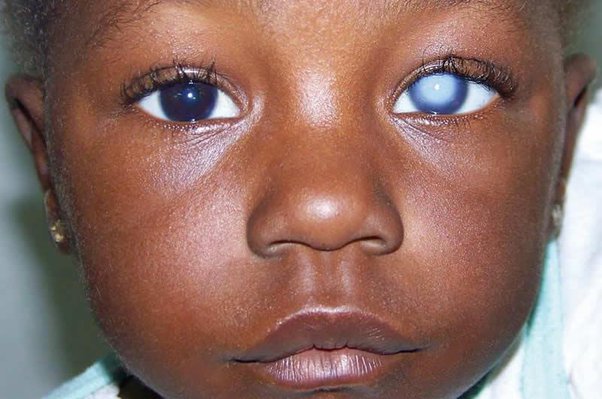
CONGENITAL CATARACTS
Classifications of Congenital Cataracts.
Congenital cataracts can be classified based on various factors such as morphology, age of onset, and etiology.
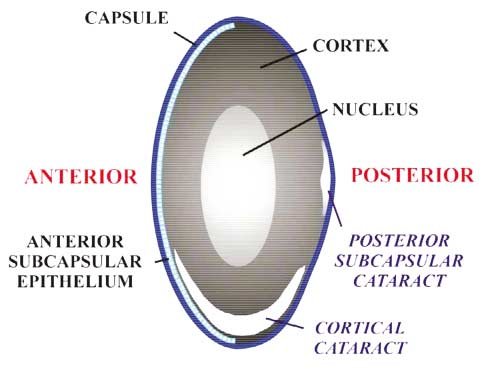
Morphology: Based on their physical appearance.
- Polar Cataract: Lens opacities that involve the subcapsular cortex and lens capsule of the anterior or posterior pole of the lens. Anterior polar cataracts present as Small, bilateral, symmetric, non progressive opacities that do not impair vision. Posterior polar cataracts produce more visual impairment than anterior polar cataracts because they tend to be larger and are positioned closer to the nodal point of the eye.
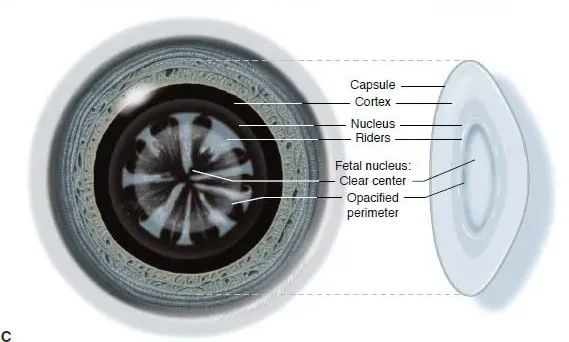
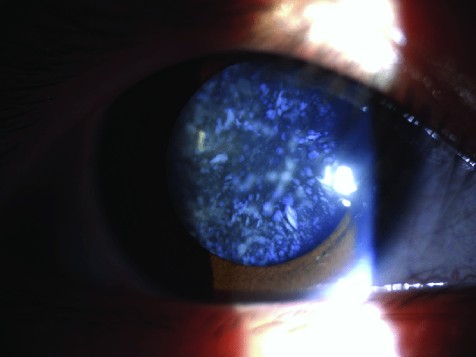
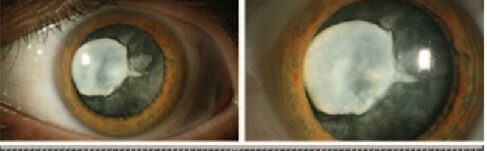
- Lamellar Cataract/Zonular Cataract: Lamellar cataracts are the most common type of congenital cataracts. The cataract is visible as an horseshoe- shaped opacity that surrounds a clearer center and is itself surrounded by a layer of clear cortex. Lamellar cataracts may be inherited or result from a transient toxic influence during embryonic lens development.
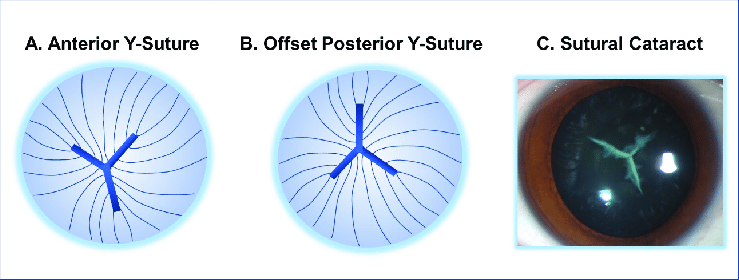
- Sutural Cataract: Opacification of the Y-sutures of the fetal nucleus that commonly do not impair vision. They are usually bilateral, symmetric, and frequently inherited in an autosomal dominant pattern. These opacities often have branches or knobs projecting from them.

- Coronary Cataract: Coronary cataracts consist of club-shaped cortical opacities arranged around the equator of the lens like a crown or corona. They cannot be seen unless the pupil is dilated, and they usually do not affect visual acuity. They are often inherited in an autosomal dominant pattern.
- Cerulean Cataract/Blue-dot Cataract: Cerulean cataracts are small bluish opacities located in the lens cortex. They are nonprogressive and usually do not cause visual symptoms.
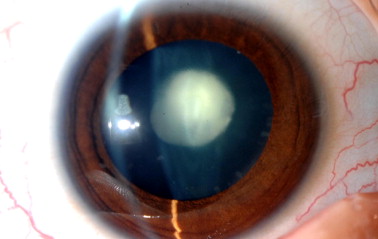
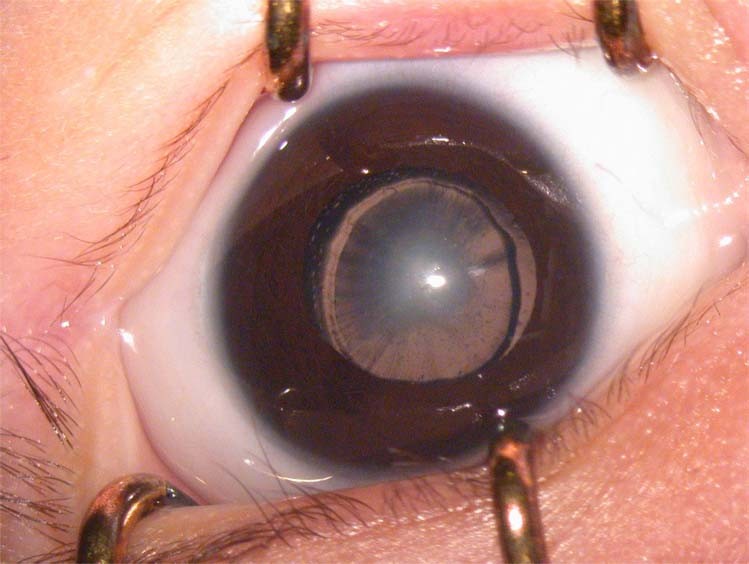
- Nuclear Cataract: Opacities of either the embryonic nucleus alone or both the embryonic and fetal nuclei. They are usually bilateral, with a wide spectrum of severity. Eyes with congenital nuclear cataracts tend to be microphthalmic and have an increased risk of developing aphakic glaucoma.
- Capsular Cataract: Small opacifications of the lens epithelium and anterior lens capsule that spare the cortex. They are differentiated from anterior polar cataracts by their protrusion into the anterior chamber, but generally do not affect vision.
- Membranous Cataract: Membranous cataracts occur when lens proteins are resorbed, allowing the anterior and posterior lens capsules to fuse into a dense white membrane. They cause significant visual disability due to the resulting opacity and lens distortion.
Age of Onset:
- Congenital/Infantile cataract: Lens opacities present at birth.
- Acquired/Juvenile cataract: Onset after infancy, in childhood.
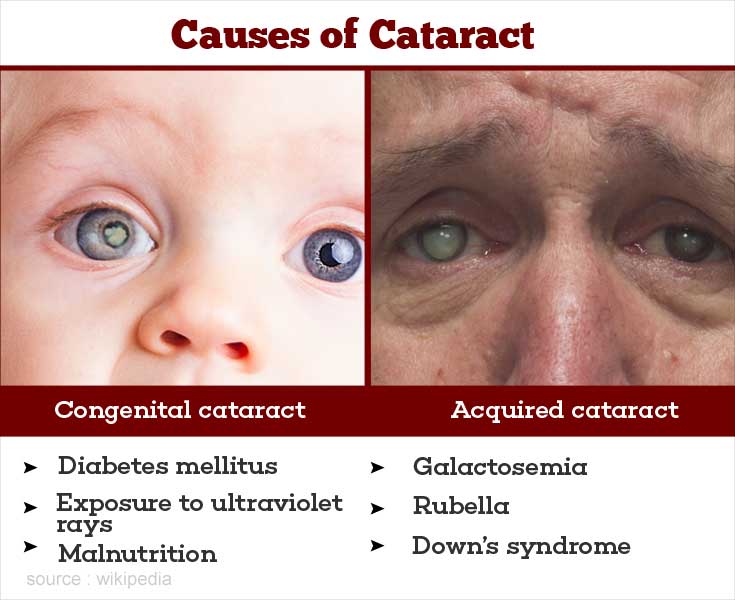
Etiology:
- Genetic cataract/Hereditary: Caused by mutations in genes involved in lens structure or clarity. The affected individuals are usually perfectly well, and have no associated systemic illness. Associated with microphthalmos.
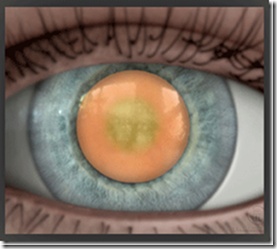
- Metabolic cataract: Caused by metabolic disorders such as galactosemia, hypoglycemia, hypocalcemia. Galactosemia is a metabolic disorder in which the child’s body cannot metabolize galactose, a major component of milk and milk products. The baby develops typical ‘oil droplet’ cataracts which are easily seen by examining the red reflex. These are reversible, and the lens returns to normal on removing dairy products from the diet.
- Traumatic cataract: Caused by external injuries to the eye. Trauma is the most common cause of unilateral cataract in children. Traumatic cataract is usually the result of a penetrating injury, though blunt trauma can also lead to cataract formation.
- Secondary cataracts: Such as those secondary to marternal infection during pregnancy. TORCH syndrome: Toxoplasmosis, Others(Syphilis, Hepatitis B), Rubella, Cytomegalovirus (CMV), Herpes infection.. Usually bilateral, dense, and central. The most common maternal infection to cause congenital cataract in the child is Rubella. The cataracts caused by Rubella may be present at birth, or develop several months later.
- Iatrogenic cataract: Caused by well-intentioned medical treatment, Such as Radiation, Drugs, Surgeries, e.t.c. latrogenic cataract is most commonly seen in children who have had Total body irradiation for leukemia, Organ transplants, On long-term systemic steroid therapy. These children are usually older children and do very well after cataract surgery.

CONGENITAL CATARACTS Read More »