

Cells and Tissues
BNS 111: Anatomy & Physiology
SEMESTER I - Cell and Tissues
Cell Theory
Alright, let's dive into the microscopic world that makes up our bodies, starting with the fundamental concept of theCell Theory. This theory is one of the cornerstones of biology and medicine, giving us the basic understanding of life. It essentially has three main parts, like three key rules about cells:
- All living organisms are made up of one or more cells.This means whether it's a tiny bacterium, a plant, or a human being, the basic unit of structure is the cell. Some organisms are single-celled (like amoeba), while complex organisms like us are made of trillions of cells working together.
- The cell is the basic unit of structure and organization in organisms.This means that the cell is the smallest level at which life functions can be carried out. Just like a single brick is the basic unit of a wall, a cell is the basic unit of a tissue, an organ, and ultimately, an organism. All the complex processes of life happen within cells.
- Cells arise from pre-existing cells.This means cells don't just appear out of nowhere. New cells are produced through cell division (like mitosis or meiosis) from cells that already exist. This explains growth, repair, and reproduction in living things.

Cell Structure and Organelles
Now that we know cells are the basic units, let's peek inside and see what they are made of! Think of a cell like a tiny factory, with different departments and machines (calledorganelles) each doing a specific job to keep the factory running. Human cells, being eukaryotic (having a true nucleus), have several key parts:
The cell is generally divided into two main regions:
- Plasma Membrane (Cell Membrane):This is the outer boundary of the cell, like the factory wall. It's a flexible but sturdy barrier that controls what enters and leaves the cell. It's made mainly of a double layer of lipids (fats) with proteins embedded in it. These proteins act like gates, channels, or pumps, allowing specific substances to pass through. The plasma membrane is crucial for maintaining the cell's internal environment and communicating with other cells.
- Cytoplasm:This is everything inside the plasma membrane but outside the nucleus. It's like the factory floor and all the machinery on it. The cytoplasm consists of two main parts:
- Cytosol:This is the jelly-like fluid portion of the cytoplasm. It's mostly water, but contains dissolved substances like salts, sugars, proteins, and waste products. Many chemical reactions of the cell happen here.
- Organelles:These are the "little organs" or specialized structures suspended in the cytosol, each with its own shape and specific function. They are like the different machines and departments in our factory.
Let's look at the key organelles found in a typical human cell:
- Nucleus:This is the "control center" or "brain" of the cell, usually the largest organelle. It contains the cell's genetic material (DNA) organized intochromosomes. The nucleus controls the cell's activities by directing protein synthesis. It is surrounded by a double membrane called thenuclear envelope, which has pores allowing materials to pass in and out.
- Mitochondria:These are the "powerhouses" of the cell. They are responsible for generating most of the cell's supply ofATP(adenosine triphosphate), which is the cell's main energy currency, through a process calledcellular respiration. Cells that need a lot of energy, like muscle cells, have many mitochondria.
- Endoplasmic Reticulum (ER):This is a network of interconnected membranes extending throughout the cytoplasm. It's involved in producing, processing, and transporting proteins and lipids. There are two types:
- Rough ER (RER):Studded with ribosomes, it's involved in the synthesis and modification of proteins that are destined for secretion or insertion into membranes.
- Smooth ER (SER):Lacks ribosomes and is involved in synthesizing lipids (like steroids), detoxifying harmful substances (especially in liver cells), and storing calcium ions (especially in muscle cells).
- Ribosomes:These are tiny structures responsible forprotein synthesis. They can be free in the cytoplasm (making proteins used within the cell) or attached to the RER (making proteins for export or membranes). They are like the assembly lines for building proteins.
- Golgi Apparatus (Golgi Complex or Golgi Body):This is like the cell's "packaging and shipping center." It modifies, sorts, and packages proteins and lipids received from the ER into vesicles for transport to their final destinations, either inside or outside the cell.
- Lysosomes:These are like the cell's "recycling centers" or "garbage disposal." They contain powerful digestive enzymes that break down waste materials, cellular debris, and foreign invaders like bacteria.
- Peroxisomes:These are small vesicles that contain enzymes that help detoxify harmful substances (like alcohol) and break down fatty acids. They produce hydrogen peroxide as a byproduct, but also contain enzymes to break down hydrogen peroxide into water and oxygen, protecting the cell.
- Cytoskeleton:This is a network of protein filaments and tubules that extends throughout the cytoplasm. It's like the cell's "skeleton" and "road system," providing structural support, maintaining cell shape, and allowing for movement of organelles and the cell itself (in some cases). It includesmicrofilaments,intermediate filaments, andmicrotubules.
- Centrosomes and Centrioles:Located near the nucleus, the centrosome is the main organizing center for microtubules. Within the centrosome are two cylindrical structures called centrioles, which are important for cell division, forming the spindle fibers that separate chromosomes.
- Cilia and Flagella:These are whip-like or hair-like projections extending from the surface of some cells.Ciliaare usually short and numerous, and their coordinated beating moves substances along the cell surface (e.g., in the airways to move mucus).Flagellaare usually long and single, and their movement propels the cell itself (e.g., the tail of a sperm cell).

Cell Functions and Functional Specialization
Even though all cells share basic structures and carry out essential life processes, different types of cells in our body are highly specialized to perform specific functions. Thisfunctional specializationis what allows us to have complex tissues, organs, and organ systems. Think of the different workers in our factory – some are builders, some are packers, some are security guards, each with a unique role.
Some fundamental functions that most cells perform to stay alive and maintain the organism include:
- Metabolism:The sum of all chemical processes that occur in the body. Cells carry out metabolic reactions to obtain energy (like cellular respiration in mitochondria) and to synthesize or break down molecules needed for their structure and function.
- Responsiveness:The ability to detect and respond to changes in their environment. This can be sensing chemical signals, physical touch, or electrical impulses. For example, nerve cells respond to stimuli by generating electrical signals.
- Movement:Can refer to movement of the entire cell (like white blood cells moving to an infection site) or movement of structures within the cell (like organelles being transported) or movement produced by the cell (like muscle cells contracting).
- Growth:An increase in cell size or an increase in the number of cells through cell division.
- Differentiation:The process by which a less specialized cell becomes a more specialized cell type. This is how a single fertilized egg develops into all the different cell types in the body (nerve cells, muscle cells, skin cells, etc.).
- Reproduction:Can refer to the formation of new cells for growth, repair, or replacement (through mitosis) or the production of a new organism (through meiosis and fertilization).
Now, let's look at how different cells are specialized for particular jobs, often by having more of certain organelles or unique structures:
- Muscle Cells:Specialized for contraction. They are packed with protein filaments (actin and myosin) that slide past each other to shorten the cell, producing force and movement. They also have abundant mitochondria for energy and specialized smooth ER (sarcoplasmic reticulum) for calcium storage, which is crucial for contraction.
- Nerve Cells (Neurons):Specialized for transmitting electrical and chemical signals over long distances. They have long extensions called axons and dendrites. Their plasma membrane is excitable, meaning it can generate and conduct electrical impulses. They have many ribosomes and ER for synthesizing neurotransmitters.
- Red Blood Cells:Specialized for transporting oxygen. They lack a nucleus and most organelles (like mitochondria) in their mature state, which maximizes the space available for hemoglobin, the protein that binds oxygen. Their biconcave shape also increases surface area for gas exchange and allows them to squeeze through narrow blood vessels.
- Epithelial Cells:Specialized for covering surfaces, lining cavities, protection, absorption, and secretion. They are often tightly packed together and may have specialized structures like microvilli (to increase surface area for absorption, like in the intestines) or cilia (to move substances, like in the airways).
- Gland Cells:Specialized for secretion (producing and releasing substances like hormones, enzymes, or mucus). They have abundant ribosomes, ER, and Golgi apparatus to synthesize, process, and package their secretory products into vesicles.
- Bone Cells (Osteocytes):Specialized for maintaining bone tissue. They are embedded in a hard extracellular matrix they helped produce, providing structural support to the body.
- White Blood Cells (e.g., Macrophages):Part of the immune system, specialized for defense. Some can move actively (amoeboid movement) and engulf foreign particles or debris (phagocytosis), acting like the body's cleanup crew and security. They have abundant lysosomes to break down ingested material.

Cell Cycle Regulation and Disorders
Cells don't live forever. For growth, repair, and replacement, cells need to divide. TheCell Cycleis the ordered sequence of events that a cell goes through from the time it is formed until it divides into two new daughter cells. It's a tightly regulated process, like a carefully planned schedule. The main phases of the cell cycle are:
- Interphase:This is the longest phase where the cell grows, copies its DNA, and prepares for division. It includes three sub-phases:
- G1 Phase (First Gap):Cell grows and carries out normal metabolic functions.
- S Phase (Synthesis):DNA is replicated (copied).
- G2 Phase (Second Gap):Cell continues to grow and synthesizes proteins needed for division.
- Mitotic (M) Phase:This is when the cell actually divides. It includes:
- Mitosis:The nucleus divides, and the copied chromosomes are separated into two identical sets. Mitosis itself has stages: Prophase, Metaphase, Anaphase, Telophase.
- Cytokinesis:The cytoplasm divides, splitting the original cell into two separate daughter cells.
The cell cycle is controlled by a complex system of internal and external signals and checkpoints, like quality control points in the factory.Cell cycle regulationensures that cells divide only when necessary, that DNA replication is completed accurately, and that chromosomes are correctly distributed to the daughter cells. Key regulators include proteins calledcyclinsand enzymes calledcyclin-dependent kinases (CDKs). There are also checkpoints (e.g., G1 checkpoint, G2 checkpoint, M checkpoint) that pause the cycle if something is wrong, allowing time for repair or signaling the cell to undergo programmed cell death (apoptosis) if the damage is too severe.
Disorders of Cell Cycle Regulation:What happens when this careful regulation goes wrong? This is where we see serious problems, most notablycancer. Cancer is fundamentally a disease of uncontrolled cell division. It occurs when genetic mutations damage the genes that regulate the cell cycle (like genes for cyclins, CDKs, or checkpoint proteins). Damaged cells ignore the checkpoints, divide continuously without proper signals, and can invade other tissues (metastasis). Other disorders can involve too little cell division, leading to tissue degeneration or poor wound healing. Understanding cell cycle regulation is vital for developing treatments for cancer and other related conditions.



Epithelial Tissue and Glands
Epithelial tissue, also calledepithelium(plural: epithelia), is one of the four basic tissue types in the body. Think of it as the "covering" or "lining" tissue. It forms sheets of cells that cover body surfaces, line body cavities and hollow organs, and are the main tissue in glands.
Key characteristics of epithelial tissue:
- Polarity:Epithelial cells have an apical surface (free surface, exposed to the body exterior or the cavity of an internal organ) and a basal surface (attached to underlying tissue). The apical surface often has specialized structures like microvilli or cilia.
- Specialized Contacts:Epithelial cells fit closely together to form continuous sheets, bound by specialized junctions like tight junctions (prevent leakage) and desmosomes (provide strong adhesion). This creates a barrier function.
- Supported by Connective Tissue:The basal surface is attached to a thin layer of connective tissue by abasement membrane(also called the basal lamina). This membrane provides structural support and acts as a selective filter.
- Avascular but Innervated:Epithelial tissue itself does not have blood vessels (avascular), so it receives nutrients by diffusion from the underlying connective tissue. However, it does have nerve endings (innervated).
- Regeneration:Epithelial tissue has a high regenerative capacity, meaning it can reproduce rapidly to replace damaged or lost cells (important for tissues exposed to friction or damage, like the skin).
Epithelial tissues are classified based on two main criteria: thenumber of cell layersand theshape of the cells.
Based on the number of layers:
- Simple Epithelium:Consists of a single layer of cells. These are typically found where absorption, secretion, and filtration occur, as the single layer allows for easy passage of substances.
- Stratified Epithelium:Consists of two or more layers of cells. These are found in areas subject to wear and tear, where protection is important (e.g., skin surface). The layers provide durability.
- Pseudostratified Epithelium:Appears to be stratified because the cell nuclei are at different levels, but it is actually a single layer of cells of varying heights. Often ciliated, found in the respiratory tract.
Based on the shape of the cells (named according to the shape of the cells in the apical layer for stratified epithelia):
- Squamous Cells:Flat, scale-like cells.
- Cuboidal Cells:Cube-shaped cells, about as tall as they are wide.
- Columnar Cells:Tall, column-shaped cells, taller than they are wide.
Combining the number of layers and cell shape gives us the main types of epithelial tissue:
- Simple Squamous Epithelium:Single layer of flat cells. Found in air sacs of lungs, lining of blood vessels. Allows for rapid diffusion and filtration.
- Simple Cuboidal Epithelium:Single layer of cube-shaped cells. Found in kidney tubules, small glands. Involved in secretion and absorption.
- Simple Columnar Epithelium:Single layer of tall cells. Found in the lining of the digestive tract (often with microvilli for absorption) and gallbladder. Involved in absorption and secretion (including mucus).
- Pseudostratified Columnar Epithelium:Single layer, but appears layered; cells are columnar. Found in the trachea and upper respiratory tract (usually ciliated, moving mucus). Involved in secretion and movement of mucus.
- Stratified Squamous Epithelium:Multiple layers, apical cells are flat. Found in the skin surface (keratinized, tough) and lining of the mouth, esophagus, vagina (non-keratinized, moist). Provides protection against abrasion.
- Stratified Cuboidal Epithelium:Multiple layers, apical cells are cube-shaped. Rare, found in ducts of some large glands (e.g., sweat glands).
- Stratified Columnar Epithelium:Multiple layers, apical cells are columnar. Very rare, found in small amounts in the pharynx, male urethra, and some gland ducts.
- Transitional Epithelium:Modified stratified epithelium where the apical cells change shape depending on stretching. Found in the lining of the urinary bladder, ureters, and part of the urethra. Allows these organs to stretch and recoil.
Main functions of epithelial tissue:
- Protection:Forms barriers against physical injury, chemicals, bacteria, and water loss (e.g., skin epidermis).
- Absorption:Takes in substances from a free surface (e.g., nutrients in the digestive tract lining).
- Secretion:Produces and releases substances like mucus, hormones, enzymes, and sweat (done by glandular epithelium).
- Filtration:Allows passage of small molecules while blocking larger ones (e.g., in the kidneys and capillaries).
- Excretion:Removes waste products from the body (e.g., in sweat).
- Sensory Reception:Contains nerve endings for touch, pain, temperature, etc. (e.g., in the skin).
Disorders affecting Epithelial Tissue:Many common diseases involve epithelial tissue. Since they form coverings and linings and regenerate quickly, they are often sites of injury and uncontrolled growth.
- Carcinomas:The most common type of cancer, arising from epithelial tissue. Examples include skin cancer, lung cancer, breast cancer, colon cancer. Because epithelial cells divide rapidly, they are prone to mutations leading to uncontrolled growth.
- Inflammation:Epithelial linings are often the first point of contact for pathogens, leading to inflammation (e.g., bronchitis - inflammation of bronchial lining).
- Genetic Disorders:Some genetic conditions affect epithelial cell function, like Cystic Fibrosis, which affects epithelial cells in the lungs, pancreas, and other organs, leading to thick mucus secretions.
- Physical Damage:Abrasions, burns, and cuts damage epithelial tissue (skin).
Glands:Glands are organs or tissues that produce and secrete specific substances. They are primarily made up of epithelial tissue. Glands can be unicellular (single-celled) or multicellular (made of many cells). They are classified based on where they secrete their products:
- Endocrine Glands:These are "ductless" glands. They secrete hormones directly into the bloodstream or interstitial fluid, which then travel to target cells elsewhere in the body to regulate various functions. Examples include the pituitary gland, thyroid gland, adrenal glands, pancreas (parts of it), ovaries, and testes. Hormones are chemical messengers.
- Exocrine Glands:These glands secrete their products into ducts, which then carry the secretions to a body surface (either external, like the skin) or into a body cavity (like the digestive tract or airways). Exocrine secretions include mucus, sweat, saliva, tears, digestive enzymes, and oil. Examples include sweat glands, salivary glands, mammary glands, liver (secretes bile into ducts), and the pancreas (secretes digestive enzymes into ducts).
Classification of Exocrine Glands based on structure:
- Unicellular:Simple, single-celled glands scattered within an epithelial sheet (e.g., goblet cells that secrete mucus in the lining of the intestines and respiratory tract).
- Multicellular:Composed of many cells forming a more complex structure with a duct and a secretory unit (acinus or tubule). They can be simple (single unbranched duct) or compound (branched duct), and tubular (tube-shaped secretory part), alveolar/acinar (sac-like secretory part), or tubuloalveolar.
Classification of Exocrine Glands based on mode of secretion:
- Merocrine Glands:Secrete their products by exocytosis (vesicles releasing contents outside the cell). The cell is not damaged. Most common type (e.g., sweat glands, salivary glands, pancreas).
- Apocrine Glands:Secrete by budding off portions of the cell membrane containing the product. Part of the cell apex is pinched off (e.g., mammary glands secrete fat droplets).
- Holocrine Glands:Secrete by accumulating products within the cell until it ruptures and dies, releasing its contents. The entire cell becomes the secretion (e.g., sebaceous glands that secrete oil onto hair and skin).
Common Disorders of Glands:
- Endocrine Disorders:Result from too much or too little hormone secretion (e.g., Diabetes Mellitus - problem with insulin from the pancreas; Hypothyroidism - too little thyroid hormone).
- Exocrine Disorders:Can involve blockage of ducts (e.g., gallstones blocking bile ducts from the liver/gallbladder, kidney stones blocking ureters from the kidney), infection of glands (e.g., mastitis - infection of mammary gland), or over/undersecretion (e.g., excessive sweating, dry mouth due to salivary gland problems).
- Cancers:Glandular epithelial tissue (adenocarcinoma) is a common site for cancer development.


Connective Tissue
Connective tissue is the most abundant and widely distributed of the primary tissues in the body. As the name suggests, its main function is toconnect, support, bind, and separate other tissues. Think of it as the body's "glue," packaging material, and structural support system. Unlike epithelial tissue, which is mainly cells, connective tissue is characterized by having a lot ofextracellular matrix– the stuff outside the cells.
Key characteristics of connective tissue:
- Common Origin:All connective tissues arise frommesenchyme, an embryonic tissue.
- Varying Degrees of Vascularity:Connective tissues have different amounts of blood supply. Some, like cartilage, are avascular (no blood vessels). Others, like bone, are well vascularized. Dense connective tissue (like ligaments) has poor vascularity.
- Extracellular Matrix:This is the non-living material found between the cells, and it's what gives connective tissue its unique properties. The matrix is made up of aground substance(an unstructured gel-like material that fills the space between cells) andfibers(protein fibers that provide support – collagen, elastic, reticular). The type and amount of ground substance and fibers vary greatly depending on the specific type of connective tissue, determining its strength, elasticity, or rigidity.
- Cells:Connective tissues have various cell types. Immature cells (ending in "-blast", e.g., fibroblasts, chondroblasts, osteoblasts) are actively secreting the matrix. Mature cells (ending in "-cyte", e.g., fibroblasts, chondrocytes, osteocytes) maintain the matrix. Other cells like fat cells (adipocytes), mast cells (involved in inflammation), and defense cells (macrophages, plasma cells) can also be found in some connective tissues.
Connective tissue is a broad category with several major classes and subclasses, each specialized for specific functions. Based on your outline, we'll focus on:
- Connective Tissue Proper (Fibrous Tissue):This is the most widespread type, with varying amounts of fibers and ground substance.
- Cartilage:A flexible but tough supporting tissue.
- Bone (Osseous Tissue):A hard, rigid supporting tissue.
- Blood:A fluid connective tissue involved in transport.
Connective Tissue Proper (Fibrous Tissue)
Connective tissue proper has two broad categories based on the density and arrangement of its fibers: Loose Connective Tissue and Dense Connective Tissue. The primary cell type in connective tissue proper is thefibroblast(or fibrocyte in its mature form), which produces the fibers and ground substance.
Loose Connective Tissue:In this type, the fibers are loosely arranged, leaving a lot of space filled with ground substance. This provides cushioning and support for other tissues and organs. It's well vascularized.
- Areolar Connective Tissue:The most common loose connective tissue. It has a gel-like matrix with all three fiber types (collagen, elastic, reticular) and various cell types (fibroblasts, macrophages, mast cells, some white blood cells). It acts as a packing material between organs, surrounds blood vessels and nerves, and underlies epithelia, providing support and holding tissue fluid. It's involved in inflammation and immunity.
- Adipose Tissue (Fat):Primarily made up ofadipocytes(fat cells) which store triglycerides (fats). It has a sparse matrix. Functions include energy storage, insulation against heat loss, and cushioning/protection of organs (e.g., around kidneys and eyeballs).
- Reticular Connective Tissue:Contains delicate networks of reticular fibers in a loose ground substance. Forms the stroma (framework) of lymphoid organs like the spleen, lymph nodes, and bone marrow, supporting blood cells.
Dense Connective Tissue:In this type, the fibers (mainly collagen) are packed more densely, providing greater strength and resistance to tension. It's less vascularized than loose connective tissue.
- Dense Regular Connective Tissue:Collagen fibers are arranged in parallel bundles, running in the same direction. This provides great tensile strength in one direction. Found intendons(connect muscle to bone) andligaments(connect bone to bone).
- Dense Irregular Connective Tissue:Collagen fibers are thicker and arranged irregularly, running in various directions. This provides tensile strength in multiple directions. Found in the dermis of the skin, fibrous capsules of organs and joints, and the perichondrium and periosteum (coverings of cartilage and bone).
- Elastic Connective Tissue:Contains a high proportion of elastic fibers, allowing the tissue to stretch and recoil. Found in the walls of large arteries, some ligaments (e.g., ligaments connecting vertebrae), and the bronchial tubes.
Disorders of Fibrous Connective Tissue:Problems with connective tissue proper can lead to various conditions:
- Injuries:Sprains (ligaments stretched/torn) and strains (tendons/muscles stretched/torn) are common injuries involving dense regular connective tissue.
- Inflammation:Tendinitis (inflammation of a tendon) or fasciitis (inflammation of fascia, a type of dense irregular connective tissue).
- Adipose Tissue Disorders:Obesity (excessive fat storage), or lipedema (abnormal fat distribution).
- Genetic Disorders:Some genetic conditions affect collagen or elastic fiber synthesis, leading to disorders like Ehlers-Danlos syndromes (affecting connective tissue strength and elasticity throughout the body) or Marfan syndrome (affecting elastic tissue, particularly in the cardiovascular system and skeleton).
Cartilage
Cartilageis a flexible but tough supporting connective tissue. It's found in many areas of the body, including joints, the nose, ears, trachea, and intervertebral discs. Unlike most connective tissues, mature cartilage isavascular(no blood vessels) and lacks nerve fibers, which means it heals very slowly if damaged.
Key features of cartilage:
- Cells:The primary cells arechondroblasts(immature, produce matrix) andchondrocytes(mature, maintain matrix). Chondrocytes are located in small cavities within the matrix calledlacunae.
- Matrix:Firm, gel-like ground substance containing varying amounts of collagen and/or elastic fibers. This matrix is what gives cartilage its resilient and supportive properties.
- Perichondrium:A layer of dense irregular connective tissue that surrounds most cartilage (except articular cartilage in joints). It contains blood vessels that supply nutrients to the cartilage cells by diffusion, and it's involved in cartilage growth and repair.
There are three types of cartilage, differing in the composition of their matrix and fibers, which affects their properties and location:
- Hyaline Cartilage:The most abundant type. It has a smooth, glassy appearance with fine collagen fibers. Provides support and flexibility, reduces friction. Found at the ends of long bones in joints (articular cartilage), in the nose, trachea, larynx, and rib cage (costal cartilage).
- Elastic Cartilage:Similar to hyaline cartilage but contains abundant elastic fibers. This makes it more flexible and able to tolerate repeated bending. Found in the external ear and the epiglottis (flap of cartilage in the throat).
- Fibrocartilage:The strongest type of cartilage, containing thick bundles of collagen fibers and less ground substance. It's compressible and resists tension, acting as a shock absorber. Found in structures subjected to heavy pressure, such as the intervertebral discs (between vertebrae), the menisci of the knee, and the pubic symphysis (joint between pelvic bones).
Disorders of Cartilage:
- Osteoarthritis:A very common degenerative joint disease where the articular cartilage at the ends of bones wears away, leading to pain, stiffness, and reduced movement.
- Cartilage Tears:Can occur in fibrocartilage structures like the menisci of the knee due to injury. Healing is slow due to avascularity.
- Inflammation:Chondritis is inflammation of cartilage.
Bone (Osseous Tissue)
Bone, or osseous tissue, is a hard, dense connective tissue that forms the skeletal framework of the body. It's one of the hardest tissues in the body due to the presence of inorganic calcium salts in its matrix. Bone is well vascularized and innervated, meaning it has a good blood supply and nerve endings, which is why bone fractures hurt and heal (though healing time varies).
Key features of bone:
- Cells:Bone tissue contains several cell types involved in its formation, maintenance, and breakdown:
- Osteoblasts:Bone-forming cells that secrete the organic part of the bone matrix (collagen fibers and ground substance).
- Osteocytes:Mature bone cells located in lacunae within the matrix. They are connected to each other and the blood supply through tiny channels calledcanaliculi. Osteocytes maintain the bone tissue.
- Osteoclasts:Large multinucleated cells that break down (resorb) bone tissue. This process is important for bone remodeling, growth, and repair, and for releasing calcium into the blood.
- Matrix:Bone matrix is unique because it ismineralized. It has both organic components (mainly collagen fibers, which provide flexibility and tensile strength) and inorganic components (mainly calcium phosphate salts, calledhydroxyapatite, which provide hardness and compressional strength). The combination makes bone strong and resistant to both pulling and pushing forces.
- Periosteum:A tough, fibrous membrane that covers the outer surface of most bones. It contains blood vessels, nerves, and bone-forming cells (osteoblasts), playing a crucial role in bone nourishment, growth in thickness, and repair.
- Endosteum:A delicate membrane lining the internal surfaces of bone, including the cavities within spongy bone and the canals within compact bone. It also contains osteoblasts and osteoclasts.
There are two main types of bone tissue found in most bones:
- Compact Bone:Dense, solid bone tissue that forms the outer layer of all bones and the shaft (diaphysis) of long bones. Its structural unit is theosteon (Haversian system)– concentric rings of bone matrix (lamellae) around a central canal containing blood vessels and nerves. This structure provides strength and resistance to stress.
- Spongy Bone (Trabecular Bone):Located inside compact bone, especially at the ends (epiphyses) of long bones and in flat bones. It consists of a network of bony struts and plates calledtrabeculaewith spaces in between. These spaces are often filled withred bone marrow, where blood cells are produced (hematopoiesis). Spongy bone is lighter than compact bone and helps bones resist stress from different directions.
Functions of Bone:
- Support:Provides a framework for the body and supports soft tissues.
- Protection:Protects vital organs (e.g., skull protects the brain, rib cage protects heart and lungs).
- Movement:Serves as attachment points for muscles, acting as levers for movement at joints.
- Mineral Storage:Stores calcium and phosphate, releasing them into the bloodstream when needed to maintain blood mineral levels (crucial for nerve and muscle function).
- Blood Cell Formation (Hematopoiesis):Occurs in the red bone marrow found within the spaces of spongy bone.
- Triglyceride (Fat) Storage:Yellow bone marrow, found in the medullary cavity of long bones, stores fat.
Disorders of Bone Tissue:
- Fractures:Breaks in bone tissue, common due to trauma. Bone's good blood supply allows it to heal, but the process takes time.
- Osteoporosis:A condition where bone resorption (breakdown) outpaces bone formation, leading to decreased bone density and increased risk of fractures, especially in older adults.
- Osteomalacia/Rickets:Softening of bones due to insufficient mineralization, often caused by vitamin D or calcium deficiency. Rickets occurs in children, osteomalacia in adults.
- Osteomyelitis:Inflammation of bone tissue, often caused by infection.
- Bone Cancers:Primary bone cancers (like osteosarcoma) or metastatic cancers that spread to bone.
Blood
Bloodis considered a connective tissue because it originates from mesenchyme and consists of cells suspended in an extensive fluid matrix calledplasma. Unlike other connective tissues, the fibers in blood are soluble protein molecules visible only during blood clotting. Blood is vital for transportation and maintaining homeostasis throughout the body.
Key components of blood:
- Plasma:The fluid extracellular matrix, making up about 55% of blood volume. It's mostly water (about 90%), but contains a vast array of dissolved substances, including plasma proteins (like albumin, globulins, fibrinogen), hormones, nutrients (glucose, amino acids), electrolytes (ions like sodium, potassium), respiratory gases (oxygen, carbon dioxide), and waste products. Plasma transports these substances throughout the body.
- Formed Elements:The cellular and cell fragment components suspended in plasma, making up about 45% of blood volume. They are produced in the red bone marrow. The main types are:
- Erythrocytes (Red Blood Cells - RBCs):The most numerous formed elements. Small, biconcave discs that lack a nucleus and most organelles in mammals. They are specialized for transporting oxygen from the lungs to the tissues and a small amount of carbon dioxide from the tissues to the lungs, thanks to the proteinhemoglobin.
- Leukocytes (White Blood Cells - WBCs):Part of the immune system, involved in defending the body against infection and disease. They are complete cells with nuclei and organelles. There are different types of WBCs (neutrophils, lymphocytes, monocytes, eosinophils, basophils), each with specific roles in immunity. They can leave the bloodstream and enter tissues to fight infection.
- Thrombocytes (Platelets):Not true cells, but small, irregular-shaped fragments of larger cells called megakaryocytes found in bone marrow. They are essential forblood clotting (hemostasis), plugging damaged blood vessels and releasing factors that promote clotting.
Functions of Blood:
- Transportation:Transports oxygen from lungs to tissues, carbon dioxide from tissues to lungs, nutrients from the digestive tract to cells, hormones from endocrine glands to target organs, metabolic wastes from cells to kidneys and liver for excretion, and heat throughout the body.
- Regulation:Helps maintain body temperature (by distributing heat), maintains normal pH in body tissues (using buffer systems), and maintains adequate fluid volume in the circulatory system.
- Protection:Prevents blood loss through clotting (hemostasis) and prevents infection using antibodies, complement proteins, and white blood cells.
Disorders of Blood:Problems with blood components or function are very common:
- Anemia:A condition characterized by a reduced number of red blood cells or insufficient hemoglobin, leading to decreased oxygen-carrying capacity (e.g., iron-deficiency anemia, sickle cell anemia).
- Leukemia:Cancers of the white blood cells, leading to an overproduction of abnormal or immature white blood cells that don't function properly.
- Clotting Disorders:Conditions affecting the blood's ability to clot, either excessively (e.g., thrombosis, leading to blood clots) or insufficiently (e.g., hemophilia, excessive bleeding). Problems with platelets or clotting factors.
- Infections:Many infections are transported by blood, and white blood cell counts are a key indicator of infection. Sepsis is a life-threatening condition caused by the body's overwhelming response to an infection in the bloodstream.
Muscle Tissue (Propulsion Tissue)
Muscle tissueis specialized tissue that is responsible for movement. It does this by contracting, which means its cells can shorten and generate force. This force is used for body movements (like walking or lifting), moving substances within the body (like blood, food, or urine), and generating heat. Muscle tissue is often referred to as "propulsion tissue" because of its role in moving things.
Key characteristics that all muscle tissues share:
- Excitability (Responsiveness):The ability to receive and respond to stimuli (like nerve signals or hormones) by changing its electrical state and contracting.
- Contractility:The ability to shorten forcibly when stimulated. This is the defining property of muscle tissue.
- Extensibility:The ability to be stretched or extended. Muscles can be stretched beyond their resting length.
- Elasticity:The ability of a muscle cell to recoil and resume its resting length after being stretched.
There are three main types of muscle tissue in the body, classified based on their structure, location, and how they are controlled:
- Skeletal Muscle Tissue:
- Structure:Made up of long, cylindrical cells calledmuscle fibers. These fibers are multinucleated (have many nuclei) and appearstriated(have visible bands or stripes) under a microscope due to the arrangement of the contractile proteins (actin and myosin).
- Control:Voluntarycontrol, meaning we consciously control its contraction (e.g., moving your arm or leg).
- Distribution:Primarily attached to bones (via tendons), forming the muscles that move the skeleton. Also found in some areas like the diaphragm and the external anal sphincter.
- Functions:Body movement, maintaining posture, stabilizing joints, and generating heat.
- Regeneration:Has limited regenerative capacity. Damage is often repaired by fibrosis (formation of scar tissue).
- Smooth Muscle Tissue:
- Structure:Made up of spindle-shaped cells (tapered at both ends) with a single central nucleus. It isnon-striated, meaning it does not have the visible banding seen in skeletal or cardiac muscle.
- Control:Involuntarycontrol, meaning we do not consciously control its contraction. It is regulated by the autonomic nervous system, hormones, and local factors.
- Distribution:Found in the walls of hollow internal organs (viscera) like the stomach, intestines, bladder, uterus, blood vessels, airways, and arrector pili muscles in the skin.
- Functions:Propels substances through internal passageways (peristalsis in the digestive tract), regulates blood flow (by constricting/dilating blood vessels), moves substances through airways, empties the bladder and uterus.
- Regeneration:Has a moderate capacity for regeneration.
- Cardiac Muscle Tissue:
- Structure:Found only in the wall of the heart. Made up of branched cells that are connected to each other by specialized junctions calledintercalated discs. These discs allow electrical signals to pass rapidly from one cell to another, enabling the heart to contract as a coordinated unit. Cardiac muscle cells are usually uninucleated (one nucleus, sometimes two) and arestriated.
- Control:Involuntarycontrol. The heart has its own pacemaker cells that initiate contractions, but the rate and force can be influenced by the autonomic nervous system and hormones.
- Distribution:Exclusively found in the wall of the heart (myocardium).
- Functions:Propels blood throughout the body as the heart contracts.
- Regeneration:Has very limited regenerative capacity. Damage (like from a heart attack) is primarily repaired by scar tissue formation.
Disorders of Muscle Tissue:
- Muscle Strains/Tears:Common injuries, especially in skeletal muscle, where muscle fibers are overstretched or torn.
- Muscle Spasms/Cramps:Involuntary, painful contractions of muscles.
- Muscular Dystrophy:A group of genetic diseases that cause progressive weakness and degeneration of skeletal muscles.
- Myasthenia Gravis:An autoimmune disorder that affects the neuromuscular junction, leading to skeletal muscle weakness and fatigue.
- Cardiomyopathy:Diseases of the heart muscle, affecting its ability to pump blood effectively.
- Smooth Muscle Disorders:Can affect the function of organs containing smooth muscle, e.g., asthma (constriction of smooth muscle in airways), Irritable Bowel Syndrome (abnormal smooth muscle contraction in the intestines).
Nervous Tissue
Nervous tissueis the main tissue that makes up the nervous system – your body's control and communication network. It's responsible for receiving stimuli, processing information, and transmitting signals to other parts of the body to coordinate actions and responses. Think of it as the body's electrical wiring and processing unit.
Nervous tissue is composed of two main types of cells: highly specialized nerve cells called neurons, and several types of supporting cells collectively called neuroglia (or glial cells).
Structural Features of Neurons and Neuroglial Cells
Neurons (Nerve Cells):These are the excitable cells of the nervous system that are specialized for transmitting information via electrical and chemical signals. They are the functional units of the nervous system. While neurons vary in shape and size, they generally have the following structural components:
- Cell Body (Soma):This is the central part of the neuron containing the nucleus and most of the cell's organelles (like abundant ribosomes, Rough ER, and Golgi apparatus, reflecting high protein synthesis for neurotransmitters). The cell body is the metabolic center of the neuron.
- Dendrites:These are typically short, branched extensions that extend from the cell body. They act like antennae, receiving signals (neurotransmitters) from other neurons and transmitting these signals *towards* the cell body. A neuron usually has many dendrites to receive input from multiple sources.
- Axon:This is a single, typically long projection that extends from the cell body. The axon transmits electrical signals (action potentials) *away* from the cell body towards other neurons, muscles, or glands. Axons can be very long, extending up to a meter in length (e.g., from the spinal cord to the muscles in your foot).
- Axon Hillock:The cone-shaped region where the axon arises from the cell body. This is typically where the action potential is generated.
- Axon Terminals (Synaptic Terminals):The branched endings of the axon. These are where the neuron communicates with other cells at junctions calledsynapses. They contain vesicles filled withneurotransmitters, chemical messengers that transmit the signal across the synapse.
- Myelin Sheath:Many axons, especially long ones, are covered by a fatty layer called the myelin sheath. In the peripheral nervous system, this sheath is formed bySchwann cells; in the central nervous system, it's formed byoligodendrocytes(types of neuroglia). The myelin sheath acts as an insulator, greatly speeding up the conduction of electrical signals along the axon by allowing the signal to jump between gaps in the sheath calledNodes of Ranvier(this is calledsaltatory conduction). Not all axons are myelinated (unmyelinated axons conduct signals more slowly).
Neuroglial Cells (Glial Cells):These are non-excitable supporting cells found in nervous tissue. They do not transmit nerve impulses themselves, but they play crucial roles in supporting, nourishing, insulating, and protecting neurons. They are often more numerous than neurons. Different types exist in the central and peripheral nervous systems:
- Neuroglia in the Central Nervous System (CNS - Brain and Spinal Cord):
- Astrocytes:Star-shaped cells that are the most abundant neuroglia in the CNS. They form a supportive framework, help regulate the chemical environment around neurons (mopping up excess neurotransmitters), help form theblood-brain barrier(which protects the brain from harmful substances in the blood), and assist in guiding neuron development.
- Microglia:Small, mobile cells that act as the CNS's immune cells. They are phagocytic, meaning they engulf and remove cellular debris, dead neurons, and pathogens. They are like the cleanup crew and defense system of the brain and spinal cord.
- Ependymal Cells:Epithelial-like cells that line the cavities within the brain (ventricles) and spinal cord (central canal). They help produce and circulatecerebrospinal fluid (CSF), which cushions the CNS.
- Oligodendrocytes:Cells that form themyelin sheatharound axons in the CNS. Each oligodendrocyte can myelinate multiple axon segments.
- Neuroglia in the Peripheral Nervous System (PNS - Nerves outside the Brain and Spinal Cord):
- Schwann Cells:These cells form themyelin sheatharound axons in the PNS. Unlike oligodendrocytes, each Schwann cell typically myelinates only a single axon segment. They are crucial for regeneration of damaged peripheral nerve fibers.
- Satellite Cells:Flattened cells that surround neuron cell bodies in ganglia (collections of neuron cell bodies in the PNS). They provide support and regulate the chemical environment around the neurons.
Organization of Peripheral Nerves and Ganglia
While the brain and spinal cord make up the central nervous system (CNS), thePeripheral Nervous System (PNS)consists of all the nerves that extend outside the CNS, connecting it to the rest of the body, and collections of neuron cell bodies outside the CNS called ganglia.
Peripheral Nerves:A nerve is essentially a bundle of many axons (nerve fibers) wrapped in connective tissue. Think of it like a communication cable containing many individual wires. The structure of a peripheral nerve from the inside out includes:
- Axon (Nerve Fiber):The core of the structure, carrying the electrical signal. May or may not be covered by a myelin sheath formed by Schwann cells.
- Endoneurium:A delicate layer of loose connective tissue that surrounds each individual axon (nerve fiber), including its myelin sheath if present.
- Fascicle:A bundle of several axons wrapped together by a coarser connective tissue layer.
- Perineurium:A layer of dense irregular connective tissue that surrounds a fascicle. It forms a protective barrier around the axon bundles.
- Epineurium:The outermost, tough fibrous sheath of dense irregular connective tissue that surrounds the entire nerve, enclosing all the fascicles, blood vessels, and lymphatic vessels supplying the nerve.
Ganglia (Singular: Ganglion):A ganglion is a collection or cluster of neuroncell bodieslocated in the peripheral nervous system. They are like "relay stations" or "switching centers" where nerve impulses are processed or relayed.
- Sensory Ganglia:Contain the cell bodies of sensory neurons (e.g., dorsal root ganglia near the spinal cord).
- Autonomic Ganglia:Contain the cell bodies of autonomic motor neurons, which regulate involuntary functions (e.g., sympathetic and parasympathetic ganglia).
Disorders affecting Nervous Tissue:
- Neuropathy:Damage to peripheral nerves, leading to pain, numbness, tingling, and weakness (e.g., diabetic neuropathy, carpal tunnel syndrome).
- Neurodegenerative Diseases:Conditions involving progressive loss of neurons (e.g., Alzheimer's disease, Parkinson's disease).
- Stroke:Damage to brain tissue due to interruption of blood supply, causing neuronal death.
- Spinal Cord Injury:Damage to the spinal cord, disrupting communication between the brain and the body.
- Tumors:Cancers can arise from neuroglial cells (gliomas) or neurons (less common).
Revision Questions: Cell and Tissues
Test your understanding of the key concepts covered in this section:
- State the three main tenets of the Cell Theory and explain their significance in understanding living organisms.
- Describe the main structural components of a typical eukaryotic (human) cell, including the plasma membrane, cytoplasm (cytosol and organelles), and nucleus. Briefly explain the primary function of at least five different organelles.
- Explain the concept of functional specialization in cells and provide three specific examples of how different cell types in the body are specialized for unique functions, relating their structure to their job (e.g., muscle cells, neurons, red blood cells).
- Outline the main phases of the cell cycle (Interphase and Mitotic Phase) and briefly describe what happens in each phase. Why is the regulation of the cell cycle crucial for health? What happens when this regulation fails?
- Compare and contrast the structure, location, control, and regenerative capacity of the three types of muscle tissue (Skeletal, Smooth, and Cardiac).
- Describe the key characteristics of connective tissue that distinguish it from epithelial tissue. Explain the role of the extracellular matrix in connective tissue.
- Name and describe the main components of blood. Explain why blood is considered a connective tissue despite its fluid nature. List three major functions of blood.
- Compare and contrast the three types of cartilage (Hyaline, Elastic, Fibrocartilage) in terms of their fiber composition, properties, and locations in the body. Why does cartilage heal slowly?
- Describe the structural features of bone tissue, including the different cell types (osteoblasts, osteocytes, osteoclasts) and the composition of the bone matrix. Explain the difference between compact bone and spongy bone.
- Explain the main structural components of a neuron (cell body, dendrites, axon, axon terminals) and their respective functions in transmitting nerve impulses. Describe the role of the myelin sheath.
- Identify the different types of neuroglial cells found in the Central Nervous System (CNS) and Peripheral Nervous System (PNS). Briefly explain the function of at least three types of neuroglia.
- Describe the organization of a peripheral nerve, including the Epineurium, Perineurium, and Endoneurium. What is a ganglion, and how does it differ structurally from a peripheral nerve?
- Discuss one common disorder for each of the four main tissue types (Epithelial, Connective, Muscle, Nervous) and briefly explain how the tissue is affected in each disorder.
References for BNS 111: Anatomy & Physiology
- Tortora, G.J. & Derickson N.,P. (2006) Principles of Anatomy and Physiology; Harper and Row
- Drake, R, et al. (2007). Gray's Anatomy for Students. London: Churchill Publishers
- Snell, SR. (2004) Clinical Anatomy by Regions. Philadelphia: Lippincott Publishers
- Marieb, E.N. (2004). Human Anatomy and physiology. London: Daryl Fox Publishers.
- Young, B, et al. (2006). Wheater's Functional Histology: A Text and Colour Atlas: Churchill
- Sadler, TW. (2009). Langman's Medical Embryology. Philadelphia: Lippincott Publishers

PYELONEPHRITIS

Classification & Specific Types of Pyelonephritis

ACUTE PYELONEPHRITIS
This is characterized by acute inflammation of the parenchyma(core substance of the kidney/kidney tissue) and the pelvis of the kidneys, Characterized by a sudden onset of symptoms.
The disease may be bilateral or unilateral. This usually results from untreated bacterial cystitis and may be associated with pregnancy, trauma of the urinary bladder, and urinary obstruction Also Ascending and Descending infections.
Can range from mild, manageable outpatient cases to severe infections requiring hospitalization, potentially complicated by sepsis or abscess. Severity can be increased in the elderly, immunocompromised individuals (e.g., cancer, AIDS), or those with underlying structural abnormalities.
Morphology:
- Gross Anatomy: Kidney(s) are often enlarged and swollen due to inflammation and edema. The capsule may be tense. On the cut section, characteristic yellowish, raised, discrete abscesses or streaks of pus may be visible on the cortical surface and extending into the medulla, often following the path of collecting ducts. The renal pelvis and calyces may show hyperemia (redness) and purulent exudate.
- Microscopic Examination: Shows characteristic tubulointerstitial inflammation. Neutrophils infiltrate the interstitial tissue and accumulate within tubular lumens (forming pus casts). There is associated tubular necrosis and destruction. Glomeruli are typically spared initially, although surrounding inflammation can occur. Blood vessels usually show resistance to infection but can be involved in severe cases or vasculitis.
Clinical Features of Acute Pyelonephritis
- Systemic Symptoms: Fever (often high-grade >38.5°C), chills, rigors, malaise, nausea, vomiting.
- Localizing Symptoms: Flank pain or back pain (typically unilateral, localized to the costovertebral angle – CVA tenderness on examination is a key sign).
- Lower UTI Symptoms (May or May Not be Present): Dysuria (painful urination), frequency, urgency. Absence doesn’t rule out pyelonephritis.
- Urine: May appear cloudy or malodorous; hematuria (blood in urine) can occur.
- Examination Findings: Fever, tachycardia, CVA tenderness. Abdominal tenderness may be present. Signs of dehydration. In severe cases, signs of sepsis (hypotension, altered mental status).
- Laboratory Findings: Urinalysis typically shows pyuria (pus/WBCs), bacteriuria, often hematuria, mild proteinuria, and crucially, WBC casts (formed in tubules, indicating renal parenchymal involvement). Urine culture confirms the diagnosis and identifies the organism (>10^4 or >10^5 CFU/mL typically significant). Blood tests show leukocytosis (high WBC count) with a left shift (increased neutrophils), elevated inflammatory markers (ESR, CRP). Blood cultures should be drawn if sepsis is suspected (positive in 15-30% of cases).
Presentation; flunk tenderness,
- fever, chills
- Dysuria
- Urgency
- frequency
Complications of Acute Pyelonephritis
- Papillary Necrosis: Ischemic necrosis of the renal papillae, more common in diabetics, those with obstruction, or sickle cell disease. Can lead to sloughing of papillae, obstruction, and worsening renal function.
- Pyonephrosis: Pus collection within an obstructed renal collecting system, essentially converting the kidney into a sac of pus. Requires urgent drainage.
- Perinephric Abscess: Collection of pus in the space surrounding the kidney, between the renal capsule and Gerota’s fascia. Often requires drainage (percutaneous or surgical).
- Intrarenal Abscess: Abscess formation within the kidney parenchyma.
- Sepsis/Urosepsis: Systemic inflammatory response syndrome (SIRS) due to infection originating in the urinary tract. Can lead to septic shock and multi-organ failure.
- Emphysematous Pyelonephritis: A rare, life-threatening necrotizing infection characterized by gas formation within the kidney parenchyma. Often associated with diabetes and requires aggressive management, sometimes nephrectomy.
- Renal Scarring: Can occur even after a single episode, especially if treatment is delayed or infection is severe.
- Acute Kidney Injury (AKI): Temporary decline in kidney function due to infection and inflammation.



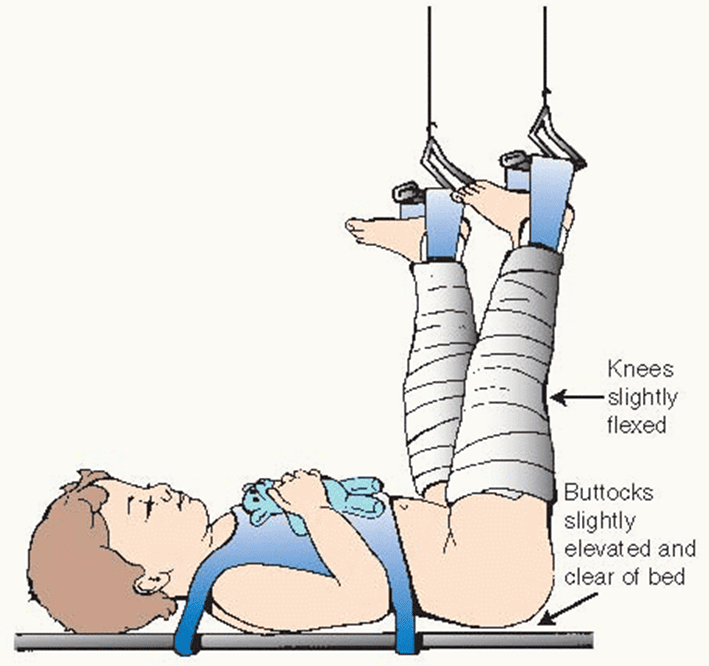
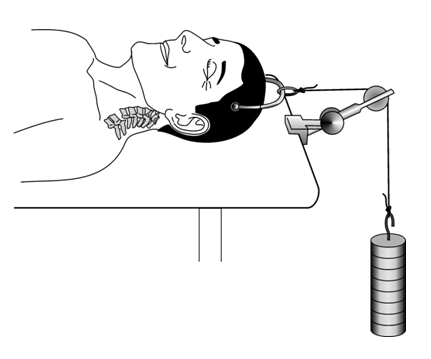
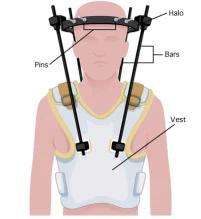
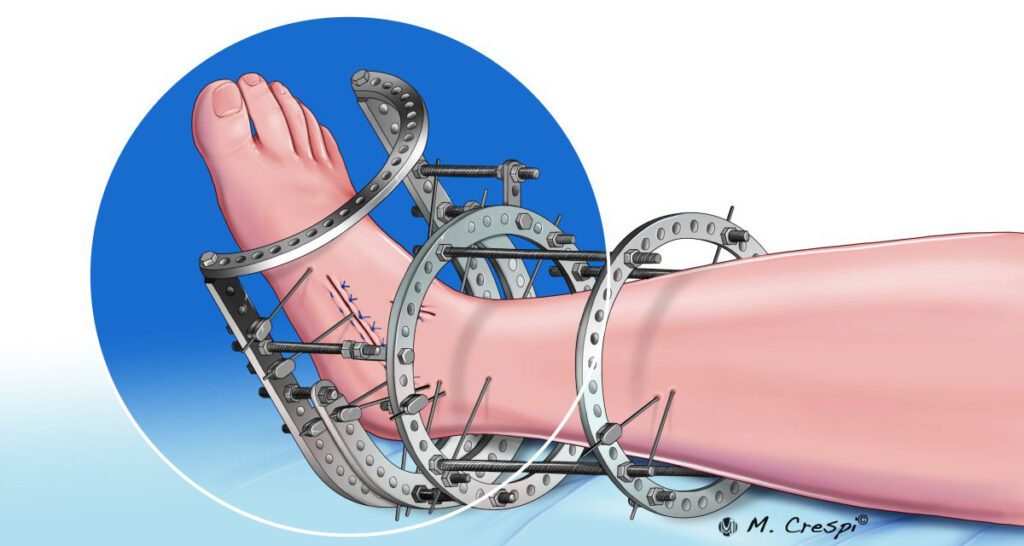
Traction in Nursing
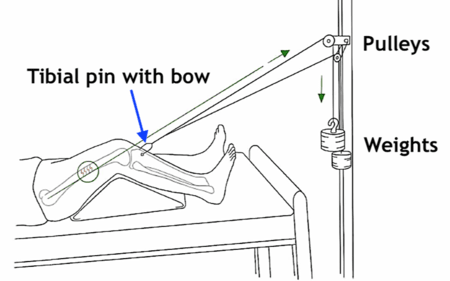
SKELETAL TRACTION
Skeletal traction is the type of traction in which a pin, nail, or wire is passed through a bone. This type of traction is mainly used for the treatment of fractures and works better for well-built strong persons.
Common sites for introducing the pins include:
- The condyles of the femur
- The tubercles of the tibia
- Calcaneus at the heels of the foot
Metallic equipment used in skeletal traction:
- Steinmann’s pins: This is a rigid steel pin passed through a bone and attached to a special stirrup. Because of the presence of the stirrup, the surgeon is able to alter the line of the pull without moving the pin.

- Kirschner wire: This is a narrow steel wire which is not rigid unless pulled on by a stirrup. When the stirrup is rotated, it can move the wire, increasing the risk of infection. Therefore, it is not as commonly used compared to Steinmann’s pin.
Preparation of the patient for skeletal traction:
- Explain the procedure to the patient and provide reassurance to allay anxiety
- Shave the area if the patient is hairy
- Administer premedication if prescribed
- Establish an intravenous line
After preparation, the patient is taken to the theater with the leg in a Thomas splint with skin traction applied. The operation is performed under general anesthesia to insert the Steinmann’s pin through the bone. A stirrup is then attached to the pin, and the patient is returned to the ward.


Traction in Nursing Read More »



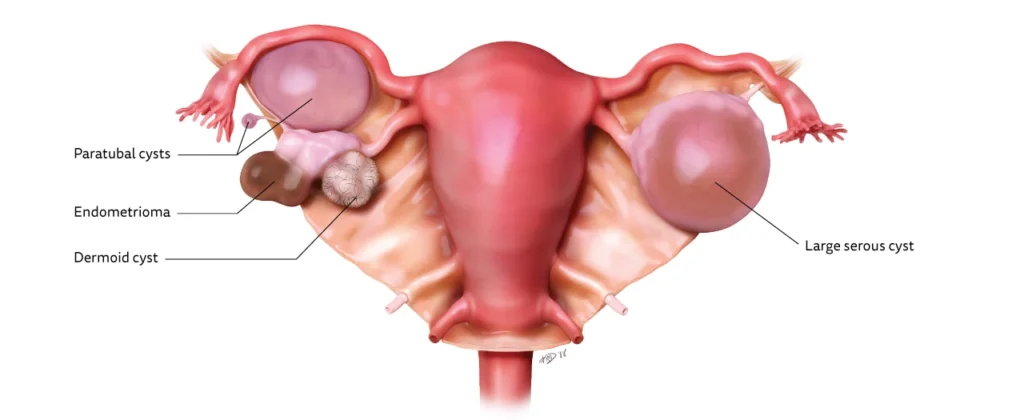
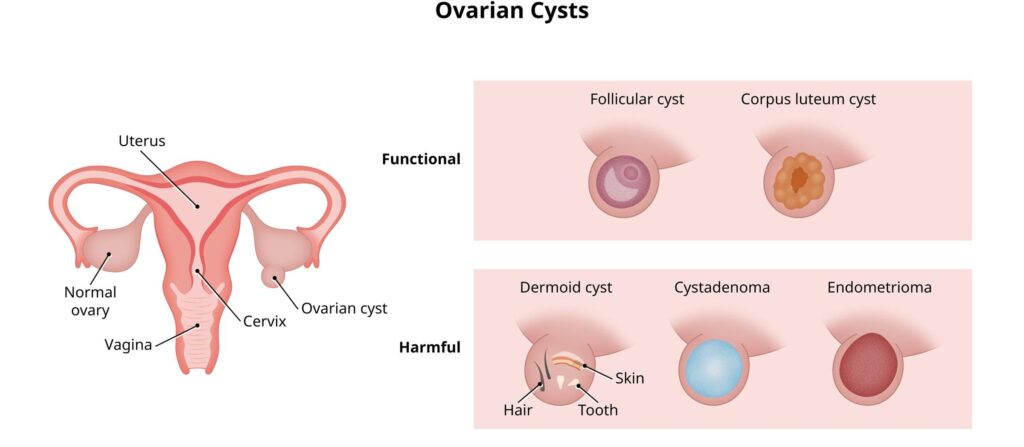
Ovarian Cysts
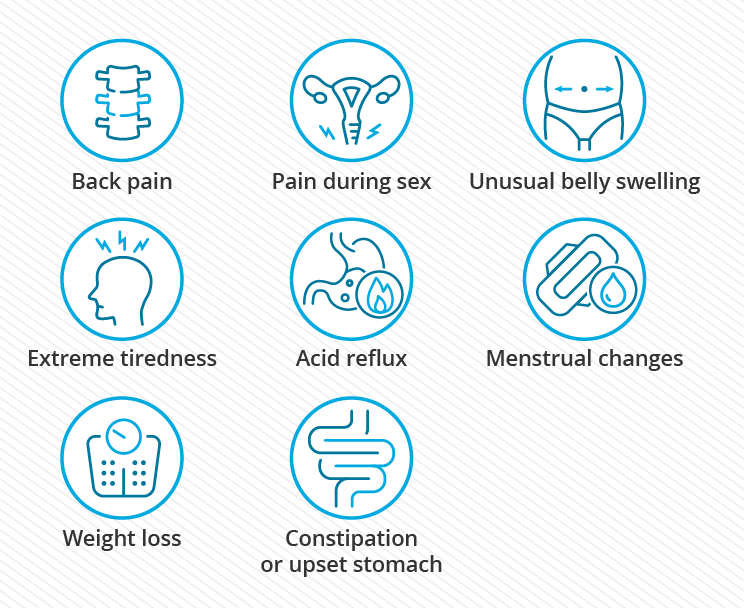
Signs and Symptoms of Ovarian Cysts:
- Often asymptomatic
- Pelvic pain or discomfort: Ovarian cysts can cause pelvic pain (sharp or dull) or pressure in the pelvic area.
- Bloating or abdominal swelling: Some women may experience bloating or a feeling of fullness in the abdomen.
- Irregular menstrual cycles: Ovarian cysts can disrupt the normal menstrual cycle, leading to irregular periods.
- Pain during intercourse: Cysts may cause pain or discomfort during sexual intercourse.
- Changes in urinary patterns: Ovarian cysts can put pressure on the bladder, leading to increased frequency or urgency of urination.
- Digestive issues: Large cysts may cause digestive symptoms such as nausea, vomiting, or changes in bowel movements.
- Painful bowel movements: Cysts can put pressure on the rectum, causing pain or discomfort during bowel movements.
- Fatigue or low energy: Some women with ovarian cysts may experience fatigue or a general feeling of low energy.
- Breast tenderness: Ovarian cysts can sometimes cause breast tenderness or changes in breast size.
Signs and Symptoms of Ruptured Ovarian Cysts:
- Sudden, severe abdominal or pelvic pain: A ruptured ovarian cyst can cause intense pain in the lower belly or back.
- Vaginal spotting or bleeding: After a cyst ruptures, some women may experience vaginal spotting or bleeding.
- Abdominal bloating: Bloating or a feeling of fullness in the abdomen may occur after a cyst ruptures.
- Severe nausea and vomiting: In some cases, a ruptured cyst may cause severe nausea and vomiting.
- Faintness or dizziness: Feeling lightheaded, faint, or dizzy can be a symptom of a ruptured ovarian cyst.
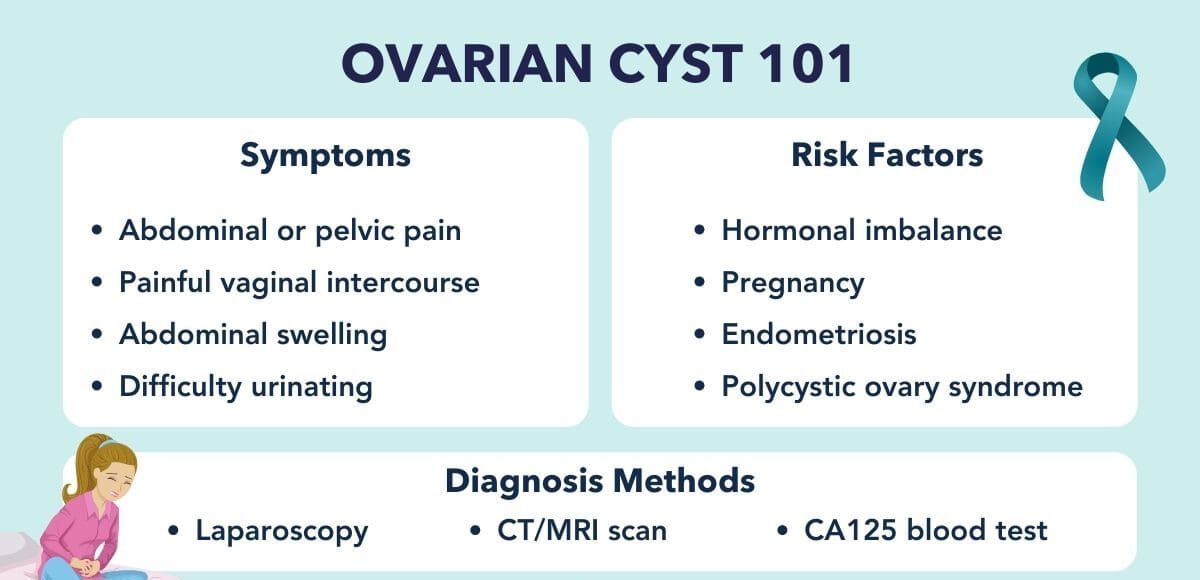
Diagnosis of Ovarian Cysts:
Medical History and Physical Examination:
- History of signs and symptoms, medical history, and any risk factors associated with ovarian cysts.
- A pelvic examination may be performed to check for any abnormalities or signs of a cyst.
- Pregnancy test : A positive pregnancy test result may suggest the patient has a corpus luteum cyst.
Imaging Tests:
- Pelvic Ultrasound: This is the most commonly used imaging test for diagnosing ovarian cysts. It can provide detailed images of the ovaries and help determine the size, location, and characteristics of the cyst.
- Transvaginal Ultrasound: In some cases, a transvaginal ultrasound may be performed, where a small probe is inserted into the vagina to obtain clearer images of the ovaries.
Blood Tests:
- CA-125 Test: This blood test measures the level of a protein called CA-125, which can be elevated in certain cases of ovarian cysts, including those that are cancerous.
- Hormone Level Tests: Blood tests may be done to check hormone levels, such as estrogen and progesterone, which can help determine the type of cyst.
Laparoscopy:
- In some cases, a laparoscopy may be recommended. It is a surgical procedure where a small incision is made in the abdomen, and a thin tube with a camera is inserted to visualize the ovaries and confirm the presence of a cyst.
Biopsy:
- If there is a suspicion of ovarian cancer, a biopsy may be performed to obtain a tissue sample for further analysis.
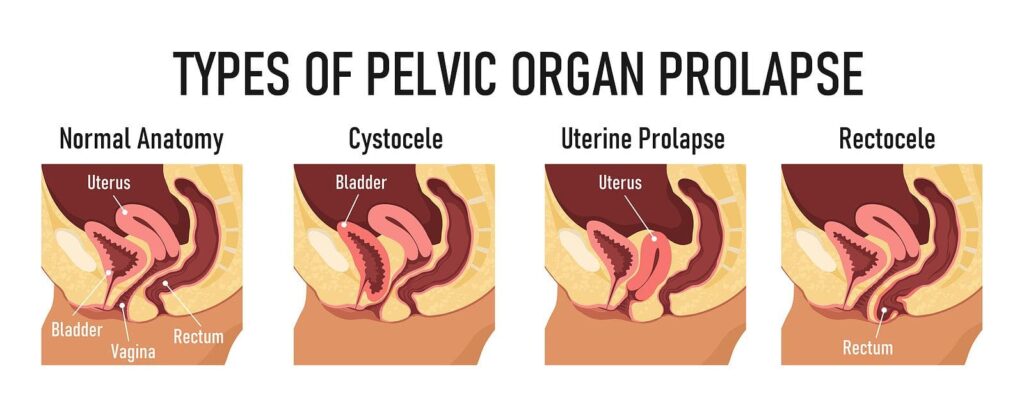
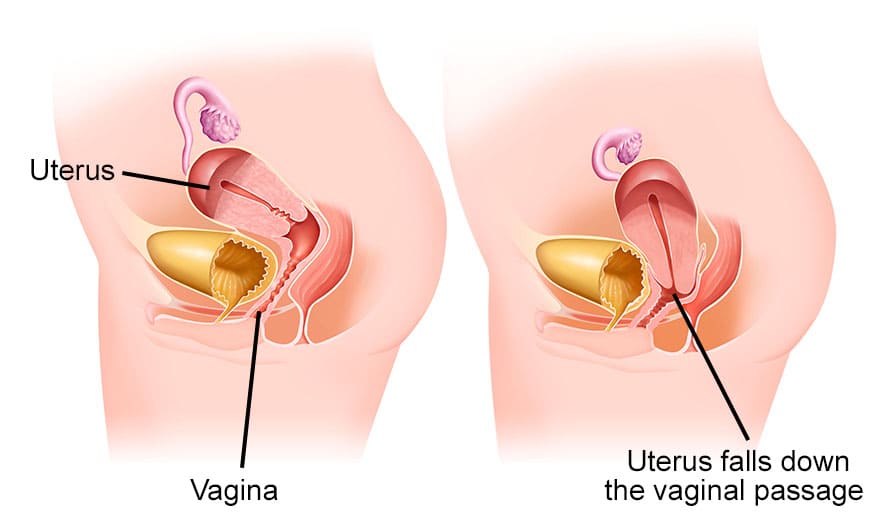
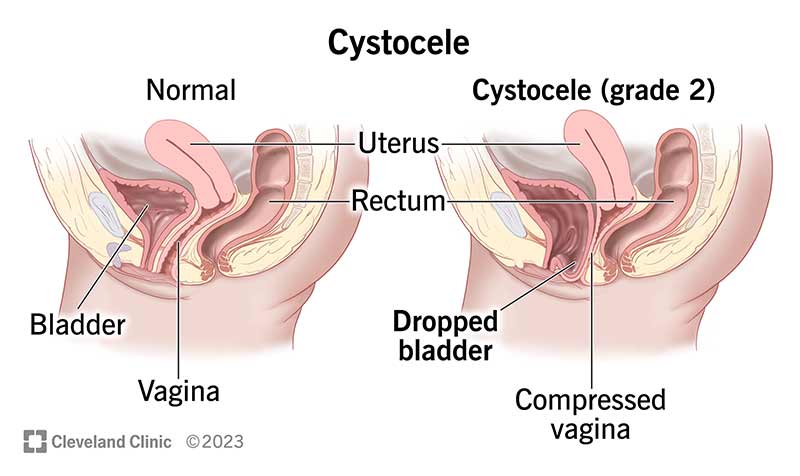
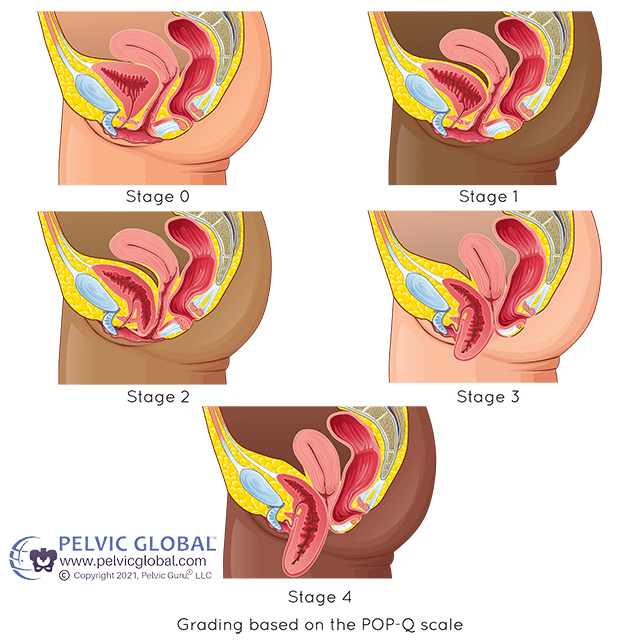
Pelvic Organ Prolapse (POP)
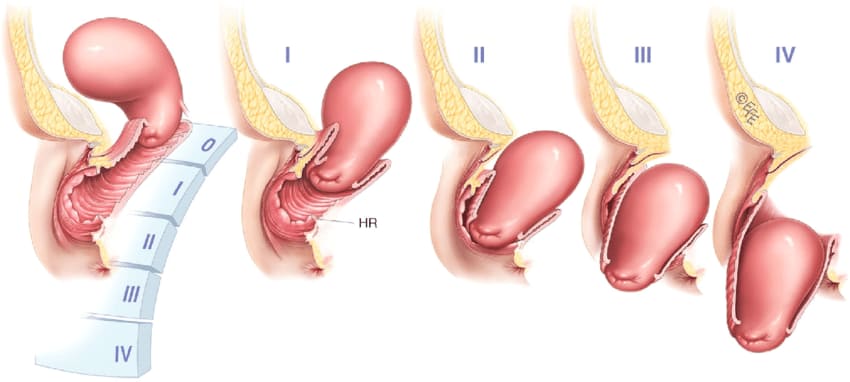
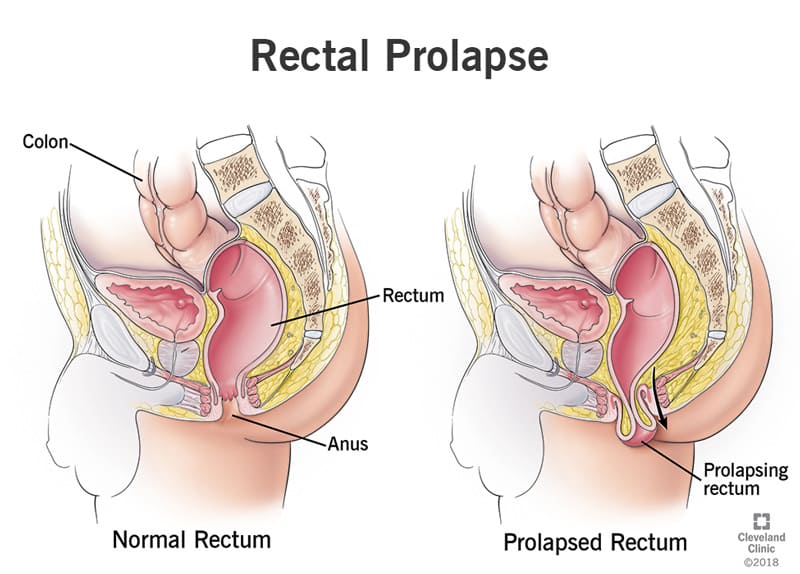
Rectal Prolapse
Rectal prolapse occurs when the rectum (the last section of the large intestine) falls from its normal position within the pelvic area and protrudes through the anus.
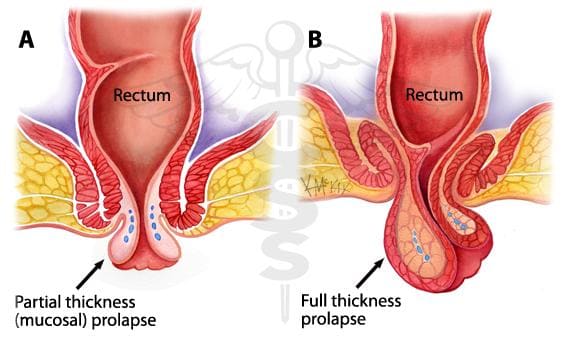
It can involve a mucosal or full-thickness layer of rectal tissue.
Pelvic Organ Prolapse (POP) Read More »