which occurs in: Peritonitis, Intestinal obstruction and paralytic ileus, Severe diarrhoea and vomiting.
- Adrenal deficiency
- The common faint. The arterioles in the muscle relax
- Over dosage of drugs eg analgesic like pethedine
- Following therapy with beta blocking agents for angina, hypertension etc
- Noxious stimuli, such as pain, if severe with cause vasodilation
- Systolic dysfunction: it is the inability of the heart to pump forward like in myocardial infarction and cardial myopathy
- Diastolic dysfunction: it is the inability of the heart to fill e.g. cardiac tamponade, ventricular hypertrophy and cardial myopathy
- Dysrhythmias eg in bradyrhythmias and tarchyrhythmias
- Structural factors like valvular stenosis or regurgitation, ventricular septal rapture
- Internal bleeding like fracture of long bones, ruptured spleen heamopneumothorax and severe pancreatitis
- Fluid shift like in burns and cysts
- Spinal anesthesia
- Vasomotor center depression
Types, and Clinical Manifestations
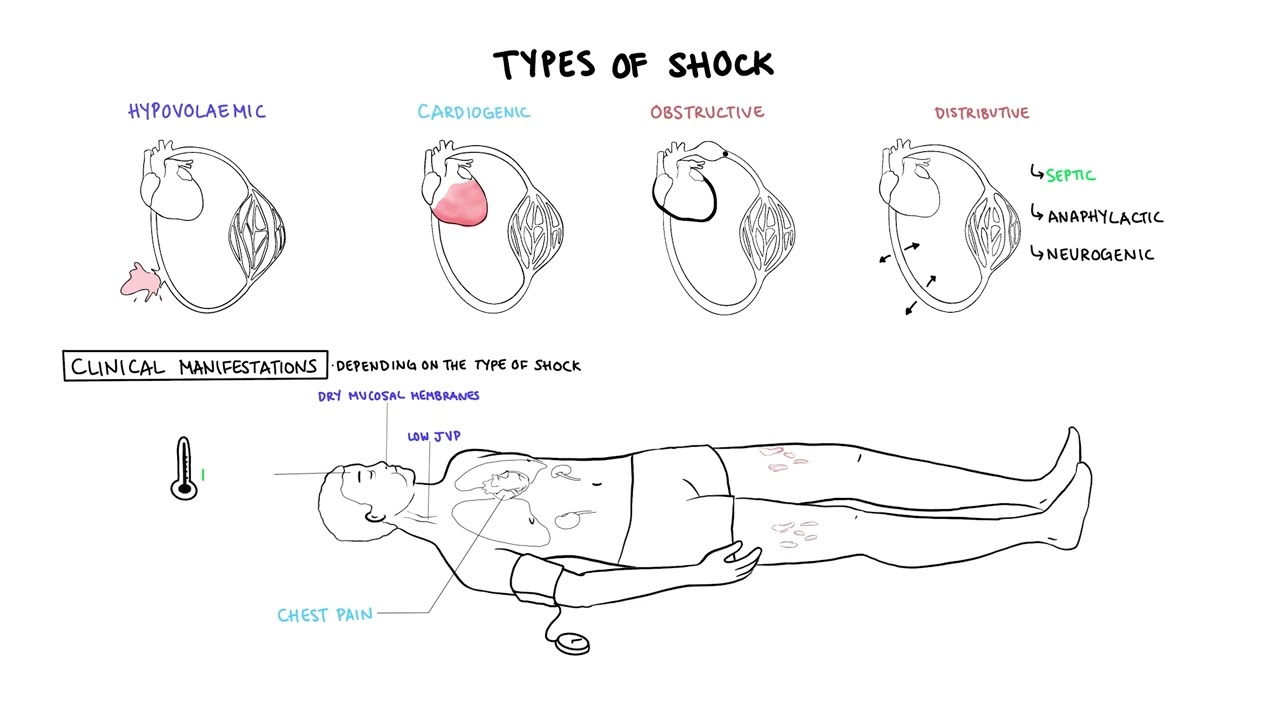
Types of Shock: Categorization by Underlying Pathophysiology
Shock is broadly classified into several types based on the primary physiological mechanism causing the inadequate tissue perfusion. While these types have distinct primary causes, they often share common clinical features and can coexist or lead to one another.
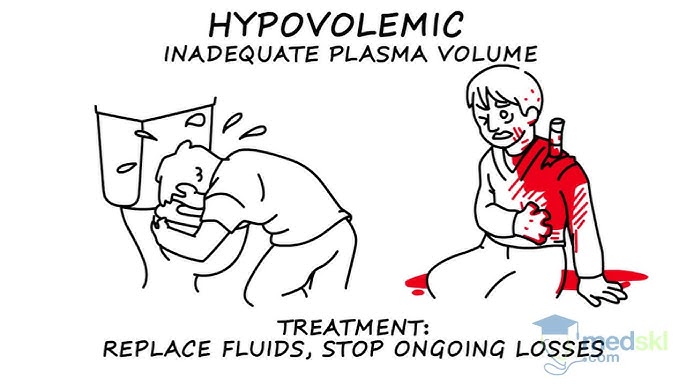
1. Hypovolemic Shock (Inadequate Circulating Volume)
- Trauma (external or internal bleeding)
- Gastrointestinal bleeding (e.g., peptic ulcer, variceal bleeding)
- Post-surgical bleeding
- Obstetric hemorrhage (e.g., postpartum hemorrhage)
- Aortic rupture
- Severe Dehydration: Vomiting, diarrhea, inadequate fluid intake.
- Severe Burns: Massive fluid shifts from intravascular space into interstitial space.
- Peritonitis/Bowel Obstruction: Fluid sequestration within the abdominal cavity or bowel lumen.
- Diabetic Ketoacidosis (DKA) / Hyperosmolar Hyperglycemic State (HHS): Profound osmotic diuresis.
- Excessive Diuretic Use.
2. Cardiogenic Shock (Pump Failure)
- Myocardial Infarction (MI): Especially extensive anterior or left ventricular MI, which damages a significant portion of the heart muscle.
- Severe Arrhythmias: Tachyarrhythmias (e.g., ventricular tachycardia, atrial fibrillation with rapid ventricular response) or bradyarrhythmias that significantly reduce ventricular filling time or heart rate.
- Valvular Heart Disease: Acute severe mitral regurgitation, aortic stenosis.
- Cardiomyopathies: Acute exacerbation of chronic heart failure.
- Myocarditis: Inflammation of the heart muscle.
- Acute Papillary Muscle Rupture.
3. Distributive Shock (Vasogenic Shock / Abnormal Vasodilation)
a. Septic Shock:
- Definition: A life-threatening organ dysfunction caused by a dysregulated host response to infection, leading to persistent hypotension requiring vasopressors to maintain mean arterial pressure (MAP) ≥ 65 mmHg and having a serum lactate level > 2 mmol/L despite adequate fluid resuscitation.
- Pathophysiology: Triggered by severe infection (bacterial, viral, fungal). Pathogen-associated molecular patterns (PAMPs) and danger-associated molecular patterns (DAMPs) released from pathogens and damaged host cells activate a complex inflammatory cascade. This leads to widespread endothelial dysfunction, microcirculatory alterations, profound vasodilation, increased capillary permeability (fluid leakage into interstitial spaces leading to relative hypovolemia and edema), and myocardial depression.
- Causes: Severe infections, particularly with Gram-negative bacteria (e.g., *E. coli, Klebsiella, Pseudomonas*) or Gram-positive bacteria (e.g., *Staphylococcus aureus, Streptococcus pneumoniae*). Common sources include pneumonia, urinary tract infections, abdominal infections (e.g., appendicitis, diverticulitis), and skin/soft tissue infections.
- Clinical Features: Often presents as "warm shock" in early stages (warm, flushed skin, bounding pulses) due to vasodilation, progressing to "cold shock" as compensatory mechanisms fail and cardiac output falls.
- Definition: A severe, life-threatening systemic allergic reaction characterized by rapid onset of profound vasodilation, increased vascular permeability, and bronchoconstriction.
- Pathophysiology: Exposure to an allergen triggers a massive release of inflammatory mediators (e.g., histamine, leukotrienes, prostaglandins) from mast cells and basophils. These mediators cause widespread vasodilation and leakage of fluid from capillaries into the interstitial space, leading to circulatory collapse and airway obstruction.
- Causes: Exposure to allergens such as insect stings, certain foods (e.g., peanuts, shellfish), medications (e.g., antibiotics, NSAIDs), or latex.
- Definition: Occurs due to loss of sympathetic nervous system tone, leading to widespread vasodilation and pooling of blood in the periphery. Unlike other forms of shock, the heart rate may be paradoxically normal or even bradycardic.
- Pathophysiology: Damage to the sympathetic nervous system (typically above T6) interrupts the normal vasoconstrictive impulses to peripheral blood vessels. This results in unopposed parasympathetic activity, leading to profound vasodilation and often bradycardia.
- Causes:
- Spinal cord injury (most common cause).
- Spinal anesthesia.
- Guillain-Barré Syndrome.
- Severe head trauma (less common as a primary cause).
- Certain drugs (e.g., ganglionic blockers, adrenergic antagonists).
- Definition: Shock resulting from acute hormonal deficiencies that disrupt normal cardiovascular function and metabolic processes.
- Causes: Adrenal crisis (acute adrenal insufficiency leading to severe hypotension refractory to fluids and vasopressors due to lack of cortisol) or myxedema coma (severe hypothyroidism leading to decreased cardiac output, bradycardia, and hypothermia).
4. Obstructive Shock (Extracardiac Obstruction to Blood Flow)
- Pulmonary Embolism (PE): Massive PE obstructs blood flow from the right ventricle into the pulmonary circulation.
- Cardiac Tamponade: Accumulation of fluid or blood in the pericardial sac, compressing the heart and preventing adequate ventricular filling.
- Tension Pneumothorax: Air accumulation in the pleural space collapses the lung and shifts the mediastinum, compressing the great vessels and heart.
- Constrictive Pericarditis (severe acute exacerbation).
- Critical Valvular Stenosis (less common as primary obstructive shock).
5. Vasovagal Shock (Neurocardiogenic Syncope)
- Definition: While often presenting as syncope (fainting), severe forms can lead to a transient state of shock. It's characterized by a sudden, exaggerated reflex response that results in both widespread peripheral vasodilation and bradycardia.
- Pathophysiology: Triggered by certain stimuli (e.g., pain, fear, emotional stress, prolonged standing, specific odors). The vagus nerve is overstimulated, leading to parasympathetic activation (bradycardia) and sympathetic inhibition (vasodilation), causing a temporary drop in blood pressure and cerebral perfusion.
- Clinical Significance: Usually self-limiting and resolves upon lying down. Rarely life-threatening unless associated with significant trauma from a fall. Not considered a true "shock state" in the critical care sense as it's typically transient and reversible with simple measures.
Recognition Features of Shock / Signs and Symptoms of Shock
The signs and symptoms of shock are a reflection of the body's compensatory mechanisms attempting to maintain vital organ perfusion, followed by the failure of these mechanisms as shock progresses. The specific presentation can vary slightly depending on the type and stage of shock.
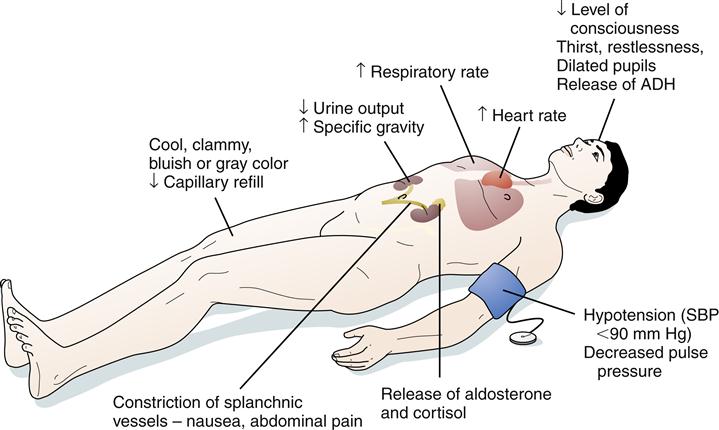
I. Early / Compensatory Stage (Body's attempt to maintain vital organ perfusion)
In this initial stage, the body activates its sympathetic nervous system and hormonal responses to maintain blood pressure and vital organ blood flow. This often leads to increased heart rate and vasoconstriction.
Cardiovascular:- Rapid Pulse (Tachycardia): The earliest and most consistent sign. The heart beats faster to compensate for reduced cardiac output.
- Normal to Slightly Decreased Blood Pressure: The body is still able to maintain BP through vasoconstriction.
- Pale, Cool, Clammy Skin: Due to peripheral vasoconstriction shunting blood away from the skin to vital organs. The clamminess is due to diaphoresis (sweating) caused by sympathetic stimulation.
- Delayed Capillary Refill: >2 seconds (indicates poor peripheral perfusion).
- Restlessness, Anxiety, Agitation: Early signs of cerebral hypoperfusion and catecholamine release.
- Increased Thirst: Due to fluid shifts and activation of the renin-angiotensin-aldosterone system.
- Oliguria: Decreased urine output (< 0.5 mL/kg/hr) as kidneys conserve fluid and blood flow is shunted away.
- Slightly Increased Respiratory Rate: Due to metabolic acidosis (from anaerobic metabolism) and increased oxygen demand.
II. Progressive / Decompensatory Stage (Compensatory mechanisms begin to fail)
As shock progresses, the compensatory mechanisms become overwhelmed, leading to widespread cellular hypoxia, anaerobic metabolism, and accumulation of lactic acid. Organ function begins to deteriorate.
Cardiovascular:- Hypotension: Significant drop in systolic blood pressure (<90 mmHg or MAP <65 mmHg) or a drop of >40 mmHg from baseline. This is a critical sign that compensation has failed.
- Weak, Thready Pulse: Rapid but difficult to palpate, indicating profound vasoconstriction and low stroke volume.
- Progressively Colder, Mottled Skin: Especially in extremities (e.g., "grey-blue skin," cyanosis of lips and nail beds) due to severe peripheral vasoconstriction and pooling of deoxygenated blood.
- Lethargy, Drowsiness, Confusion: Worsening cerebral hypoperfusion.
- Decreased Responsiveness to Stimuli.
- Nausea, Vomiting: Due to reduced blood flow to the GI tract.
- Abdominal Pain.
- Rapid, Shallow Breathing (Tachypnea): The body's attempt to compensate for metabolic acidosis.
- Increasing Lactic Acidosis: Due to anaerobic metabolism.
III. Irreversible / Refractory Stage (Widespread cellular and organ damage)
In this final stage, cellular and organ damage becomes so severe that it is irreversible, even with aggressive interventions. Multi-organ dysfunction syndrome (MODS) develops, leading inevitably to death.
Cardiovascular:- Profound Hypotension: Unresponsive to fluids and vasopressors.
- Severe Tachycardia or Bradycardia: With eventual cardiac arrest.
- Absent Peripheral Pulses.
- Unconsciousness, Coma.
- Fixed, Dilated Pupils.
- Loss of Reflexes.
- Gasping for Air (Agonal Respirations): Severe respiratory distress.
- Respiratory Failure.
- Anuria: Complete cessation of urine production.
- Acute Kidney Injury.
- Severe Lactic Acidosis: Uncorrectable.
- Electrolyte Imbalances.
- Disseminated Intravascular Coagulation (DIC): Widespread clotting and bleeding.
- Multi-Organ System Failure (MOSF).
Special Considerations: Warm Shock (Septic Shock in Early Stages)
While most forms of shock present with cool, clammy skin due to vasoconstriction, early septic shock (hyperdynamic or "warm shock" phase) can present differently due to the profound systemic vasodilation:
- Warm, Dry, Flushed Skin: Due to peripheral vasodilation.
- Rapid, Strong (Bounding) Pulse: Indicating a hyperdynamic state and decreased systemic vascular resistance.
- Fever: Evidence of underlying infection.
- Hyperventilation: To compensate for metabolic acidosis.
- Despite these initial "warm" signs, tissue perfusion is still inadequate at the microcirculatory level, and this phase rapidly progresses to decompensated ("cold") shock if not aggressively treated.
MANAGEMENT OF SHOCK
AIMS
- To treat the cause
- To improve cardiac function
- To improve tissue perfusion
Emergency treatment for shock
- Help patient to lie down and place patient in supine position
- Cover patient and keep him or her warm
- Raise and support her legs as high as possible
- Administer oxygen if possible
- Determine underlying cause and treat if possible e.g. applying pressure for bleeding.
- Lessen any tight clothing, undo anything that constrict the neck, chest and wrist
- Monitor breathing, pulse and response
- Monitor and record vital observation like pulse breathing, monitor level of response, if the casualty become unconscious, open the airway and check breathing.
General management
- Treat the cause e.g. arrest haemorrhage, drain pus etc.
- Fluid replacement e.g. plasma normal saline dextrose ringers lactate, plasma expanders maximum 1 liter can be given in 24hours.
- Blood transfusion is done whenever necessary, hypotonic solutions like dextrose are poor volume expanders and so should not be used in shock.
- Inotropic agents e.g. dopamine, dobutamine, adrenaline infusions.
- Correction of acid base balance. Acidosis is corrected by using 8.4 sodium bicarbonate intravenously.
- Steroid is often life saving. 500- 1000mg of hydrocortisone can be given. It improves perfusion, reduces the capillary leakage and systemic inflammatory effects.
- Antibiotics in patients with patients with sepsis; proper control of blood sugar and ketosis in diabetic patients.
- Catheterization to measure urine output (30 – 50mls/hour or > 0.5 ml/kg/ hour should be maintained).
- Nasal oxygen to improve oxygenation or ventilator support with intensive care unit monitoring has to be done.
- Haemodialysis (a process of removing a waste part e.g. kidney) may be necessary if kidneys are not functioning.
- Control pain using morphine (4mg iv).
- Injection ranitidine iv or omeprazole iv or pantoprazole iv.
- Activated c protein, it is beneficial as it prevents the release of inflammatory response.
- Diuretics, mannitol is an osmotic that neither absorbed in the renal tubules nor metabolized. It may be given when acidosis and Oliguria have been corrected but if oliguria persist frusemide may also be given.
- Anticoagulants may occasionally be indicated if micro- circulatory thrombosis is suspected.
Prevention of shock
Pre operative measures
- Take thorough history which include biographic data, medical history, obstetric history, gynaecological.
- Assess the level of consciousness.
- Take the baseline vital observation which include temperature, pulse, respiration and blood.
- General body assessment from head to toe to rule out abnormalities like oedema, hemorrhage, cyanosis and pallor.
- If there is external heamorrhage arrest the bleeding by positioning the patient.
- Empty the bladder by passing a catheter.
- Antibiotic prophylaxis is given to prevent sepsis.
- Take investigation such as hemoglobin estimation, cross matching, blood grouping and cross matching, clotting factor, malaria slide etc.
- Give anxiolytics to allay anxiety and give pain killer to reduce pain.
- Resuscitate patient with iv fluids.
- Reassure the patient.
- The patient should be educated about physical exercises which are done post operatively.
- Circulatory collapse should be avoided by strenuous measures if all possible.
- Preoperatively patient should be fit as possible from the point of view of the circulatory system: His blood should be a adequate in quality and volume, His tissues should be hydrated adequately, He should be mobile so that there is no stagnation in the circulatory system.
Intra operatively
- Patient is kept warm on his journey from the ward to the theater and back.
- Fear is allied and tranquiller are commonly used pre- operatively.
- The blood pressure is monitored continuously and recorded more so for the serious cases.
- Blood and fluid replacement is commenced in good time and the patient is monitored using fluid balance chart.
- Major operations are commenced only after satisfactory infusions have been established.
- The head of the bed is lowered if the blood pressure falls (Trendelenburg position).
- The anesthetist induces and maintains an adequate level of anesthesia ensuring good oxygenation and tissue perfusion.
Post operatively measures
- Fluid and electrolyte replacement (saline, 5% dextrose, Hartman solution, plasma and blood as indicated).
- Position the patient in a recovery position.
- Maintain air way patent.
- Give antibiotics to prevent infections.
- Give inflammatory drugs.
- Check the conscious level of the patient.
- Initiate exercise like coughing, deep breathing and ambulation to aid normal circulation.
- Rest and relieve of pain are continued to prevent shock.
General Nursing Considerations and Principles for Patients in Shock
Nursing care for a patient in shock is complex, dynamic, and requires rapid assessment, intervention, and continuous monitoring. The primary goals are to optimize tissue perfusion, restore hemodynamic stability, identify and treat the underlying cause, and prevent complications. Nurses work collaboratively with the medical team to implement a comprehensive plan of care.
Nursing Diagnoses)
Nursing diagnoses guide the individualized care plan for patients. Examples for a patient in shock might include:
- Decreased Cardiac Output related to altered preload, afterload, contractility, or heart rate, as evidenced by hypotension, tachycardia, altered mental status, decreased urine output, and cool, clammy skin.
- Ineffective Tissue Perfusion (Cardiac, Cerebral, Renal, Gastrointestinal, Peripheral) related to hypovolemia, impaired cardiac pump function, maldistribution of blood flow, or obstruction, as evidenced by pallor, cyanosis, delayed capillary refill, weak peripheral pulses, altered mental status, oliguria, and increased serum lactate.
- Impaired Gas Exchange related to ventilation/perfusion mismatch, increased metabolic demand, or pulmonary edema, as evidenced by tachypnea, dyspnea, abnormal blood gas values, and cyanosis.
- Deficient Fluid Volume related to active fluid loss, failure of regulatory mechanisms, or third-space fluid shift, as evidenced by hypotension, tachycardia, decreased urine output, and dry mucous membranes.
- Risk for Infection related to invasive procedures, compromised immune status, or presence of underlying infection.
- Acute Confusion related to decreased cerebral perfusion, metabolic imbalances, or hypoxia, as evidenced by disorientation, agitation, or altered level of consciousness.
- Risk for Imbalanced Body Temperature related to altered metabolic rate, infection, or environmental factors.
- Anxiety/Fear related to critical illness, threat of death, or unpredictable prognosis.
Nursing Interventions (General Principles - specific actions depend on the type of shock)
Interventions are aimed at supporting vital organ function, addressing the underlying cause, and minimizing further deterioration. These often fall into categories of hemodynamic support, respiratory support, infection control, and monitoring.
1. Optimize Hemodynamic Status and Perfusion:
- Fluid Resuscitation: Administer intravenous fluids (crystalloids or colloids) as prescribed and monitor response (e.g., blood pressure, heart rate, urine output, central venous pressure).
- Vasopressors/Inotropes: Administer vasoactive medications (e.g., norepinephrine, dopamine, dobutamine) as prescribed to improve blood pressure and cardiac output, titrating carefully to desired effect and continuously monitoring for adverse effects (e.g., arrhythmias, tissue ischemia).
- Blood Product Administration: Administer blood transfusions (e.g., packed red blood cells, plasma, platelets) for hemorrhagic shock as indicated.
- Positioning: Position the patient to optimize cardiac output and venous return (e.g., modified Trendelenburg for hypovolemic shock if tolerated and not contraindicated).
- Maintain Body Temperature: Prevent hypothermia, which can worsen acidosis and coagulopathy. Use warming blankets if necessary.
2. Support Respiratory Function and Oxygenation:
- Oxygen Therapy: Administer high-flow oxygen via appropriate device (e.g., non-rebreather mask).
- Airway Management: Assess and maintain a patent airway. Prepare for and assist with intubation and mechanical ventilation if respiratory failure is imminent or present.
- Ventilator Management: Monitor ventilator settings, ensure proper oxygenation and ventilation, and prevent ventilator-associated complications.
- Arterial Blood Gas (ABG) Monitoring: Frequently assess ABG results to monitor oxygenation, ventilation, and acid-base balance.
3. Monitor and Assess Continuously:
- Vital Signs: Monitor heart rate, blood pressure (preferably arterial line), respiratory rate, and oxygen saturation continuously and frequently.
- Cardiac Monitoring: Continuous ECG monitoring for arrhythmias and signs of ischemia.
- Neurological Status: Assess level of consciousness, pupillary response, and motor function frequently to detect changes in cerebral perfusion.
- Urine Output: Insert an indwelling urinary catheter and monitor hourly urine output as a sensitive indicator of renal perfusion and overall hemodynamic status.
- Skin Assessment: Monitor skin color, temperature, turgor, and capillary refill for changes in perfusion.
- Laboratory Values: Monitor serial laboratory tests (e.g., CBC, electrolytes, lactate, renal and liver function tests, coagulation studies) to track response to treatment and detect complications.
- Fluid Balance: Accurately track all intake and output.
- Pain Assessment: Administer analgesia as needed, considering its effects on hemodynamics.
4. Identify and Treat the Underlying Cause:
- Administer broad-spectrum antibiotics promptly after obtaining cultures.
- Identify and control the source of infection (e.g., drainage of abscess, removal of infected line).
- Administer medications to improve cardiac contractility or reduce afterload as prescribed.
- Prepare for and assist with interventions like angioplasty, thrombolysis, or intra-aortic balloon pump (IABP) insertion.
- Identify and stop the source of bleeding or fluid loss.
- Administer fluids/blood products.
- Prepare for and assist with interventions to relieve obstruction (e.g., pericardiocentesis for tamponade, needle decompression/chest tube for tension pneumothorax).
5. Prevent Complications:
- Infection Control: Maintain strict aseptic technique for all invasive procedures (e.g., IV line insertion, Foley catheter care, wound care).
- Skin Integrity: Implement pressure injury prevention strategies (e.g., frequent repositioning, pressure-relieving devices) due to poor perfusion and immobility.
- Nutrition: Initiate enteral or parenteral nutrition as soon as feasible to support metabolic needs and gut integrity.
- Psychological Support: Provide emotional support to the patient and family, explain procedures, and answer questions honestly.
- Deep Vein Thrombosis (DVT) Prophylaxis: Administer prophylactic anticoagulants or use pneumatic compression devices as ordered.
6. Documentation and Communication:
- Document all assessments, interventions, and patient responses accurately and in a timely manner.
- Communicate effectively with the interdisciplinary team (physicians, respiratory therapists, pharmacists, etc.) regarding patient status, changes, and concerns.

GANGRENE
GANGRENE
Definition
Causes: Ischemia and Infection as Primary Drivers
- Thrombosis: Formation of a blood clot within a blood vessel, obstructing flow.
- Embolism: A piece of clot, fat, or other material travels and lodges in a blood vessel, blocking it.
- Atherosclerosis: Hardening and narrowing of arteries, leading to chronic reduction in blood flow, especially to the extremities.
- Vasoconstriction/Vasospasm: Severe narrowing of blood vessels (e.g., in Raynaud's phenomenon).
- External Compression: Pressure on blood vessels (e.g., from tight casts, prolonged immobility leading to pressure ulcers).
- Gas Gangrene: Caused predominantly by *Clostridium perfringens* and other anaerobic bacteria, which produce potent toxins and gas within tissues.
- Streptococcal and Staphylococcal Infections: While less common as a primary cause of widespread gangrene compared to clostridial species, severe invasive infections (e.g., necrotizing fasciitis) can rapidly lead to tissue death.
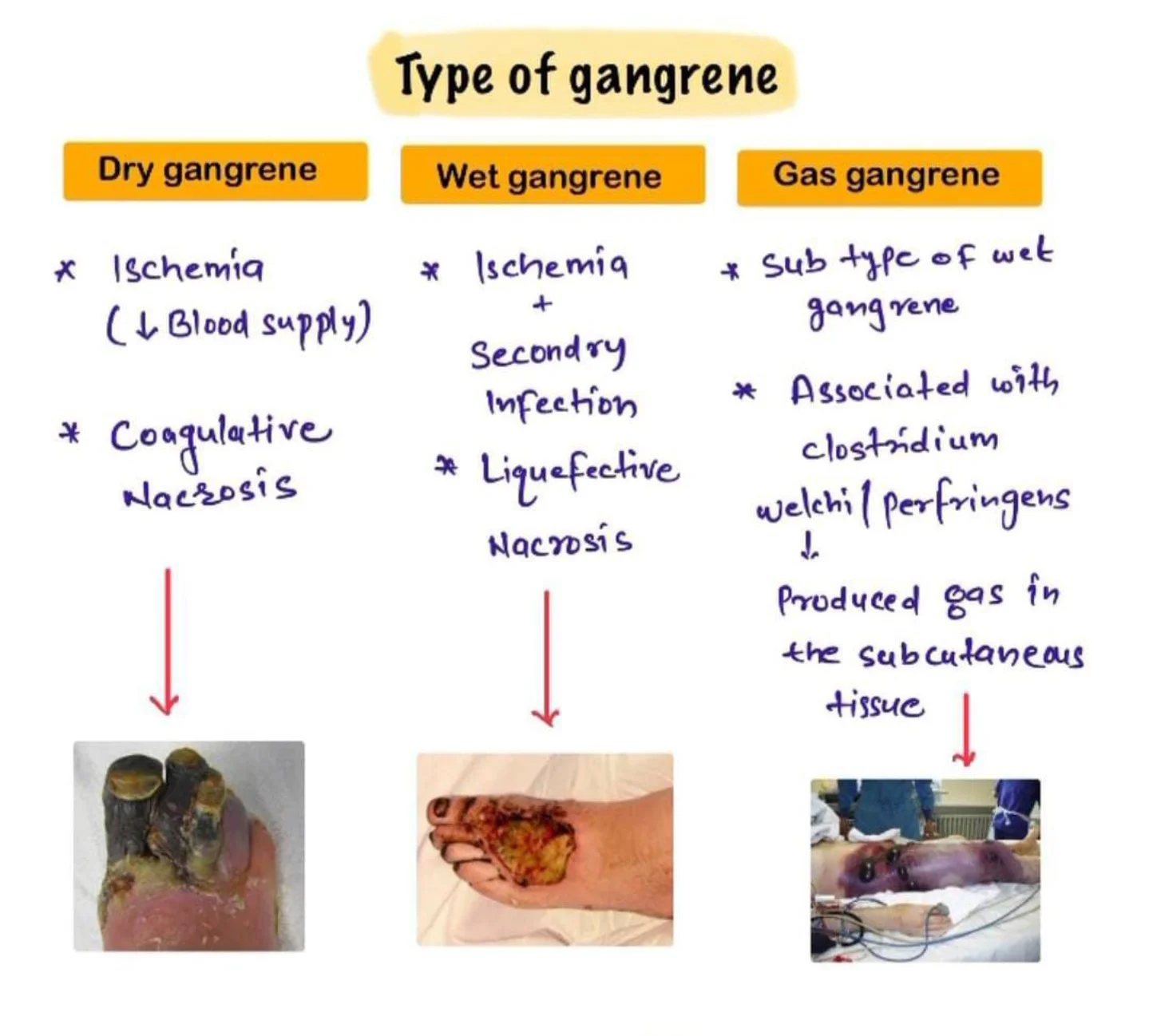
Types of Gangrene
Dry Gangrene
- Dry gangrene begins at the distal part of the limb due to ischemia and often occurs in the toes and feet of elderly patients due to arteriosclerosis (abnormal thickening and hardening of the arterial walls).
- Dry gangrene spreads slowly until it reaches the point where the blood supply is inadequate to keep tissue viable.
- The affected part is dry, shrunken and dark black, resembling mummified flesh.
- If the blood flow is interrupted for a reason other than severe bacterial infection, the result is a case of dry gangrene.
- People with impaired peripheral blood flow, such as diabetics, are at greater risk of contracting dry gangrene.
- The early signs are a dull ache and sensation of coldness in the affected area.
- If caught early, the process can sometimes be reversed by vascular surgery.
- If necrosis sets in, the affected tissue must be removed and treated like a case of wet gangrene.
Wet Gangrene
- Wet gangrene occurs in naturally moist tissue and organs such as the mouth, bowel, lungs, cervix, and vulva.
- Bedsores occurring on body parts such as the sacrum, buttocks and heels (not in “moist” areas) are also categorized as wet gangrene infections.
- In wet gangrene, the tissue is infected by microorganisms, which cause tissue to swell and emit a foul odour.
- Wet gangrene usually develops rapidly due to blockage of venous and/or arterial blood flow.
- The affected part is saturated with stagnant blood which promotes the rapid growth of bacteria.
- The toxic products formed by bacteria are absorbed causing systemic manifestation of bacteria and finally death.
- The affected part is soft, putrid, rotten and dark.
- The darkness in wet gangrene occurs due to the same mechanism as in dry gangrene.
Gas Gangrene
- Gas gangrene is a bacterial infection that produces gas within tissues.
- It is a deadly form of gangrene usually caused by bacteria.
- Infection spreads rapidly as the gases produced by bacteria expand and effect healthy tissue.
- Gas gangrene is caused by environmental bacteria; Clostridium perfringens.
- It can also be from; Group A Streptococcus, Staphylococcus aureus & Vibrio vulnificus.
- These Bacteria are mostly found in soil.
- These environmental bacteria enter the muscle through a wound and cause necrotic tissue and powerful toxins.
- These toxins destroy nearby tissue, generating gas at the same time.
- Gas gangrene can cause necrosis, gas production, and sepsis.
- Progression to toxemia and shock is often very rapid.
- Because of its ability to quickly spread to surrounding tissues, gas gangrene should be treated as a medical emergency.
Internal Gangrene
- Strangulated Hernia: A loop of intestine becomes trapped and its blood supply is cut off.
- Volvulus: Twisting of the intestine.
- Intussusception: A portion of the intestine telescopes into another.
- Ischemic Colitis: Reduced blood flow to the colon.
- Acute Mesenteric Ischemia: Blockage of major arteries supplying the intestines.
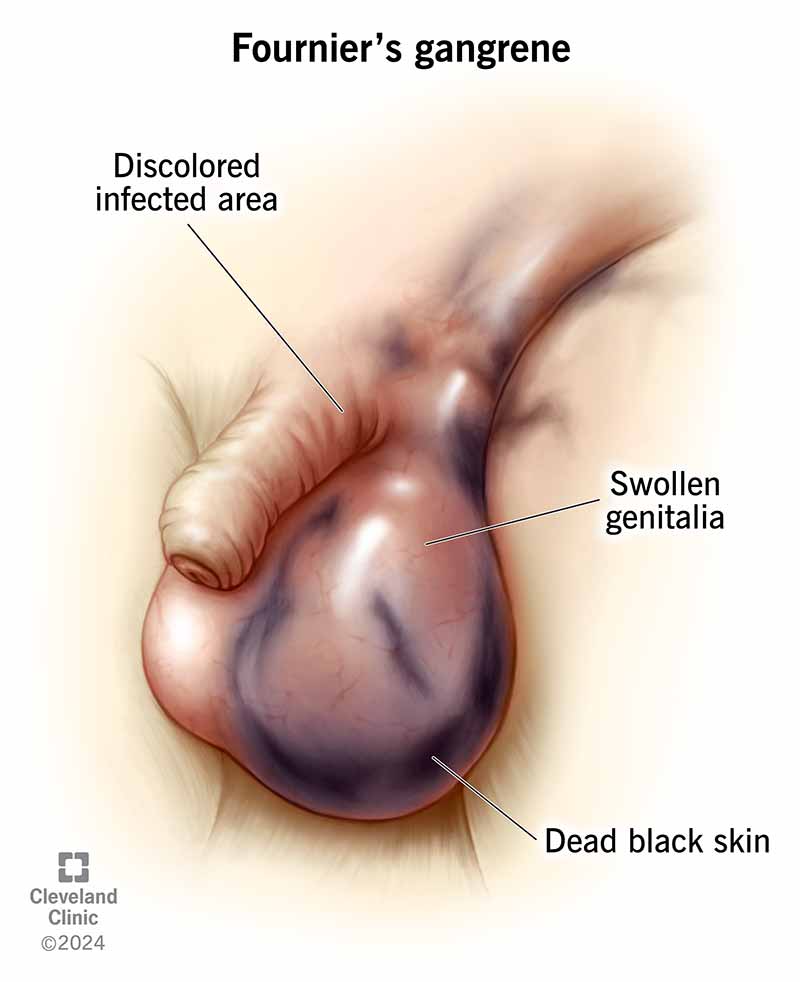
Fournier's Gangrene
Meleney's Gangrene (Progressive Bacterial Synergistic Gangrene)
- Description: A rare, chronic, and progressively spreading necrotizing soft tissue infection, often occurring as a complication of surgery (especially abdominal surgery) or trauma.
- Etiology: Caused by a synergistic infection, typically involving a microaerophilic non-hemolytic Streptococcus and a Staphylococcus aureus.
- Clinical Presentation: Patients develop exquisitely painful, rapidly enlarging skin lesions, often one to two weeks after an operation. The lesion has a characteristic appearance: a central area of necrosis and ulceration surrounded by a purplish zone, which is then surrounded by an outer ring of erythema.
- Management: Requires aggressive debridement and targeted antibiotic therapy.
Risk Factors & Clinical Picture: Who is at Risk and What to Look For
General Risk Factors for Gangrene Development
Any condition that impairs blood flow, compromises the immune system, or increases susceptibility to severe infections can elevate the risk of gangrene.
- Atherosclerosis: Hardening and narrowing of arteries, leading to Peripheral Arterial Disease (PAD).
- Peripheral Arterial Disease (PAD): Critical reduction of blood flow to the limbs.
- Raynaud's Phenomenon: Severe vasoconstriction in fingers and toes, though typically not severe enough to cause gangrene unless prolonged and severe.
- Severe Vasculitis: Inflammation of blood vessels.
- Diabetes Mellitus: A leading cause. Imbalanced blood sugar levels damage blood vessels (micro- and macroangiopathy) and nerves (neuropathy), reducing sensation and blood flow, making feet especially vulnerable to injury and infection.
- Smoking: Significantly damages blood vessels, accelerates atherosclerosis, and reduces oxygen delivery to tissues.
- Obesity: Contributes to diabetes and vascular disease.
- Alcoholism: Can lead to malnutrition and a weakened immune system.
- Intravenous Drug Use (IVDU): Can cause local infections, abscesses, and damage to blood vessels at injection sites.
- Weak Immune System: Conditions like HIV/AIDS, cancer, chemotherapy, or long-term corticosteroid use impair the body's ability to fight infection.
- Serious Injury or Trauma: Crush injuries, deep penetrating wounds, frostbite, severe burns, and scalds can directly damage tissues and blood vessels, leading to ischemia and providing entry points for bacteria.
- Surgery: While rare, can introduce bacteria or compromise blood supply if not managed carefully.
- Direct infection by highly virulent bacteria (e.g., *Clostridium perfringens*, Group A Streptococcus) can cause gangrene even in initially healthy tissue, particularly in necrotizing fasciitis.

Signs and Symptoms: Recognizing the Clinical Presentation
Symptoms typically begin suddenly and can worsen rapidly, especially in wet or gas gangrene. Clinical presentation varies by type but generally includes:
- Pain: Moderate to severe pain, which can be disproportionate to the visible injury (especially in gas gangrene or necrotizing fasciitis). Pain may initially be dull or aching, progressing to intense, throbbing, or burning.
- Skin Discoloration:
- Dry Gangrene: Initial pallor, progressing to dull red, purple, then ultimately black, resembling mummified tissue.
- Wet/Gas Gangrene: Initial pallor or bronze discoloration, rapidly progressing to dark red, purplish, or black.
- Swelling (Edema): Progressive and often rapid swelling around the affected area. The tissue may feel tense and firm.
- Blisters/Bullae: Formation of vesicles or large bullae (blisters) filled with brown, foul-smelling, or serosanguineous (blood-tinged) fluid.
- Foul Odor: A putrid, sweetish, mousy, or decaying smell emanating from the affected tissue, particularly in wet and gas gangrene due to bacterial activity.
- Skin Breakdown: Ulceration, sloughing of skin, and visible decay.
- Crepitus: A palpable crackling or crunching sensation when the affected area is pressed, indicating the presence of gas in the subcutaneous tissues (a hallmark of gas gangrene).
- Fever: Moderate to high-grade fever, often accompanied by chills and rigors.
- Tachycardia: Rapid heart rate.
- Tachypnea: Rapid breathing.
- Hypotension: Low blood pressure, especially as sepsis progresses to septic shock.
- Diaphoresis: Profuse sweating.
- Altered Mental Status: Confusion, disorientation, stupor, or delirium, progressing to coma in severe cases.
- Oliguria/Anuria: Decreased or absent urine output due to kidney injury.
- Nausea, Vomiting, Abdominal Pain: If internal organs are affected.
- General Malaise: Feeling unwell, weakness, fatigue.
Diagnostics: Confirming the Diagnosis and Guiding Treatment
Diagnosis of gangrene is primarily clinical, but diagnostic tests are crucial for confirming the type, identifying the causative organism, assessing the extent of tissue damage, and guiding treatment.
- Complete Blood Count (CBC): Marked leukocytosis (elevated white blood cell count) with a left shift is typical, indicating bacterial infection. Anemia may also be present.
- Inflammatory Markers: Elevated C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR). Procalcitonin levels can also be useful in assessing the severity of bacterial infection.
- Blood Cultures: To identify bacteremia and systemic infection. Crucial for guiding systemic antibiotic therapy.
- Electrolytes, Renal Function Tests (BUN, Creatinine): To assess for fluid and electrolyte imbalances and kidney injury, especially with sepsis.
- Liver Function Tests (LFTs): To assess for liver involvement.
- Blood Glucose: Especially important for diabetic patients to assess control.
- Gram Stain of Fluid/Tissue Aspirate: Rapid identification of bacterial morphology (e.g., Gram-positive rods suggestive of Clostridium).
- Aerobic and Anaerobic Tissue/Fluid Culture and Sensitivity: Definitive identification of causative organisms and their susceptibility to antibiotics. This is critical for targeted therapy.
- Plain X-rays: Can reveal gas in soft tissues (subcutaneous emphysema), especially useful for suspected gas gangrene. May also show foreign bodies or underlying bone involvement (osteomyelitis).
- Ultrasound: Can show fluid collections, tissue edema, and sometimes gas. Also useful for assessing blood flow (Doppler ultrasound).
- Computed Tomography (CT) Scan: Provides detailed cross-sectional images, clearly delineating the extent of soft tissue involvement, fascial plane involvement, and the presence and distribution of gas. Essential for pre-surgical planning.
- Magnetic Resonance Imaging (MRI): Offers superior soft tissue contrast, invaluable for assessing muscle involvement, edema, and differentiating between viable and non-viable tissue. Can be particularly useful for identifying necrotizing fasciitis early.
- Angiography (CT Angiography, MR Angiography, Conventional Angiography): To visualize arterial blood flow and identify blockages in cases of suspected dry gangrene or critical limb ischemia, guiding revascularization procedures.
Management of Gangrene
Managing necrotizing infections like gangrene requires a multi-faceted approach, integrating medical, surgical, and comprehensive nursing interventions. Historically, methods like maggot therapy (biodebridement) were used for necrotic tissue. While largely superseded by antibiotics, maggot therapy has seen a resurgence in specific chronic wound care cases due to its efficacy in consuming only devitalized tissue.
I. Medical & Surgical Management (Collaborative Care)
A. On Admission & Initial Assessment:
- Patient Placement: Admit to a surgical ward; consider isolation precautions (e.g., contact precautions) if the infection is highly virulent or there's significant exudate/drainage. Barrier nursing principles are paramount to prevent cross-contamination.
- Positioning: Position the patient for comfort and to optimize circulation to unaffected areas. Elevate affected limbs if swelling is present, unless contraindicated by arterial insufficiency. Frequent repositioning is essential to prevent pressure injuries.
- Vital Signs & General Observation: Obtain and meticulously record baseline vital signs (temperature, pulse, respiration, blood pressure, oxygen saturation). Observe for signs of systemic infection (JACCOLD: Jaundice, Anemia, Cyanosis, Clubbing, Oedema, Lymphadenopathy, Dehydration – though for acute infection, focus more on fever, tachycardia, tachypnea, hypotension, altered mental status). Assess for signs of sepsis and septic shock.
- Intravenous Access: Establish immediate IV access for fluid resuscitation, antibiotic administration, and other necessary medications, according to physician's orders.
- Pain Assessment: Perform a comprehensive pain assessment using an appropriate pain scale.
B. Investigations:
Prompt diagnostic testing is crucial for identifying the causative organism and assessing the extent of systemic involvement.
- Wound Culture & Sensitivity: Aspirate fluid or tissue from the wound for Gram stain, aerobic and anaerobic culture, and sensitivity testing to guide targeted antibiotic therapy.
- Blood Cultures: Obtain blood cultures (typically two sets from different sites) to identify bacteremia and potential sepsis.
- Imaging Studies:
- X-ray: To determine the presence of gas (crepitus/bubbles) in soft tissues (suggestive of gas gangrene) or bone involvement (osteomyelitis).
- CT/MRI: Provide more detailed visualization of soft tissue involvement, extent of necrosis, and gas patterns.
- Hematological Studies:
- Complete Blood Count (CBC): To assess for leukocytosis (elevated WBC count, indicating infection), anemia (due to chronic disease or blood loss), and platelet count.
- Coagulation Profile (PT/INR, PTT): To assess clotting status, especially in severe sepsis or disseminated intravascular coagulation (DIC).
- C-Reactive Protein (CRP) & Erythrocyte Sedimentation Rate (ESR): Inflammatory markers indicating systemic inflammation.
- Biochemical Studies:
- Electrolytes, Renal Function Tests (BUN, Creatinine): To monitor for fluid and electrolyte imbalances and assess kidney function, especially with antibiotic use or sepsis.
- Liver Function Tests (LFTs): To assess for liver involvement/damage.
- Blood Glucose: Especially important for diabetic patients, as hyperglycemia can worsen infections.
- Type & Crossmatch: Prepare for potential blood transfusions to correct anemia or support hemodynamic stability, especially in severe cases or impending surgery.
C. Treatment (Pharmacological & Surgical):
- Antibiotic Therapy:
- Administer broad-spectrum antibiotics intravenously immediately after cultures are drawn, without waiting for results. Examples include high-dose penicillin (e.g., Penicillin G 2.4 million units IV q4-6h) for clostridial infections, along with synergistic agents like clindamycin to inhibit toxin production.
- Cephalosporins (e.g., ceftriaxone), fluoroquinolones (e.g., ciprofloxacin), and metronidazole (for anaerobic coverage, typically 500mg IV q6-8h) are often part of combination therapy, tailored to suspected pathogens.
- Antibiotics alone are often insufficient because they may not adequately penetrate ischemic or necrotic muscles.
- Antitoxins: In specific cases (e.g., gas gangrene caused by *Clostridium perfringens*), antitoxin administration may be considered, though its efficacy is debated and it's less commonly used than antibiotics.
- Analgesia: Aggressive pain management is crucial. Administer analgesics as prescribed, such as diclofenac 75mg IM, or opioids like tramadol IV or IM, titrated to effect. Consider patient-controlled analgesia (PCA) for severe pain.
- Blood Transfusion: Administer packed red blood cells as indicated to correct anemia and improve oxygen-carrying capacity, especially in hemodynamically unstable patients.
- Surgical Intervention:
- Emergent Debridement: The most critical intervention. Surgical debridement to remove all necrotic, infected tissue is often life-saving. This involves extensive incision and drainage to establish a larger wound opening for aeration (as many causative bacteria are anaerobic) and promote drainage. Repeat debridements may be necessary.
- Amputation: If the limb is extensively gangrenous, non-viable, or threatening the patient's life due to uncontrolled infection, amputation (surgical removal of the limb) may be necessary to prevent further spread and save the patient's life.
- Revascularization: For arterial gangrene, restoring blood flow to the affected area (e.g., bypass surgery, angioplasty) is the best treatment option, as it addresses the underlying ischemia. This may precede or follow debridement depending on the clinical situation.
- Hyperbaric Oxygen Therapy (HBOT): Administration of 100% oxygen at increased atmospheric pressure. This can inhibit the growth of anaerobic bacteria, enhance the killing power of phagocytes, and promote angiogenesis and wound healing. It's often used as an adjunctive therapy, particularly in gas gangrene.
II. Nursing Diagnoses & Interventions
A. Impaired Tissue Integrity (Related to necrotic tissue, infection, impaired circulation)
- Wound Care & Debridement Assistance:
- Assist physician/surgeon with debridement procedures (surgical, mechanical, enzymatic, autolytic).
- Perform meticulous wound care with strict aseptic technique (medical and surgical asepsis). Ensure all equipment and linens are autoclaved and sterile.
- Irrigate wounds as prescribed (e.g., with normal saline, hydrogen peroxide for specific anaerobic infections).
- Apply prescribed dressings (e.g., moist-to-dry, specialized antimicrobial dressings, negative pressure wound therapy [NPWT]).
- Observe the wound closely for bleeding, oozing, increased exudate, foul odor, changes in color, and signs of spreading infection (e.g., cellulitis, crepitus). Document findings thoroughly.
- Monitor drainage and secretions. Implement appropriate isolation precautions (e.g., contact precautions) based on institutional policy and pathogen.
- Educate patient and family on proper hand hygiene and avoiding contamination of the wound.
- Circulatory Management:
- Elevate affected limb if edema is present (unless contraindicated by arterial disease) to promote venous return.
- Assess peripheral pulses, capillary refill, skin color, and temperature regularly in the affected and unaffected limbs.
- Avoid restrictive clothing or bedding that could impede circulation.
- Nutritional Support: Ensure adequate protein, calorie, vitamin (especially C and A), and mineral (zinc) intake to promote wound healing. Consult with a dietitian.
B. Acute Pain (Related to tissue damage, surgical incisions, infection)
- Pain Assessment & Management:
- Regularly assess pain intensity, characteristics, and location using an appropriate pain scale (e.g., 0-10 numeric scale).
- Administer prescribed analgesics proactively and on a schedule, rather than waiting for severe pain. Utilize a multimodal approach (e.g., opioids, NSAIDs, adjuncts).
- Evaluate the effectiveness of pain medication and adjust as needed in collaboration with the physician.
- Teach and encourage non-pharmacological pain relief methods (e.g., relaxation techniques, guided imagery, distraction, repositioning, application of heat/cold if appropriate and safe).
- Comfort Measures:
- Ensure patient is in a comfortable position, using pillows for support.
- Maintain a quiet and calming environment. Minimize unnecessary disturbances.
C. Risk for Infection / Sepsis (Related to invasive procedures, compromised immune status, necrotic tissue)
- Infection Control:
- Adhere to strict hand hygiene before and after all patient contact and procedures.
- Maintain sterile technique for all invasive procedures (e.g., dressing changes, IV insertion, catheterization).
- Monitor for signs of systemic infection (fever, chills, tachycardia, hypotension, altered mental status, increased WBC count).
- Administer prescribed antibiotics on time and monitor for adverse effects.
- Maintain meticulous Foley catheter care (if applicable) to prevent urinary tract infections.
- Ensure proper care of all IV lines to prevent phlebitis or line infections.
- Fluid & Electrolyte Balance: Monitor intake and output, urine specific gravity, and electrolyte levels. Administer IV fluids as prescribed to maintain hydration and perfusion.
- Early Ambulation: Encourage early mobilization as tolerated to prevent complications like pneumonia and deep vein thrombosis (DVT), which can worsen systemic compromise.
D. Disturbed Sleep Pattern (Related to pain, hospital environment, anxiety)
- Environmental Modifications:
- Optimize sleep environment: dim lights, control noise on the ward (e.g., wear soft-soled shoes, lower voices, prompt treatment of alarms).
- Bundle nursing care to minimize nighttime interruptions.
- Comfort & Relaxation:
- Administer pain medication before sleep if pain is a factor.
- Offer warm beverages (if allowed), back rubs, or a quiet conversation.
- Suggest relaxation techniques or play soft, calming music for those who find it helpful.
- Daytime Activities: Encourage appropriate daytime activity and exposure to natural light to help regulate circadian rhythm.
E. Self-Care Deficit (Related to pain, weakness, impaired mobility)
- Hygiene & Personal Care:
- Assist with daily bed baths or showers as tolerated. Maintain personal hygiene.
- Perform oral care at least twice daily, or more frequently if patient is NPO or has a dry mouth.
- Provide meticulous skin care, especially for pressure areas, by repositioning every 2 hours and using pressure-relieving devices.
- Elimination: Ensure regular bowel and bladder elimination. Offer bedpan/urinal frequently or assist to commode/bathroom as mobility allows. Monitor for constipation or urinary retention.
- Encourage Independence: Promote patient independence in self-care activities as much as possible to foster a sense of control and recovery.
III. Long-Term Management & Discharge Planning
A. Patient Education:
Comprehensive patient and family education is vital for successful recovery and prevention of recurrence.
- Medication Compliance: Emphasize the importance of completing the full course of antibiotics, even if symptoms improve, to prevent antibiotic resistance and recurrence.
- Wound Care at Home: Provide clear, step-by-step instructions (and demonstration) on wound care, dressing changes, and signs of infection to report immediately.
- Activity Restrictions: Explain any activity restrictions or limitations on the affected limb/area.
- Nutrition: Reinforce the importance of a balanced diet to support healing.
- Recognition of Complications: Educate on signs and symptoms of potential complications (e.g., worsening infection, fever, increasing pain, changes in wound, signs of sepsis) and when to seek immediate medical attention.
- Lifestyle Modifications: Discuss management of underlying conditions (e.g., strict glycemic control for diabetics, smoking cessation for PVD).
B. Follow-up Care:
- Schedule follow-up appointments with the surgeon, wound care specialist, and primary care provider.
- Arrange for home health nursing services if indicated for complex wound care or continued monitoring.
- Provide contact information for emergencies and questions.
IV. Potential Complications
Close monitoring for and prompt intervention against complications are essential for positive patient outcomes.
- Disfiguring or disabling, permanent tissue damage (e.g., loss of limb function, scarring).
- Osteomyelitis (bone infection).
- Recurrence of infection.
- Sepsis: Life-threatening organ dysfunction caused by a dysregulated host response to infection.
- Septic Shock: Sepsis with persistent hypotension requiring vasopressors and elevated lactate.
- Acute Kidney Injury/Failure (due to sepsis or nephrotoxic medications).
- Liver damage/Jaundice (due to sepsis, severe infection, or certain medications).
- Disseminated Intravascular Coagulation (DIC).
- Acute Respiratory Distress Syndrome (ARDS).
- Stupor
- Delirium
- Coma
- Chronic pain.
- Impaired mobility and functional limitations requiring rehabilitation.
- Psychological distress (anxiety, depression, body image issues).

Proptosis / Exophthalmos
Proptosis of the eye, also known as exophthalmos, is a condition where one or both eyes bulge or protrude from their normal position in the eye sockets. It can be caused by various factors affecting the structures around the eyes.
Proptosis can occur due to a variety of etiologies that increase the volume of the orbital contents.
- Thyroid Eye Disease: One of the common causes of proptosis is thyroid eye disease, also known as Graves’ ophthalmopathy. It occurs when the immune system mistakenly attacks the tissues around the eyes, causing inflammation and pushing the eyes forward.
- Orbital Cellulitis and Infections: Infections in the eye socket, known as orbital cellulitis, can lead to swelling and proptosis.
- Orbital Tumors: Benign or malignant tumors in the eye socket can cause the eyes to bulge out. These growths need to be evaluated and treated promptly.
- Trauma or Injury: Severe injuries to the eye or orbit can displace the eye from its normal position, resulting in proptosis.
- Allergic Reactions: Severe allergic reactions in and around the eyes can cause swelling and push the eyes forward.
- Thyroid disorders, such as hyperthyroidism (overactive thyroid).
- Previous history of eye injuries or surgeries.
- Family history of thyroid eye disease or other eye conditions.
- Certain infections that can affect the eye socket and surrounding tissues.
Proptosis, also known as exophthalmos, can be classified based on different criteria:
- a. Acute Proptosis: Sudden onset of bulging eyes, often associated with infections, trauma, or inflammatory conditions.
- b. Chronic Proptosis: Gradual and persistent eye protrusion, frequently linked to conditions like thyroid eye disease or slow-growing tumors.
- a. Thyroid-Related Proptosis: Caused by thyroid eye disease, usually associated with hyperthyroidism (Graves’ ophthalmopathy).
- b. Inflammatory Proptosis: Resulting from infections or autoimmune disorders that lead to eye inflammation and swelling.
- c. Neoplastic Proptosis: Caused by benign or malignant tumors within the orbit.
- d. Traumatic Proptosis: Arising from injuries or fractures involving the eye and surrounding structures.
- e. Allergic Proptosis: Due to severe allergic reactions affecting the eye and eye socket.
- a. Unilateral Proptosis: Affecting only one eye, often seen in localized conditions or trauma to one eye.
- b. Bilateral Proptosis: Involving both eyes, commonly observed in systemic or thyroid-related causes.
- a. Mild Proptosis: Minimal eye protrusion with no significant impact on vision or eye function.
- b. Moderate Proptosis: Noticeable eye bulging with mild-to-moderate impact on eye movement and visual acuity.
- c. Severe Proptosis: Pronounced eye protrusion with significant visual impairment, restricted eye movement, and potential complications.
It consists of several important parts:
- Cornea: The clear front part that allows light to enter the eye.
- Iris: The colored part of the eye that controls the size of the pupil.
- Pupil: The black center that regulates the amount of light entering the eye.
- Lens: Located behind the iris, it focuses light onto the retina.
- Retina: The back of the eye where images are formed and sent to the brain through the optic nerve.
- Optic Nerve: Carries visual information from the retina to the brain for processing.
The orbit, also called the eye socket, is a bony cavity in the skull that houses the eye and its surrounding structures. The orbit is made up of several bones, including the frontal bone, maxilla, zygomatic bone, and others. It not only protects the eye but also provides support and attachment points for the eye muscles.
Within the orbit, there are important soft tissues that include:
- Extraocular Muscles: These muscles control the movement of the eye in different directions.
- Fat Tissue: Provides cushioning and support for the eye within the orbit.
- Blood Vessels and Nerves: Supply nutrients and transmit sensory information to and from the eye.
Proptosis occurs when there is an abnormal increase in the volume of tissue within the orbit, causing the eye to bulge forward. This can happen due to swelling, growths, or displacement of structures within the eye socket.
As a result of proptosis, the eye is pushed out of its normal position, which can lead to several effects:
- Visible Bulging: The affected eye(s) may appear more prominent than the other eye due to the forward displacement.
- Limited Eye Movement: Proptosis can hinder the normal movement of the eye because of the increased pressure within the confined space of the orbit.
- Exposure of the Eye Surface: The bulging eye may have difficulty closing fully, leading to problems with lubrication and dryness.
- Vision Problems: Proptosis can impact the alignment of the eyes, leading to double vision (diplopia) or blurred vision.

- Bulging or Protruding Eye(s): One of the most noticeable signs of proptosis is when one or both eyes appear to bulge or protrude from their normal position within the eye sockets. The affected eye(s) may look larger and more prominent than usual, which can be concerning for the person experiencing this symptom.
- Redness and Swelling: Proptosis often leads to redness and swelling around the affected eye(s) and the surrounding tissues. The increased pressure within the eye socket can cause inflammation, making the eye area appear puffy and irritated.
- Vision Changes and Diplopia (Double Vision): Changes in vision are common with proptosis. The displaced position of the eye can disrupt the normal alignment, leading to double vision (diplopia). This occurs when the images seen by each eye do not merge properly, resulting in two overlapping images instead of a single clear image.
- Pain or Discomfort: Patients with proptosis may experience varying degrees of pain or discomfort around the affected eye(s) and the surrounding area. The pressure and stretching of tissues within the eye socket can cause pain, which may worsen with eye movement or touch.
- Eyelid Abnormalities: Proptosis can affect the position and function of the eyelids. Some patients may experience difficulty fully closing the affected eye, leading to incomplete blinking and potential corneal exposure, which can cause dryness and irritation.
- Photophobia (Light Sensitivity): Increased protrusion of the eye can make it more sensitive to light, leading to discomfort or pain when exposed to bright lights.
- Watery Eyes: Proptosis can disrupt the normal tear flow and drainage, resulting in excessive tearing (epiphora).
- Displacement of the Eye Muscles: The abnormal position of the eye may cause the extraocular muscles (responsible for eye movement) to become misaligned, leading to limited or abnormal eye movements.
- Changes in Eye Appearance: Aside from bulging, proptosis may cause changes in the appearance of the eye(s), such as a widened palpebral fissure (the opening between the upper and lower eyelids) or changes in the position of the iris.
- Pressure Sensation: Some individuals with proptosis may describe a feeling of pressure or heaviness around the eyes due to the increased tissue volume within the eye socket.

The first step in diagnosing proptosis involves a thorough clinical examination by healthcare professionals, such as ophthalmologists or eye specialists. During the examination, the following assessments may be performed:
- Visual Acuity Test: To assess how well the patient can see at various distances using an eye chart.
- Eye Movement Examination: To check for any limitations or abnormalities in the movement of the affected eye(s).
- Pupil Examination: To evaluate the size and reaction of the pupils to light.
- Eye Pressure Measurement: To check for increased intraocular pressure, which may be associated with certain eye conditions.
- Slit-Lamp Examination: A specialized microscope used to examine the front structures of the eye, including the cornea, iris, and lens.
- Fundoscopy: To visualize the back of the eye (retina and optic nerve) using an ophthalmoscope.
Imaging studies are essential to get a detailed view of the eye and the structures within the orbit. The two most common imaging modalities used for proptosis diagnosis are:
- Magnetic Resonance Imaging (MRI): This non-invasive technique uses powerful magnets and radio waves to create detailed images of the eye, orbit, and surrounding soft tissues. MRI helps identify any abnormal growths, inflammation, or changes in the eye and orbital structures.
- Computed Tomography (CT Scan): CT scans provide cross-sectional images of the eye and orbit, offering precise information about the bony structures and any abnormalities present. It helps in identifying fractures, tumors, or other conditions affecting the eye socket.
- Thyroid Eye Disease (Graves’ Ophthalmopathy): This autoimmune condition is one of the common causes of proptosis and may be associated with other signs of hyperthyroidism.
- Orbital Cellulitis: An infection of the tissues around the eye, causing redness, swelling, and pain.
- Orbital Tumors: Benign or malignant growths that can push the eye forward.
- Allergic Reactions: Severe allergies can cause eye swelling and redness.
- Traumatic Eye Injury: Severe eye injuries may lead to eye displacement and proptosis.
- Treating Underlying Conditions (e.g., Thyroid Disorders): If proptosis is caused by an underlying condition like thyroid eye disease, the primary focus of treatment is managing the underlying disorder. For instance, in Graves’ ophthalmopathy, controlling the overactive thyroid with medications, radioactive iodine, or surgery may help stabilize or improve eye symptoms.
- Corticosteroids and Immunosuppressive Therapy: In certain cases of proptosis associated with inflammation or autoimmune conditions, corticosteroids may be prescribed. These anti-inflammatory medications help reduce swelling and inflammation around the eyes. In more severe cases, immunosuppressive therapy may be used to modulate the immune response and manage the underlying cause.
- Orbital Decompression Surgery: Orbital decompression is a surgical procedure performed to alleviate pressure in the eye socket by creating additional space. It involves removing or reshaping parts of the bony orbit to allow the displaced eye to move back to a more normal position. This surgery is commonly used for patients with proptosis due to thyroid eye disease or other conditions causing compression of the optic nerve.
- Orbital Tumor Removal: If proptosis is caused by benign or malignant tumors within the orbit, surgical removal may be necessary. The goal is to excise the tumor while preserving the surrounding eye structures and restoring a more natural eye position.
- Eye Realignment Surgery: In cases of proptosis resulting from muscle imbalances or nerve problems, eye realignment surgery may be recommended. This procedure aims to reposition the affected eye(s) to improve alignment and reduce double vision.
Nursing care for patients with proptosis is holistic, encompassing patient education, careful monitoring, and significant emotional support.
| No. | Nursing Diagnosis | Interventions & Rationale |
|---|---|---|
| 1 | Risk for Corneal Injury / Dry Eye related to incomplete eyelid closure (lagophthalmos) secondary to proptosis. |
|
| 2 | Disturbed Body Image related to altered facial appearance (bulging eyes). |
|
| 3 | Impaired Visual Perception (Diplopia) related to extraocular muscle displacement and misalignment. |
|
| 4 | Deficient Knowledge related to disease process, eye hygiene, and treatment plan. |
|
- Visual Acuity Checks: Regular visual acuity assessments should be performed to monitor changes in the patient’s vision. Record and report any abnormalities in visual acuity to the healthcare team promptly.
- Assessing for Complications: Monitoring for potential complications related to proptosis, such as signs of optic nerve compression (loss of color vision, reduced visual field), severe corneal exposure, and eye infections. Regular assessments can help detect these issues early, allowing for timely intervention.
- Pre-operative Preparation: Ensure all imaging (MRI, CT) is available. Educate the patient on what to expect post-surgery, including the likelihood of swelling and bruising around the eyes.
- Post-operative Positioning: Following orbital surgeries, nurses will help position the patient to minimize swelling and promote comfort. Elevating the head of the bed (Semi-Fowler's position) and keeping the patient’s head elevated can help reduce post-operative swelling and pressure around the eyes.
- Cold Compresses: Apply prescribed cold compresses gently around (not directly on) the eyes to reduce post-operative edema and discomfort.
- Monitor Neurological and Visual Status: Closely check pupillary response, visual acuity, and eye movements post-operatively to quickly identify complications like retrobulbar hemorrhage or nerve damage.
Proptosis / Exophthalmos Read More »

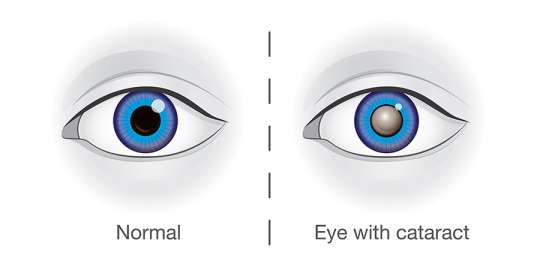
Cataract

Classifications of Cataracts
Age-Related Cataract Classification
A. Morphological Classification

Nuclear Cataract: Occurs in the central nucleus of the lens, often leading to a yellowing or browning of the lens. This type can progress slowly over years. Most common.
CORTICAL CATARACT

Cortical Cataract: Occur on the outer edge/layer of the lens (cortex). Begins on the outer edge of the lens, characterized by white, wedge-shaped opacities that spread towards the center. This type often causes issues with glare.
SUBCAPSULAR CATARACT
- Occur just under the capsule of the lens.
- Starts as a small, opaque area.
- It usually forms near the back of the lens, right in the path of light on its way to the retina.
- It’s interferes with reading vision
- Reduces vision in bright light
- Causes glare or halos around lights at night.
POSTERIOR SUBCAPSULAR CATARACTS

- Posterior Subcapsular Cataracts: Begins at the back of the lens (posterior pole) and spreads to the periphery or edges of the lens. It can be developed when: Part of the eye is chronically inflamed or Heavy use of some medications (steroids).
- Affects vision more than other types of cataracts because the light converges at the back of the lens. Dilating drops are useful in this type by keeping the pupils large and thus allow more light into the eye.
IMMATURE CATARACT

- Immature Cataract: The lens is partially opaque, with some areas remaining clear. Vision is still possible but may be significantly impaired.
MATURE CATARACT
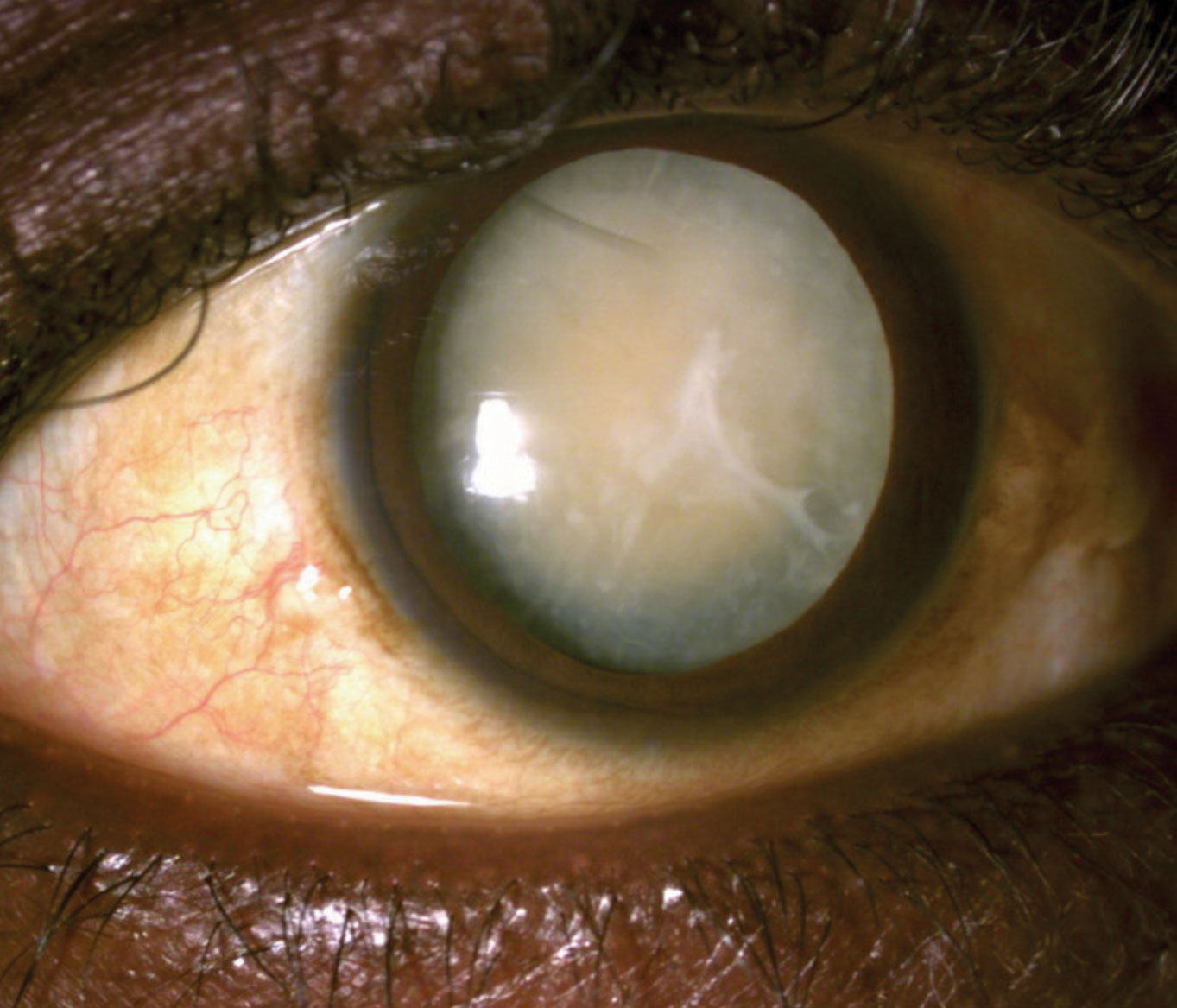
- Mature Cataract: The lens is completely opaque, leading to a significant reduction in vision. The lens may appear pearly white.
- Lens appears pearly white
- Mature cataract, with obvious white opacity at the Centre of pupil.
HYPERMATURE CATARACT ( Morgagnian)
Hypermature Cataract (Morgagnian): The lens cortex becomes liquefied, and the lens nucleus may sink within the capsule. This can lead to a wrinkled anterior capsule and potentially severe complications.
- Intumescent: The proteins in the lens break down and the lens absorbs water and becomes swollen, appearing milky white.
- Liquefactive/Morgagnian Type: Cortex undergoes auto-lytic liquefaction and turns uniformly milky white. The nucleus loses support and settles to the bottom.
CONGENITAL CATARACT

Congenital Cataract Classification
- Occur in about 3:10000 live births.
- 2/3 of case are bilateral (half of the cause can be identified)
- The most common cause is genetic mutation usually.
- It can cause amblyopia(lazy eye) in infants.
It is divided to:
1. Systemic Association
- Metabolic Disorders: Conditions like galactosemia and galactokinase deficiency can cause cataracts in infants.
- Prenatal Infections: Infections like congenital rubella can lead to cataract formation in newborns.
- Chromosomal Abnormalities: Genetic syndromes such as Down syndrome, Patau syndrome, and Edward syndrome are associated with a higher risk of congenital cataracts.
2. Non-Systemic Association
- Idiopathic Cases: In some cases, the cause of congenital cataracts is unknown.
Clinical Findings / Investigations
• The most common objective finding associated with cataracts is decreased visual acuity.
• This is measured with an office wall chart or near-vision card.
- VISUAL ACUITY

Acuity refers to the sharpness of vision or how clearly you see an object.
• In this test, the doctor checks to see how well you read letters from across the room
• Eyes are tested one at a time, while the other eye is covered.
• Using the chart with progressively smaller letters from top to bottom, to determine the level of vision.
2. SLIT LAMP EXAM (SLE)
• SLE allows the ophthalmologist to see the structures of the eye under
magnification.
• The microscope is called a slit lamp because it uses an intense slit of light to illuminate your cornea, iris, and lens.
• These structures are viewed in small sections to detect any small
abnormalities.
3. DILATED EXAM

• Dilating drops are placed in the eyes to dilate the pupils wide and provide a better view to the back of the eyes.
• It allows the ophthalmologist to examine the lens for signs of a cataract and, if needed, determine how dense the clouding is.
• It also allows for examination of the retina and the optic nerve.
• Dilating drops usually keep your pupils open for a few hours before
their effect gradually wears off.
4. REFRACTION

• This is performed by your doctor to see if the decrease in vision is simply
due for need for new glasses, or if there is another process at work that accounts for the decrease in visual acuity.
Treatment/Management of Cataracts
1. Non-Surgical Management.
- Glasses: Cataracts alter the refractive power of the natural lens, so glasses can help maintain good vision.
- Make sure that eyeglasses or contact lenses are the most accurate prescription possible.
- Patient Advice:
- Lighting: Improve home lighting with more or brighter lamps.
- Sunglasses: Wear sunglasses outdoors to reduce glare.
- Night Driving: Limit night driving.
2. Surgical Management.
Indications:
- Changes in eyeglasses no longer improve vision.
- Quality of life is significantly impacted.
- Cataract removal is likely to improve vision (when visual acuity cannot be improved with glasses).
Surgical Techniques:
Phacoemulsification:
- Procedure: A tiny, hollowed tip uses high-frequency (ultrasonic) vibrations to break up the cloudy lens (cataract). The same tip is used to suction out the lens.
- Advantages: Minimally invasive, precise, and generally results in faster recovery.
Extracapsular Cataract Extraction (ECCE):
- Procedure: The nucleus and cortex are removed from the capsule, leaving behind the intact posterior capsule, peripheral anterior capsule, and zonules.
- Advantages: Preserves the capsular bag, reducing the risk of complications like vitreous prolapse.
Intracapsular Cataract Extraction:
- Procedure: The entire lens (nucleus, cortex, and capsule) is removed as a single piece after breaking the zonules.
- Advantages: Eliminates the risk of posterior capsular opacification (after-cataract).
- Disadvantages: Increased risk of complications like vitreous prolapse and retinal detachment.
3. Pre-Operative Assessment:
- General Health Evaluation:
Blood pressure check.
Assessment of patient’s ability to cooperate with the procedure and lie flat during surgery.
Eye Drop Instillation Instruction: Teach patients how to instill eye drops correctly.
Reassurance and Consenting: Provide reassurance and obtain informed consent.
Intraocular Pressure: Ensure normal intraocular pressure or adequate control of pre-existing glaucoma.
4. Post-Operative Care:
- Discharge: Patients are usually discharged home the same day.
Follow-Up: Patients are seen in the office the next day, the following week, and then again after a month to monitor healing progress.
Patient Advice:
Discomfort: Mild discomfort is normal for a couple of days after surgery.
Eye Patch/Shield: Wear an eye patch or protective shield the day of surgery.
Exertion: Avoid strenuous exertion to prevent increased pressure in the eyeball.
Trauma: Avoid ocular trauma.
Medications: The doctor may prescribe medications to prevent infection and control eye pressure:
Steroid drops: To reduce inflammation.
Antibiotic drops: To prevent infection.
Complications of Cataract Surgery
- Infective Endophthalmitis: A rare but severe infection that can lead to vision loss.
- Suprachoroidal Hemorrhage: Severe intraoperative bleeding that can cause permanent vision loss.
- Uveitis: Inflammation of the uvea, more common in patients with diabetes or a history of ocular inflammation.
- Ocular Perforation: A rare but serious complication.
- Refractive Error: Incorrect intraocular lens power can lead to residual vision problems.
- Posterior Capsular Rupture and Vitreous Loss: Can increase the risk of retinal detachment.

Corneal Ulcers
CORNEAL ULCERS
Corneal ulcers are open sores or epithelial defects with underlying inflammation on the cornea, the transparent front part of the eye that covers the iris and pupil.
These ulcers are often visible as grey to white opaque or translucent areas on the normally clear cornea. In some cases, they may be too small to detect without adequate magnification.
The cornea is useful in focusing light on the retina and protecting the inner eye structures. Corneal ulcers can be a serious condition leading to vision loss if not treated.
A Cornea ulcer will often appear as a grey to white opaque or translucent area on the normally clear and transparent cornea. Some corneal ulcers may be too small to see without adequate magnification.
Cornea is the structure in front of the eye. The cornea overlies the iris which is the coloured part of the eye and is separated from the iris by the aqueous fluid in the anterior chamber of the eye.
Signs and Symptoms of Corneal Ulcers
- Redness: The conjunctiva (the white part of the eye) and the anterior chamber may appear red due to dilated blood vessels.
- Eye Pain: Ranges from mild to severe, often worsening with bright light exposure (photophobia).
- Visual Disturbance: Blurred vision, especially if the ulcer is centrally located.
- Tearing and Discharge: Excessive tearing, pus, or thick discharge from the affected eye.
- Foreign Body Sensation: A constant feeling that something is in the eye.
- Swelling: The eyelids may be swollen, and there may be noticeable edema around the ulcer.
- Visible Ulcer: In some cases, a white or grey round spot on the cornea may be visible.
Investigations
- Slit Lamp Examination: A slit lamp microscope is used to examine the eye in detail. A fluorescein dye is often applied to highlight the ulcer, making it more visible under blue light.
- Microbial Cultures: Swabs or scrapings from the ulcer are sent for microscopy, culture, and sensitivity testing to identify the causative organism and guide treatment.
- Corneal Sensitivity Test: This assesses the sensitivity of the cornea, which may be reduced in cases of viral ulcers or chronic conditions.
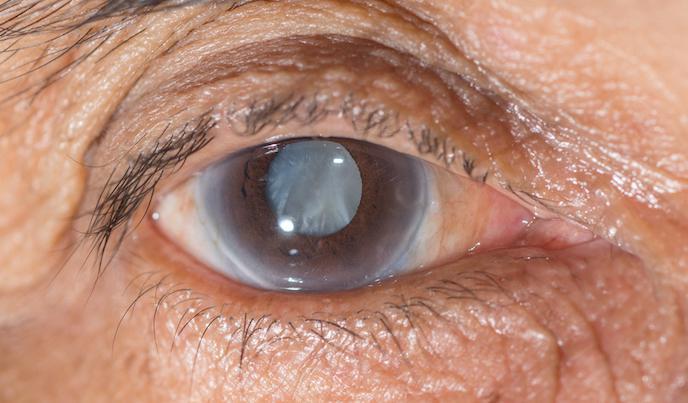
Glaucoma
Normal Pathway of Aqueous Humor
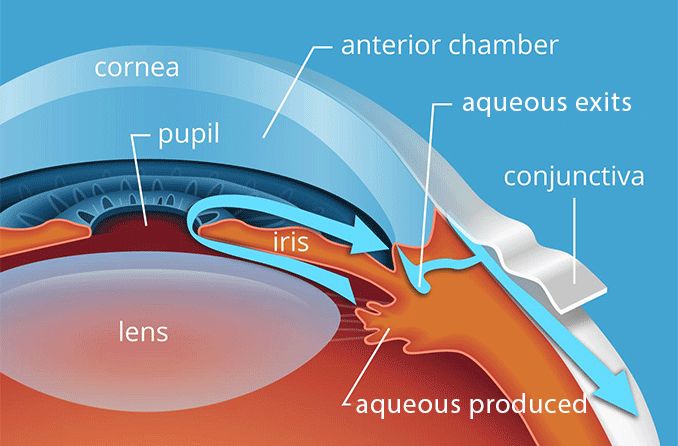
Aqueous fluid Circulation:
- The aqueous fluid is a clear fluid produced in the Cilliary body then it will flow out through the Iris, lens, Pupil, Cornea, Anterior Chamber Trabecular Meshwork then to the Schlemm Canal.
- The aqueous fluid flows nourishing the cornea and lens.
- The eye has an internal fluid circulation system
- Fluid is produced at the base of the iris
- The fluid flows through the pupil to the front of the iris
- The fluid exits the eye at the angle between the iris and the cornea where it drains through a spongy meshwork
The IOP is determined by:
- Rate of aqueous production in the ciliary body
- Resistance encountered by the aqueous as it flows out of the passages.

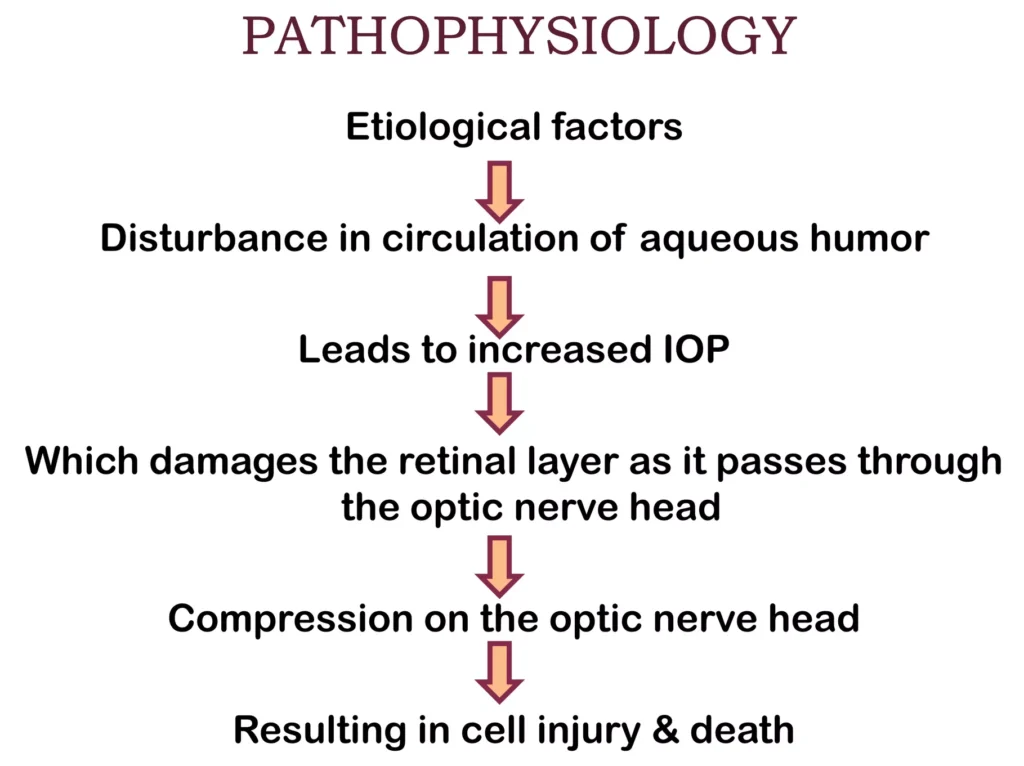
Pathophysiology of Glaucoma
The underlying cause of open-angle glaucoma remains unclear.
Excess production of aqueous humor, and decreased outflow of aqueous humor, are the key factors in the pathophysiology of glaucoma.
Excess production of aqueous humor can occur, leading to an increase in intraocular pressure. Additionally, there may be a decrease in the outflow of aqueous humor due to blockage or narrowing of the drainage pathways.
The increased intraocular pressure puts pressure on the optic nerve, compromising its blood supply and leading to ischemia. The optic nerve is responsible for transmitting visual information from the eye to the brain. When the optic nerve is damaged, it can result in the loss of vision.
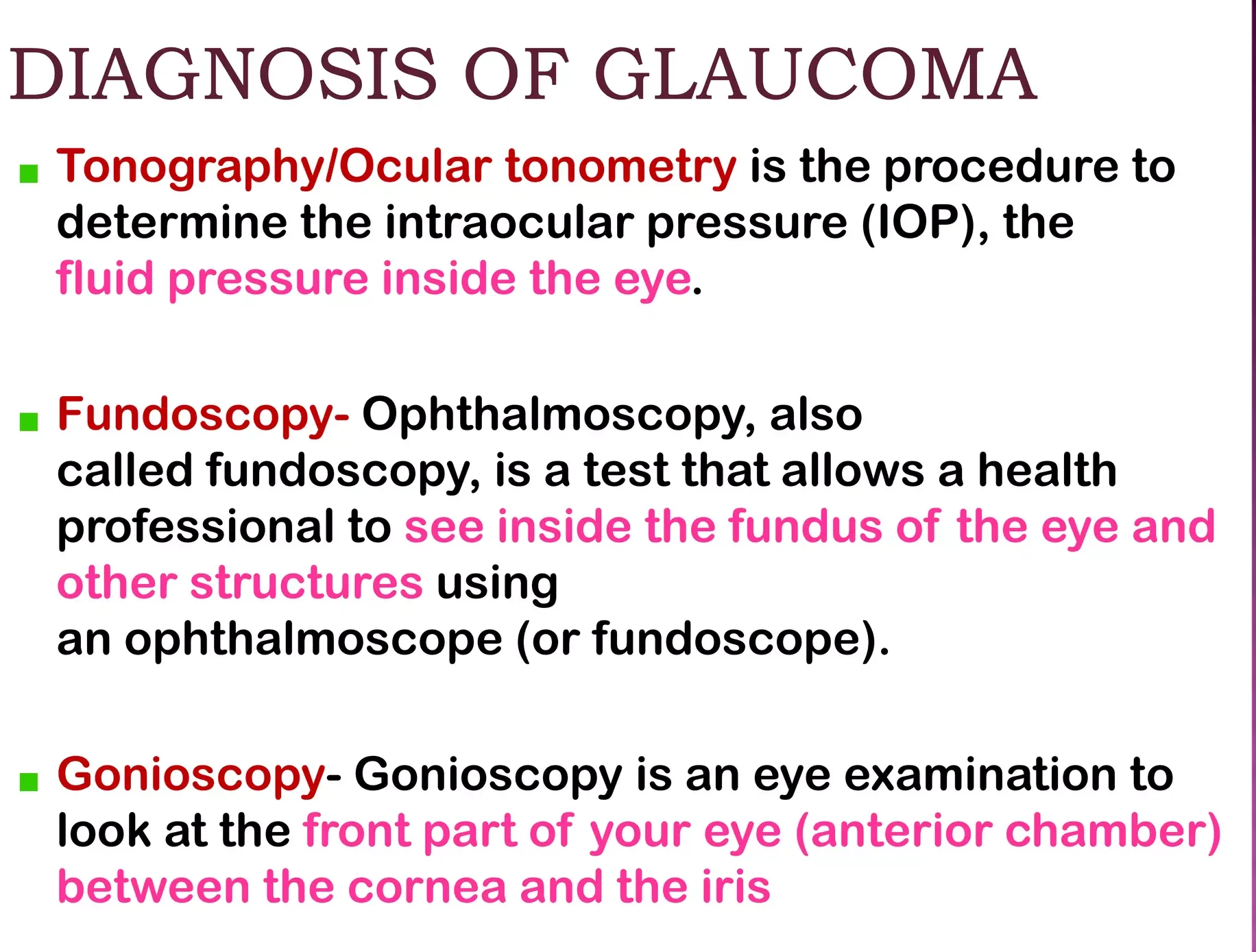
Diagnosis of Glaucoma
Screening for glaucoma is usually performed as part of a standard eye examination performed by optometrists and ophthalmologists.
- History taking: Examination for glaucoma also could be assessed with more attention given to sex, race, history of drug use, refraction, inheritance and family history.
Glaucoma tests;
- Tonometry: This test measures the intraocular pressure (IOP) within the eye. The examiner will numb the eye with eye drops and then use a tonometer to measure the pressure. This can be done by applying a puff of warm air or using a tiny tool.
- Gonioscopy: This test examines the angle where the iris meets the cornea. Eye drops are used to numb the eye, and a hand-held contact lens with a mirror is gently placed on the eye to visualize the angle between the cornea and iris.
- Ophthalmoscopy (Dilated Eye Examination): This test examines the shape and color of the optic nerve. Eye drops are used to dilate the pupil, allowing the examiner to use a magnification device with a light to examine the optic nerve
- Perimetry (Visual Field Test): This test assesses the complete field of vision. Patient is asked to look straight ahead while a light spot is presented in different areas of the peripheral vision. This helps create a map of the vision.
- Pachymetry: This test measures the thickness of the cornea. A pachymeter is gently placed on the front of the eye to measure the corneal thickness. This measurement can help in understanding eye pressure readings.
- Nerve Fiber Analysis: Imaging techniques such as optical coherence tomography, scanning laser polarimetry, and scanning laser ophthalmoscopy can be used to assess the thickness of the retinal nerve fiber layer.
Classification of Glaucoma.
Glaucoma has been classified into specific types:

Congenital Glaucoma
Congenital glaucoma is a rare form of glaucoma that is present at birth or develops shortly after birth.
- It is characterized by abnormalities in the angle of anterior chamber obstructing the outflow of aqueous humour, leading to increased intraocular pressure and potential damage to the optic nerve.
- Congenital glaucoma can manifest at birth ( True Congenital) before 3 years ( Infantile) or between 3-16 years Juvenile).
Clinical Feature of Congenital Glaucoma.
- Age of onset: Congenital glaucoma presents in infants and young children, usually before the age of 3 years.
- Triad of symptoms: The classic triad of symptoms associated with congenital glaucoma includes :
- Watering (epiphora): Excessive tearing or watery eyes.
- Photophobia: Sensitivity to light.
- Blepharospasm: Involuntary contraction or twitching of the eyelids.
- Buphthalmos: Congenital glaucoma can cause enlargement of the eyeball, known as buphthalmos or “ox eye or bull’s eye” . This occurs due to increased intraocular pressure (IOP) and rapid expansion of the eye.
- Corneal changes: The elevated IOP in congenital glaucoma can lead to corneal enlargement and clouding. This can result in corneal edema and opacification, which may cause visual impairment.
- Haab striae: Horizontal or oblique breaks in Descemet membrane, known as Haab striae, can be seen in congenital glaucoma. These striae are a result of the stretching of the cornea due to increased IOP.
- Optic nerve damage: If left untreated or uncontrolled, congenital glaucoma can lead to optic nerve damage. This can result in vision loss.
- Variable presentation: The severity and presentation of congenital glaucoma can vary. Some cases may be unilateral (affecting one eye) while others may be bilateral (affecting both eyes).
- Blepharospasm (involuntary forceful closure of eyes): In congenital glaucoma, blepharospasm is a common clinical feature that refers to the involuntary and forceful closure of the eyelids.
- Excessive lacrimation: Excessive tearing or lacrimation is another common symptom of congenital glaucoma since the increased pressure in the eye can cause the tear ducts to produce more tears than usual.
- Enlarged and edematous cornea: The cornea, the clear front part of the eye, can become enlarged and edematous in congenital glaucoma. The increased pressure in the eye can lead to fluid accumulation in the cornea, causing it to swell which can result in cloudiness and opacification of the cornea.
- Thin and blue sclera: The sclera, the white outer layer of the eye, may appear thin and blue in congenital glaucoma, due to increased pressure in the eye. The blue color is due to the visibility of the underlying choroid layer through the thin sclera.
- Deep anterior chamber: Congenital glaucoma can cause a deepening of the anterior chamber, which is the space between the cornea and the iris. The increased pressure in the eye can push the iris backward, resulting in a deeper anterior chamber.
- Flat lens: In congenital glaucoma, the lens of the eye may appear flat. The increased pressure in the eye can affect the shape and position of the lens. This can lead to changes in the focusing ability of the eye.
- Optic disc atrophy: Optic disc atrophy, which refers to the degeneration and loss of nerve fibers in the optic disc, can occur in congenital glaucoma. The increased pressure in the eye can cause damage to the optic nerve.
Management of Congenital Glaucoma
The management of congenital glaucoma involves a combination of medical therapy and surgical interventions.
The main Aims of management is to lower intraocular pressure (IOP) and prevent further damage to the optic nerve.
Medical Therapy:
- Medical therapy is often used as a temporary measure to control IOP and clear the cornea before surgery.
- Medications such as topical beta-blockers like timolol, betaxolol, or prostaglandin analogs, and carbonic anhydrase inhibitors may be prescribed to reduce IOP.
Surgical Interventions:
1. Angle Surgery: The mainstay of treatment for congenital glaucoma is angle surgery, which aims to improve aqueous outflow and lower IOP.
- Goniotomy: In this procedure, an incision is made across the trabecular meshwork to improve drainage of aqueous humor.
- Trabeculotomy: This surgery involves incising the trabecular meshwork to create a new drainage pathway for aqueous humor.
2. Trabeculectomy: If angle surgery is not successful in controlling IOP, trabeculectomy may be performed. This procedure involves creating a new drainage channel to bypass the trabecular meshwork.
3. Glaucoma Implant Surgery: In cases where other surgical options fail, glaucoma implant surgery may be considered. This involves the placement of a drainage device, such as a Molteno, Baerveldt, or Ahmed implant, to regulate the flow of aqueous humor and lower IOP.
Follow-up and Monitoring:
- Regular follow-up visits with an ophthalmologist are essential to monitor IOP, assess the effectiveness of treatment, and detect any potential complications or disease progression.
- Ongoing management may involve adjustments to medication dosages, additional surgical interventions if necessary, and monitoring for potential long-term complications such as refractive errors or amblyopia.
ACQUIRED GLAUCOMA
Acquired glaucoma refers to glaucoma that develops later in life due to various factors such as age, genetics, underlying medical conditions, or trauma.
It is a chronic and progressive condition that requires ongoing management to control IOP and preserve vision.
It is further divided into;
PRIMARY GLUCOMA.
- Primary Open angle glaucoma.
- Primary angle closure Glaucoma
- Chronic angle closure glaucoma.
SECONDARY GLAUCOMA
- Lens induced glaucoma
- Glaucoma due to uveitis
- Neurovascular Glaucoma
- Glaucoma associated with intraocular tumor
- Steroid induced glaucoma.

PRIMARY OPEN-ANGLE GLAUCOMA (POAG)
Primary Open-Angle Glaucoma (POAG) also called as open angle glaucoma or chronic simple glaucoma or simple complex glaucoma results from the overproduction of aqueous humour through trabecular mesh work resulting into increased IOP and damage to optic nerve, resulting into loss of vision.
In this type there in no narrowing of the anterior chamber BUT there is resistance in the trabecular meshwork to aqueous flow resulting in gradual increase in IOP along with cupping of the optic disc and visual fields defects.
Predisposing factors for primary glaucoma include:
- Cigarette smoking.
- Diabetes Mellitus and Hypertension diseases.
- Myopia (nearsightedness).
- Old age.
Clinical features of primary glaucoma may include:
- Asymptomatic in the early stages.
- Mild headache and pain in the eye.
- Difficulty in reading.
- Delayed dark adaptation.
- Alteration in vision sites.
- Mild ache in the eyes
- Increased IOP ( more than24 mmhg)
- Loss of Peripheral vision
- Reduced visual acquity at night.
- Corneal edema
- Visual field deficit.
Investigations for primary glaucoma include:
- Tonometry: To measure intraocular pressure (IOP). In glaucoma, IOP may remain permanently high in the late stages and fluctuating in the early stages.
- Gonioscopy: To assess the angle of the anterior chamber. Narrowing of the angle may be observed in glaucoma.
- Fundus examination: Done with the use of ophthalmoscopy and a slit lamp biomicroscope to look for disc changes.
- Perimetry: To assess changes in the visual field.
Treatment options for primary glaucoma include:
Medical treatment: This is the first choice for open-angle glaucoma.
- Topical beta blockers: These drugs lower the production of aqueous fluid, thereby reducing IOP. Examples include Timolol mealate: (2.5-5 mg B.D), Betaxolol 25mg B.D, Levabunolol 2.5-5% B.D it has a longer effect
- Dorzolamide(2%): It lowers IOP by decreasing the production of aqueous fluid.
- Latanoprost(0.5): It decreases the flow of aqueous fluid.
- Pilocarpine: It contracts the ciliary muscle and opens the trabecular meshwork, allowing increased outflow of aqueous humor.
- Adrenergic group: Drugs like epinephrine hydrochloride decrease aqueous production through vasoconstriction.
Surgical treatment: Surgery is considered when there is a failure to respond to maximal medical therapy.
- Laser therapy: Laser trabeculoplasty (ALT) may be performed if the patient does not respond to medical treatment
- Filtering surgery: Trabeculectomy is a surgical procedure that creates an opening in the white of the eye to allow fluid to leave the eye.
- Drainage tubes: Small tubes may be inserted in the eye to drain excess fluid and lower IOP.
- Minimally invasive glaucoma surgery (MIGS): These procedures have less risk and require less postoperative care compared to traditional surgeries