Introduction to Mycology
Medical Mycology
By the conclusion of this exhaustive master guide, you will be deeply conversant with:
- The fundamental differences between the Kingdom Fungi and bacteria or plants, focusing on ultrastructure and metabolic pathways.
- The exact morphological classifications (Yeasts, Molds, Dimorphic Fungi) and their microscopic hallmarks (e.g., septate vs. aseptate hyphae).
- The Taxonomic and Clinical classifications of fungal diseases (Mycoses), ranging from superficial skin infections to fatal systemic invasions.
- Strict, protocol-driven specimen collection methodologies and the specialized stains and culture media required to grow and identify fungi in the laboratory.
- The high-yield Pharmacology of Antifungal Agents, identifying exact molecular targets within the fungal cell wall and cell membrane.
I. Introduction to Mycology
Mycology is the specialized biological study of fungi (singular: fungus). The term is derived from "Mykes," the Greek word for mushrooms. While human biology often focuses heavily on plants, animals, and bacteria, fungi represent an entirely separate, massive, and highly evolved kingdom of life.
Diversity and Ecological Scope
- Massive Populations: By 2011, fungal species were estimated to outnumber plants by at least a 6 to 1 ratio. More recent estimates, utilizing advanced high-throughput DNA sequencing methods, suggest that approximately 5.1 million distinct fungal species exist on Earth.
- Clinical Relevance: Despite this staggering biodiversity, only a few hundred of these species possess the physiological mechanisms required to survive at 37°C and evade the human immune system to actually cause human disease.
Mycoses & Unique Phenotypic Features
Diseases directly caused by fungal invasion or overgrowth are clinically termed Mycoses. In the diagnostic laboratory, fungi can present with highly unique, striking phenotypic features that aid microbiologists in immediate presumptive identification:
- Pigment Production: Many fungi produce intense, macroscopic pigments. Example: Rhodotorula species (an opportunistic yeast often found contaminating central venous catheters) produce a characteristic, brilliant salmon-pink to coral-red pigment on agar plates.
- Mucoid Appearance: Certain fungi appear incredibly mucoid, wet, and slimy on agar media. This is visually indicative of a massive polysaccharide capsule encompassing the cell. Example: Cryptococcus neoformans utilizes this thick, slimy capsule to evade phagocytosis by human macrophages, allowing it to cross the blood-brain barrier and cause severe meningitis.
II. Fungal Microscopic Morphologies
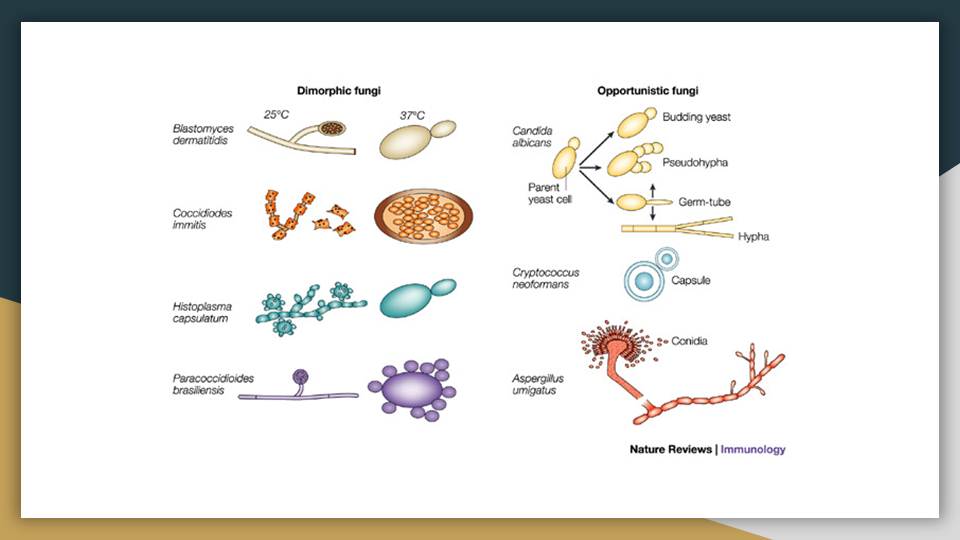
Fungi generally exist in one of two distinct morphological forms: Yeasts or Molds (Moulds). Some highly adapted, medically important fungi can exist as both, depending on the environmental temperature—a phenomenon called Thermal Dimorphism.
A. Yeasts
- Structure: Yeasts are simple, single-celled eukaryotic organisms. They are typically spherical, ellipsoid, or oval in shape.
- Reproduction: They multiply asexually through a process called budding. The newly pinched-off daughter cell is officially termed a blastoconidium (the "blast" or offspring of the mother cell).
- Growth Pattern: In human tissue, they can grow extracellularly in the bloodstream or hide intracellularly within host macrophages to evade immune detection.
- Pseudohyphae vs. True Hyphae: When budding daughter cells elongate but delay detachment—remaining physically attached in a long, "sausage-like" chain—they form Pseudohyphae (fake hyphae). This is a classic hallmark diagnostic feature of Candida albicans in clinical smears. True hyphae (which C. albicans can also form via "germ tubes") have parallel, straight walls without constrictions at the septa.
- Culture Characteristics: On standard agar media, yeast colonies look remarkably similar to bacterial colonies—smooth, creamy, pasty, and opaque. They mature relatively quickly for fungi, usually within 24 to 72 hours, though some fastidious species may require up to 5 days.
- Clinical Examples: Candida spp., Cryptococcus neoformans, and Malassezia furfur.
B. Molds (Moulds)
- Structure: Molds are complex, multicellular organisms that form long, continuous, branching, filamentous tube-like structures called hyphae (singular: hypha).
- The Mycelium: As individual hyphae grow, branch, and intertwine, they form a dense, macroscopic, woven network visible on the agar plate or decaying food called a Mycelium.
- Types of Hyphae:
- Vegetative hyphae: These penetrate deep down into the agar surface (or deeply into the host's necrotic tissue) to physically absorb nutrients, functioning similarly to the roots of a plant.
- Aerial hyphae: These project upwards into the air above the agar surface. They appear as hairy, fuzzy, or fluffy structures and bear the reproductive fruiting bodies that release microscopic spores / conidia into the wind.
- Culture Characteristics: On media, molds appear distinctly fluffy, fuzzy, woolly, or cotton-like. Most produce striking diagnostic pigments (e.g., forest green, deep black, bright yellow) on the surface or reverse side of the agar. Molds grow very slowly, taking anywhere from 3 days to 4 weeks to fully mature.
- Clinical Examples: Aspergillus fumigatus, Trichophyton tonsurans, and Microsporum canis.
C. Hyphal Architecture (Septate vs. Aseptate)
A critical diagnostic feature a pathologist looks for under the microscope is whether the mold's hyphae have internal walls.
The long hyphal tubes are divided into individual compartments (cells) by distinct, regularly spaced transverse cross-walls called "septa." These septa usually have tiny pores allowing cytoplasm to flow between cells.
Clinical Example: Aspergillus species classically present as narrow, septate hyphae that branch at acute, 45-degree V-shaped angles.
The hyphal tubes are continuous, wide, and hollow with absolutely NO cross-walls. The cytoplasm flows freely, containing multiple free-floating nuclei.
Clinical Example: Finding broad, ribbon-like, aseptate hyphae branching at wide 90-degree right angles in a necrotic tissue biopsy is the classic hallmark of Mucormycosis (caused by Rhizopus or Mucor), a rapidly fatal, flesh-eating fungal infection seen in diabetic ketoacidosis.
III. Fungal Cell Ultrastructure
The absolute foundation of medical mycology and antifungal pharmacology relies on understanding that fungi are Eukaryotes. Unlike bacteria (which are simple prokaryotes), fungal cells are evolutionarily closer to human cells. They possess a true, membrane-bound nucleus containing multiple chromosomes, alongside complex organelles such as mitochondria, rough and smooth endoplasmic reticulum, and Golgi apparatus.
| Cellular Feature | Fungi (Eukaryote) | Bacteria (Prokaryote) |
|---|---|---|
| Size (Diameter) | Large (2 - 15 µm) | Small (0.5 - 2.0 µm) |
| Nuclear Structure | True nucleus enclosed by a well-defined nuclear membrane. | No nuclear membrane (free-floating nucleoid region). |
| Internal Organelles | Mitochondria, ER, Golgi, and massive vacuoles present. | None (Absolutely no membrane-bound organelles). |
| Cell Membrane Sterols | Sterols are abundant (Specifically Ergosterol). | Sterols are generally absent (except in Mycoplasma). |
| Cell Wall Composition | Complex Polysaccharides (Beta-glucans, mannans, chitin). No peptidoglycan. | Composed almost entirely of Peptidoglycan (Murein). |
| Spores | Produce a wide, complex variety of sexual and asexual reproductive spores. | Produce Endospores strictly for survival in harsh conditions, not for reproduction. |
The Fungal Cell Wall: Chitin & Glucan
Unlike plants (which rely on cellulose) and bacteria (which rely on peptidoglycan), the fungal cell wall is a rigid, multi-layered armor composed of beta-glucans, mannoproteins, and Chitin (a tough polymer of N-acetylglucosamine, which is the exact same substance that makes up the hard exoskeletons of insects and crabs).
Pharmacological Rule: Because there is absolutely NO peptidoglycan in a fungal cell wall, standard antibacterial antibiotics like Penicillin, Cephalosporins, or Vancomycin are 100% useless against fungal infections!
The Fungal Cell Membrane: Ergosterol
Just beneath the cell wall lies the phospholipid bilayer of the cell membrane. To maintain structural fluidity, mammalian (human) cell membranes use Cholesterol. Fungal cell membranes, however, utilize a unique, synthesized sterol called Ergosterol.
IV. Characteristics of Fungi
A. Habitat & Ecological Role
Fungi are ubiquitous; they are found globally in soil, on plants, in water, and decaying organic matter. Ecologically, they are the primary decomposers of the planet, breaking down dead wood and leaves to recycle carbon and nitrogen. While most are environmental saprophytes (living on dead matter), some species have evolved to live peacefully as normal flora in/on humans:
- Malassezia furfur: Normal lipophilic (fat-loving) flora on the sebum-rich areas of human skin (chest, back, scalp).
- Candida species: Normal flora on the skin, oral cavity, gastrointestinal tract (GIT), and the female genital tract. They only cause disease when the host's immune system or normal bacterial flora is disrupted (e.g., after heavy antibiotic use).
B. Growth Requirements
- Air: Most fungi are strictly aerobic (they require oxygen to survive). There are very few anaerobic fungi.
- pH: A slightly acidic environment of pH 5.6 to 6.0 is optimal for fungal growth. (Laboratory Application: This is why fungal laboratory agars, like Sabouraud Dextrose Agar, are deliberately made highly acidic—it actively encourages fungi to flourish while chemically inhibiting the growth of contaminating environmental bacteria!)
- Moisture: Fungi strongly prefer a humid, moist environment. (This is why fungal skin infections like athlete's foot thrive in sweaty socks and locker rooms).
- Temperature & Thermal Dimorphism:
- Room Temperature (25°C - 30°C): Optimal for environmental Molds.
- Body Temperature (37°C): Optimal for Yeasts.
Thermal Dimorphism: "Yeast in the Beast, Mold in the Cold!"
Certain highly pathogenic fungi (like Histoplasma capsulatum or Coccidioides immitis) are strictly Dimorphic. They physically alter their entire genetic expression and morphology based on environmental temperature to survive and infect.
- At 25°C (in the "cold" room temperature / soil), they grow as infectious, spore-releasing Molds. A patient inhales these microscopic mold spores from the dust.
- Once inhaled, at 37°C (inside the hot "beast" / human lungs), the heat triggers a morphological shift. The spores rapidly convert into single-celled Yeasts. Yeasts are much harder for human white blood cells to destroy, allowing the fungus to disseminate through the blood!
C. Fungal Reproduction
Fungi possess incredibly complex life cycles designed for maximum environmental dispersion.
- Budding: The defining asexual reproductive feature of yeast fungi.
- Conidia or Spores: The defining reproductive feature of mold fungi. Millions of microscopic spores can be released from a single mold colony.
- Mold Reproduction Cycle: Molds can reproduce through both asexual (anamorph state) and sexual (teleomorph state) pathways.
- Asexual Reproduction: Spores (conidia) germinate to produce vegetative mycelium. Aerial hyphae produce specialized sacs (sporangia) or exposed structures (conidiophores) which burst to release millions of genetically identical cloned spores.
- Sexual Reproduction: Occurs when environmental conditions are harsh, ensuring genetic diversity. It involves Plasmogamy (fusion of cytoplasm from two different mating types), Karyogamy (fusion of the two nuclei), and finally Meiosis to produce genetically robust, diverse spores (e.g., Zygospores, Ascospores).
V. Classification of Fungi
Because the fungal kingdom is so massive and diverse, scientists and clinicians use completely different frameworks to group them depending on their specific professional needs. We classify fungi using three main criteria:
- Scientific classification criterion (Taxonomic/Botanical origins).
- Morphological classification criterion (Based on physical appearance under a microscope in the lab).
- Clinical or Medical classification criterion (Based on the anatomical site of human infection).
A. Scientific (Taxonomic) Classification Criterion
Historical Context: Initially, early biologists classified fungi alongside plants because they grew out of the ground and their spores looked like seeds. The naming of fungi remains strictly governed by the International Code of Botanical Nomenclature.
The Paradigm Shift: Modern genomics proved Fungi are NOT plants! Plants make their own food via photosynthesis (Autotrophs). Genetically and metabolically, fungi are actually closer to animals. Fungi are Heterotrophic Osmotrophs; they cannot make food. They secrete powerful digestive enzymes outward into the environment, dissolve the organic matter (like a dead tree or human skin), and absorb the liquid nutrients.
The Taxonomic Tree:
- Kingdom: Myceteae
- Division: Amastigomycota (Meaning fungi that completely lack flagella/motile swimming cells).
- Four Subdivisions (Phyla):
- Zygomycotina: Produce thick-walled sexual resting spores called zygospores. Include the rapid-growing bread molds like Rhizopus.
- Ascomycotina: The "sac fungi". Produce sexual ascospores inside a specialized sac called an ascus. Includes Saccharomyces and many Aspergillus species.
- Basidiomycotina: The "club fungi". Produce sexual basidiospores on a club-shaped structure. Includes macroscopic mushrooms and the human pathogen Cryptococcus.
- Deuteromycotina (Fungi Imperfecti): A massive "holding category". These are fungi where scientists have never observed them reproducing sexually in a laboratory setting. Because their sexual phase is unknown, they are deemed "imperfect." The vast majority of medically important human pathogens (like Candida and Dermatophytes) were historically placed in this category.
B. Morphological Classification Criterion
This is the most practical classification for laboratory technicians looking down a microscope.
- Yeasts: Single-celled, budding organisms. Examples: Candida spp., Cryptococcus, Malassezia furfur.
- Moulds (Molds): Multicellular, filamentous, hyphae-forming organisms. Examples: Aspergillus, Penicillium.
- Dimorphic Fungi: Fungi that can switch between yeast and mold forms depending on the temperature. Examples: Histoplasma, Coccidioides, Blastomyces.
VI. Clinical or Medical Classification Criterion
In human medicine, the primary way doctors classify mycoses is strictly by the anatomical depth and site affected by the fungal disease.
Definition: Infections strictly limited to the outermost, dead, non-vascular body surfaces: the highly keratinized layers of the skin (stratum corneum), hair, nails, and mucous membranes. They rarely trigger a massive systemic immune response.
- Dermatophytoses (Tinea / Ringworm): Caused by a specialized group of fungi that literally secrete keratinase enzymes to eat keratin for food. Includes Tinea capitis (scalp), Tinea corporis (body ringworm), and Tinea pedis (Athlete's foot).
Mnemonic for Dermatophytes (M.E.T.): Microsporum, Epidermophyton, and Trichophyton. - Pityriasis (Tinea) versicolor: Caused by the lipid-loving yeast Malassezia furfur. Presents as hyper- or hypo-pigmented scaly patches on the chest and back. Microscopically appears as "spaghetti and meatballs" (short hyphae and clustered yeast).
- Candidiasis: Candida albicans overgrowth on mucosal surfaces causing Oral Thrush (white plaques in the mouth) or vulvovaginal yeast infections.
Definition: Deep, chronic, localized infections that penetrate the epidermis to affect the dermis, subcutaneous connective tissue, and muscle. They are almost universally caused by traumatic implantation of environmental fungi from soil or vegetation directly into a wound.
- Sporotrichosis ("Rose Gardener's Disease"): Caused by the dimorphic fungus Sporothrix schenckii. Classically presents in landscapers who prick their finger on a rose thorn. Nodular, ulcerating lesions slowly travel linearly up the arm following the lymphatic drainage tract.
- Chromoblastomycosis: Caused by dematiaceous (dark-pigmented) soil fungi like Fonsecaea pedrosoi. Causes massive, chronic, warty, cauliflower-like lesions on the lower limbs of agricultural workers.
- Mycetoma (Madura Foot): Caused by fungi like Madurella mycetomatis. Results in massively swollen, deformed limbs with sinus tracts draining pus and fungal granules to the skin surface.
The "Bacterial-Like Fungi" Anomaly: Actinomycosis (Actinomyces israelii) and Nocardiosis (Nocardia spp.) cause identical subcutaneous mycetomas. However, these organisms are actually branching, filamentous Bacteria, NOT true fungi! Because the clinical presentation (granulomatous draining tracts) is identical to fungal infections, they are historically grouped together in mycology courses.
Definition: Severe, devastating, and often fatal infections where internal organs are deeply invaded (lungs, brain, bloodstream, liver). They usually begin via inhalation of spores into the lungs. They are frequently opportunistic infections seen in immunocompromised patients (e.g., severe HIV/AIDS, profound neutropenia from chemotherapy, or post-organ transplant).
- Bloodstream Candidiasis (Candidemia): Candida albicans escaping the gut/skin and reaching the sterile blood, causing fatal sepsis.
- Invasive Pulmonary Aspergillosis: Aspergillus fumigatus rapidly invading lung tissue and destroying major blood vessels in leukemic patients, causing massive pulmonary hemorrhage.
- PJP (Pneumocystis jirovecii pneumonia): An atypical fungus causing a lethal, suffocating pneumonia. It is a hallmark, massive AIDS-defining illness.
- Cryptococcal Meningitis: Cryptococcus neoformans spores inhaled from pigeon droppings. The yeast disseminates to the brain, causing lethal swelling and meningitis in AIDS patients.
- Mucormycosis (Zygomycosis): Caused by Rhizopus and Mucor. A highly aggressive, flesh-eating fungal infection that invades the nasal sinuses and destroys the face/eyes/brain, extremely common in poorly controlled diabetics (Diabetic Ketoacidosis provides the perfect acidic, iron-rich environment for the fungus).
- Endemic Dimorphic Granulomas: Histoplasma capsulatum (found in bat/bird guano in the Ohio River Valley) causing severe TB-like lung granulomas.
Fungi don't just cause disease by actively invading human tissue. They can cause immense physiological harm via toxins and immune hyper-reactions.
- Allergies: Severe Type I and Type III hypersensitivity reactions to inhaled airborne fungal antigens (spores), leading to severe asthma or Allergic Bronchopulmonary Aspergillosis (ABPA).
- Mycotoxicoses: Severe, acute, or chronic poisoning caused by ingesting secondary fungal metabolites (toxins) growing on food supplies.
- Aflatoxin B1: Produced by Aspergillus flavus growing on poorly stored peanuts and grains. It aggressively mutates the human p53 tumor suppressor gene, directly causing Hepatocellular Carcinoma (Liver Cancer).
- Ergot Alkaloids: Produced by Claviceps purpurea on rye grain. Causes severe vasoconstriction (gangrene of limbs) and severe hallucinations (historically linked to the Salem Witch Trials).
- Mycetismus: Mushroom poisoning. Eating inherently poisonous macroscopic mushrooms like Amanita phalloides (The "Death Cap" mushroom), whose amatoxins halt human RNA polymerase II, causing acute, fatal liver necrosis within days.
VII. Specimens Collection for Fungal Diagnosis
Proper specimen collection is the absolute most critical step in clinical mycology. Fungi grow incredibly slowly on agar. If a sample is heavily contaminated with fast-growing bacteria from the patient's normal skin flora, the bacteria will swarm the plate within 24 hours, completely destroying and masking the fungal culture.
- Skin, Hair, and Nails (Infections of Keratinized Tissue):
- Preparation: Swab the entire area vigorously with 70% ethanol first. Rationale: This kills the normal bacterial flora on the skin so they don't overgrow the slow-growing fungus in the lab. It also removes surface oils.
- Skin: Do not just scrape the center of a ringworm lesion (it is usually dead and empty). Vigorously scrape skin scales from the active, red, advancing border of the lesion using the blunt edge of a sterile scalpel blade.
- Hair: Use a Wood's Lamp (UV light); some infected hairs will fluoresce brilliant green. Pluck the infected hair out by the root with sterile forceps directly into a sterile petri dish.
- Nails: Scrape away the crumbly top layer and collect subungual debris from deep under the nail bed.
- Subcutaneous Mycoses & Abscesses:
- Abscess: Clean the area with 70% ethanol, then forcefully aspirate deep pus from the center of the nodule using a needle and syringe into a sterile container. Never use a superficial cotton swab, as it will only pick up skin flora and miss the deep fungal elements.
- Subcutaneous: Perform a surgical punch biopsy to get a core of deep infected tissue.
- Respiratory Mycoses:
- Bronchoalveolar lavage (BAL), transtracheal aspirate, or direct lung biopsies are far superior and exponentially more diagnostically accurate than expectorated (coughed-up) sputum. Sputum gets heavily contaminated with oral bacteria and saliva as it passes through the mouth.
- Systemic & Other Infections:
- GIT infections: Stool swab, placed in a specialized transport medium.
- Urine: Must be obtained strictly by sterile catheterization or midstream clean-catch to avoid heavy perineal/vaginal yeast contamination.
- Blood: Collect heavily in routine automated blood culture bottles or specialized fungal lysis-centrifugation blood culture tubes.
- Body Fluids (CSF, Synovial, Pleural): Collect 3-10ml in a plain sterile tube or a tube with an anticoagulant to prevent clotting of fibrin which traps the fungi.
- Bone Marrow: Collect in a yellow-topped vacutainer tube containing SPS (Sodium Polyanethol Sulfonate) anticoagulant, which prevents clotting and also neutralizes human white blood cells that might eat the fungi in the tube.
VIII. Fungal Identification in the Mycology Lab
Direct microscopic examination is incredibly valuable because it is rapid and cost-effective. When properly executed, it can provide an immediate presumptive diagnosis (e.g., seeing broad aseptate hyphae in a diabetic patient), allowing clinicians to start life-saving, highly toxic antifungal therapy immediately, weeks before the slow-growing cultures mature. Identification is based on three main pillars:
- Staining results & microscopic morphology (Looking for specific hyphae, yeast cells, and unique conidia/spore patterns).
- Colony morphology on the agar plate (Is it a pasty yeast, a powdery mold, or a deeply pigmented colony?).
- Growth patterns and biochemical tests on highly selective media.
A. Pre-Analytical Reagents & Mucolytics
Before staining can even begin, thick biological specimens like dense sputum, thick pus, or solid tissue must be chemically digested. This "frees" the fungal elements trapped inside the thick human mucus so they can be laid flat and seen under the microscope.
- N-acetyl-L-cysteine (NALC), 0.5%: A powerful mucolytic agent that breaks disulfide bonds in mucus. It is specifically used to digest thick sputum specimens submitted for the detection of Pneumocystis jirovecii. Sodium citrate is added to the mixture to chemically stabilize the acetylcysteine.
- Dithiothreitol (Sputolysin), 0.0065 M: Another potent mucolytic agent used to heavily digest and prepare respiratory sputum specifically for the detection of Pneumocystis carinii / jirovecii.
- Potassium Hydroxide (KOH 10% - 20%): The absolute gold standard for direct fungal wet mounts of skin, hair, and nails.
- Mechanism: KOH strongly digests and dissolves the dense, proteinaceous keratin components of human host tissues. However, because fungal cell walls are made of highly resistant, tough chitin, they easily resist the alkali degradation. The human tissue melts away, leaving the fungal hyphae completely intact and beautifully visible!
B. Basic Mycology Wet Mounts
- Lactophenol Cotton Blue (LPCB): LPCB is universally paired with KOH because it significantly enhances the visibility of clear, transparent fungi.
- Aniline (Cotton) Blue: A dye that selectively and aggressively binds to the chitin in the fungal cell wall, staining the entire fungus a brilliant, deep blue.
- Phenol: Acts as a potent fungicidal agent, instantly killing the fungus to protect the lab technician.
- Lactic acid: Acts as a clearing agent and physically preserves delicate fungal reproductive structures (conidiophores).
- Glycerol: A viscous liquid that prevents the wet mount slide from drying out under the microscope heat.
- Permanent Mounts: The addition of 10% polyvinyl alcohol (LPCB PVA) to the stain acts as a hard plastic fixative, creating a permanent stained slide for preserving excellent slide culture preparations for teaching purposes.
IX. Specialized Staining Techniques
Because fungi are often transparent and hide deep within complex human tissues, they are completely invisible in standard H&E tissue preparations without highly specialized, targeted chemical dyes. Here is the full arsenal of mycology stains:
Used specifically for the rapid visualization of heavily encapsulated organisms in Cerebrospinal Fluid (CSF), namely Cryptococcus neoformans.
Mechanism: It is a Negative Stain. The massive, thick polysaccharide capsule of the yeast physically acts as a steric barrier, completely excluding the large, dark carbon ink particles. The entire background of the slide stains pitch black, while the yeast cell is outlined by a bright, clear, glowing halo representing the capsule.
Clinical Note: While historically classic, the CRAG test (Cryptococcal Antigen test) using lateral flow assays is now far more sensitive and specific for diagnosing Cryptococcal meningitis.
A non-specific, highly sensitive chemofluorescent fluorochrome dye that aggressively binds directly to B-1,3 and B-1,4 linked polysaccharides (specifically the cellulose and chitin forming the fungal cell walls).
KOH is added to melt away the human tissue debris. It requires a high-powered fluorescent microscope. The fungal elements will brilliantly fluoresce a glowing bluish-white or apple-green against a pitch-dark background when excited with UV or blue-violet radiation.
Specific Use: Pneumocystis jirovecii cysts appear round, uniform in size, with a highly characteristic, intense internal "double-parenthesis" like structure shining brightly.
Considered the ultimate, most sensitive histological tissue stain for fungi, including P. jirovecii. The chromic acid oxidizes fungal cell wall polysaccharides into aldehydes. The aldehydes then chemically reduce the silver nitrate in the stain into solid, black metallic silver. Result: All fungal elements are sharply and thickly delineated in stark black against a pale green or yellow tissue background.
Detects fungi in clinical tissue specimens (especially yeast cells and hyphae). Similar to GMS, periodic acid oxidizes the fungal wall sugars to aldehydes, which react with the Schiff reagent. Result: Most fungi will take up this stain, turning a brilliant, vibrant pink-magenta or bright purple. The background human tissue stains orange (if picric acid is used) or green (if light green is used).
These are extremely specific Mucopolysaccharide stains. They are exceptionally useful for differentiating Cryptococcus neoformans from other yeast species of similar size and shape in a tissue biopsy. The incredibly thick capsular material of Cryptococcus selectively absorbs the dye, staining a deep, vibrant rose to red (Mucicarmine) or striking blue (Alcian Blue), while other human tissue elements stain a neutral yellow.
Originally developed in histology to demonstrate melanin production in mammalian skin tissue. In mycology, it is used specifically to detect Dematiaceous (dark-pigmented) fungi and C. neoformans (which produces melanin via phenoloxidase). The fungal elements appear dark brown to brownish-black against a reddish cellular background.
Used specifically for the rapid detection of Pneumocystis jirovecii cysts directly from lung biopsies and Bronchoalveolar Lavage (BAL) fluid.
It selectively stains the cysts a reddish-blue or dark purple against a clean light blue background. The cysts may uniquely appear punched-in, collapsed, or crescent-shaped (like a deflated ping-pong ball). Important Limitation: The active trophozoite forms of the fungus are NOT discernible with this stain, only the thick-walled cysts.
- Gram Stain: Yeasts (like massive Candida cells) and Nocardia filaments typically stain strongly Gram-positive (dark crystal violet/purple). However, Cryptococcus and true filamentous mold fungi are very poorly stained and unreliable on a Gram stain.
- Modified ZN (Acid-Fast): Nocardia spp. are unique because they are weakly acid-fast positive, helping differentiate them from Actinomyces.
- Giemsa Stain: Used for blood, bone marrow, and tissue biopsies. Exceedingly useful for detecting intracellular Histoplasma capsulatum hiding inside human macrophages. They appear as small oval yeasts staining blue with a clear "hyaline halo" (representing poor cell wall staining, not a true capsule).
Ascomycetous fungi (like Saccharomyces) produce sexual ascospores under harsh culture conditions. They are stained using malachite green and safranin (similar to bacterial endospore stains). The tough ascospores take up the heat-driven malachite green, staining brilliant green, while the surrounding vegetative cellular parts stain pink. (The Kinyoun acid-fast stain protocol can also be utilized for this purpose).
X. Culture Media and Incubation Conditions
A. Media Selection
A highly specialized, wide variety of media is necessary in clinical mycology, and the exact selection strictly depends on the suspected anatomical specimen type and expected pathogenic profile.
- Sabouraud Dextrose Agar (SDA - Emmons modification): The universal, general-purpose isolation workhorse. Contains 2% dextrose, peptones, and is balanced to a pH of 6.9-7.0. It usually has added antibiotics to suppress swarming bacteria. (Often used antibiotic-free for sterile fluids).
- Sabouraud-Brain Heart Infusion (SAB-BHI): General purpose, but the addition of the highly nutritious sheep brain and beef heart infusion allows for the maximum, rapid recovery of extremely fastidious, hard-to-grow dimorphic fungi (like Histoplasma and Blastomyces).
- Inhibitory Mould Agar (IMA): Contains the broad-spectrum antibiotic Chloramphenicol (CAF) alongside gentamicin to heavily and aggressively inhibit bacterial overgrowth in highly contaminated specimens like sputum or feces.
- Mycobiotic Agar (Mycosel): Contains Chloramphenicol (CAF) and Cycloheximide.
- Physiology Expansion: Cycloheximide is a potent chemical that actively kills rapidly growing environmental saprophytic molds and many yeasts (including most Candida species and Cryptococcus). This makes Mycobiotic agar highly and exclusively selective for Dermatophytes (skin/nail ringworm fungi) and dimorphic pathogens, which possess a unique intrinsic resistance to cycloheximide.
- Acetate Ascospore Agar: A specialized starvation medium used purely for cultivating and inducing yeasts to sexually produce ascospores for identification (Potassium acetate is significantly better utilized by the yeast than sodium acetate).
- Aspergillus Differential Medium: Specifically differential for isolating Aspergillus flavus. The fungus uniquely utilizes the Ferric ion built into the medium for robust pigment production, imparting a distinct, bright yellow/yellow-green/olive color to the colony base.
B. Incubation Conditions & Safety Protocols
- Temperature: All routine fungal cultures should be incubated exactly at 30°C (which is the proven optimal growth threshold for most medically significant environmental fungi). If a 30°C incubator is utterly unavailable, use room temperature (near 25°C). Suspected dimorphic fungi are plated in duplicate (one at 25°C and one at 37°C) to prove they can transition to yeast.
- Duration: Routine mold incubation takes a mandated 4 weeks (fungi grow extremely slowly, and discharging a plate as "negative" too early can kill a patient!). However, 3 weeks may be deemed clinically adequate for most fast-growing clinical isolates (excluding slow-growing skin/hair/nail dermatophytes and dimorphic pathogens like Histoplasma which can take 6 weeks).
- Yeast Exceptions: Specimens screened primarily for fast-growing yeasts (e.g., simple oral thrush, candiduria, or vaginal swabs) only need to be incubated for an absolute maximum of 7 days.
- Observation Frequency: Examine culture plates at least every 2 to 3 days for the first two weeks, and weekly thereafter. Fungi can bloom rapidly once established.
- Strict Safety Protocol: All mold identification and plate manipulation MUST be executed entirely inside a Biological Safety Cabinet Class 2 (BSC2) equipped with massive HEPA filtration exhausts. Molds release literally millions of aerosolized, microscopic spores; opening an infected plate on an open laboratory bench will permanently contaminate the entire lab environment and ensure the technician inhales massive doses of pathogenic spores directly into their lungs!
Traditional fungal cultures take agonizingly long weeks to mature. Modern tertiary hospitals now rely on rapid molecular and proteomic methods to save dying septic patients:
- MALDI-TOF Mass Spectrometry: (Matrix-Assisted Laser Desorption/Ionization Time-of-Flight). A revolutionary technology that uses an intense laser to blast and vaporize a tiny speck of the fungal colony. The machine analyzes the time it takes the vaporized fungal ribosomal proteins to hit a detector, immediately identifying the exact species in minutes based on its unique, digitized protein "fingerprint".
- rRNA Sequencing: (Clinical Correction: Your slide notes 16S rRNA, but 16S is actually strictly used for Bacterial identification. For Fungi, modern advanced labs sequence the 18S rRNA or the Internal Transcribed Spacer (ITS) region of the fungal genome for perfect, DNA-level identification. Remember ITS for advanced clinical board exams!)
XI. Antifungal Drug Targets (High-Yield Pharmacology)
Because fungi are complex eukaryotes (just like human cells), the core problem in antifungal pharmacology is creating highly toxic drugs that aggressively kill the fungal cell without simultaneously killing the human patient's cells. To achieve this selective toxicity, we must specifically target the very few biochemical structures that fungi possess but humans entirely lack (namely Ergosterol pathways and the Glucan Cell Wall).
Class: Polyenes
- Drugs: Amphotericin B (the "Gold Standard" for severe systemic infections), Lipid Formulation AmB (Colloidal dispersion, liposomal structures to reduce toxicity), and Nystatin (Topical only, too toxic for IV).
- Mechanism: These large, complex drugs physically seek out and firmly bind directly to the pre-existing ergosterol integrated within the fungal cell membrane. Once bound, they aggregate to tear massive, literal pores (holes) straight through the membrane. Crucial intracellular ions (Potassium, Magnesium) instantly leak out, leading to rapid, explosive osmotic cell death (fungicidal).
Class: Azoles
- Drugs: Fluconazole, Ketoconazole, Itraconazole, Clotrimazole, Voriconazole, Ravuconazole, Posaconazole.
- Mechanism: They are enzyme assassins. They actively bind to and inhibit the crucial fungal cytochrome P450 enzyme known as lanosterol 14-alpha-demethylase, which is absolutely required to manufacture fresh ergosterol. Without ergosterol, the membrane cannot grow, and highly toxic methylated sterol precursors build up inside the cell, stunting growth and eventually killing the fungus (fungistatic).
Class: Echinocandins
- Drugs: Caspofungin, Micafungin, Anidulafungin.
- Mechanism: They aggressively inhibit the fungal enzyme Beta-1,3-glucan synthase. Without beta-glucans, the tough fungal cell wall cannot be constructed. The cell wall collapses, and the fungus rapidly bursts and dies from severe osmotic instability in the blood. (Clinically, this class is heavily referred to as the "Penicillin of fungi" because it specifically targets the rigid cell wall, making it incredibly safe for human organs!).
Class: Pyrimidine Analogs
- Drug: 5-Fluorocytosine (Flucytosine).
- Mechanism: It acts as a massive "Trojan Horse." The fungus actively transports the harmless-looking Flucytosine into its cell using a specific permease pump. Once inside, fungal enzymes rapidly convert it into 5-fluorouracil (5-FU), a highly toxic chemotherapy molecule that aggressively halts fungal DNA and RNA synthesis, crippling the cell. It is almost always given synergistically alongside Amphotericin B (Amphotericin tears holes in the membrane, allowing the Flucytosine to flood into the cell faster).
❓ Final Module Review Question: The "Ampho-Terrible" Toxicity
Case: A severely immunocompromised patient with a massive systemic fungal infection is placed on an IV drip of Amphotericin B. Within days, the patient begins to experience severe, life-threatening kidney toxicity (nephrotoxicity), which is a famously common and devastating side effect of this specific drug. Based entirely on the mechanism of action, why does Amphotericin B cause such extreme human toxicity, whereas Penicillin (a powerful antibacterial) does not?
Answer: Penicillin strictly targets peptidoglycan, a unique cell wall substance that is completely 100% absent in human cells, making Penicillin extremely safe with virtually zero organ toxicity. Amphotericin B, however, targets and binds to Ergosterol in the fungal cell membrane. While it strongly prefers binding to ergosterol, because ergosterol is chemically and structurally very similar to human Cholesterol, Amphotericin B makes mistakes. It accidentally binds to the abundant cholesterol found in human renal (kidney) tubular cell membranes, ripping open the human cells and causing severe, direct kidney necrosis and toxicity!
References & Clinical Reading
- Larone, D. H. (2002). Medically Important Fungi: A Guide to Identification (4th ed.). ASM Press.
- Kwon-Chung, K. J., & Bennett, J. E. (1992). Medical Mycology. Lea & Febiger.
- Clinical and Laboratory Standards Institute (CLSI). Principles of Fungal Culture and Identification.
- Supplemental high-yield pharmacological integrations and foundational taxonomy derived directly from University lecture notes and standard medical board physiology outlines.
Quick Quiz
Intro to Mycology Quiz
Microbiology - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
Intro to Mycology Quiz
Microbiology
Preparing questions...
Choose your answer and keep your streak alive.
Great effort.
Here is your quick performance summary.
Introduction to Mycology Read More »