HEALTH AND DISEASE
HEALTH AND DISEASE
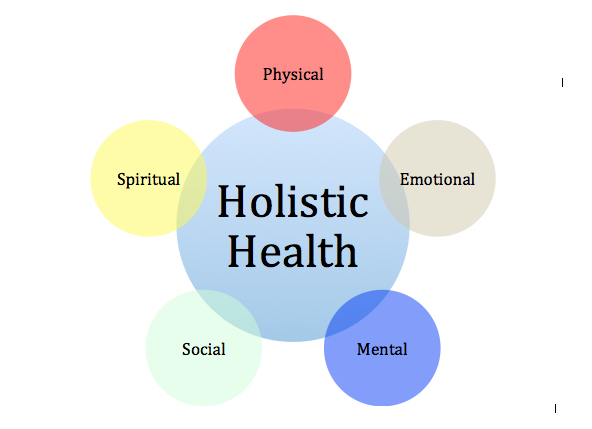
Health: Health refers to a state of complete physical, mental, and social well-being, and not merely the absence of disease or infirmity.
Disease: A disease is a specific abnormal condition that affects the body or mind and impairs normal functioning. It is often characterized by specific symptoms and signs.
Terminologies Used
- Endemic: Prevailing or continuously present in a community, e.g., TB and Malaria, Malnutrition, or diseases that are constantly found among people in a particular area.
- Epidemic: A widespread occurrence of an infectious disease in a community at a particular time.
- Prevalence: The number of cases of a disease existing at a particular time within a given population.
- Prevalence Rate: The proportion of people in a population who have a particular disease at a specified point in time or over a specified period.
- Pandemic: A disease widely prevalent in a population, e.g., HIV/AIDS.
- Sporadic: Occurrence at irregular intervals or only in a few places; scattered or isolated.
- Quarantine: Used to separate and restrict the movement of well persons who may have been exposed to a communicable disease to see if they become ill. It is often mistakenly used interchangeably with isolation, which means to separate ill persons who have a communicable disease from those who are healthy.
- Maternal Death: The death of women while pregnant or within 42 days of the termination of pregnancy.
- Mortality: The state of being subject to death.
- Infant Mortality: The death of a child less than one year of age.
- Infant Mortality Rate: The number of infants dying in the first month (year) of life (under 28 days) in a year per 1000 live births in the same year.
- Perinatal Mortality Rate: The number of stillbirths plus deaths in the first week of life per 1000 live births in a year.
- Postnatal Mortality Rate: The number of infants’ deaths at 28 days of one year of age per 1000 live births in a given year.
- Morbidity: A diseased state or symptom.
- Bioterrorism: The threatened or intentional release of biological agents (viruses, bacteria, or their toxins) for the purpose of influencing the conduct of government or intimidating or coercing a civilian population to further political or social objectives. These agents can be released via the air (aerosols), food, water, or insects.
Disease Causation and Prevention
Definition of Disease: A condition that impairs normal body functioning, typically manifested by distinguishing signs and symptoms. It represents a departure from a state of health. Diseases can be broadly categorized as communicable (infectious) or non-communicable (non-infectious).
Causes of Disease (Etiology)
Understanding the etiology of a disease is crucial for effective prevention and treatment. Diseases can arise from a variety of factors, often in combination:
Biological Agents: These are living organisms that can cause disease, often referred to as pathogens.- Bacteria: Single-celled microorganisms (e.g., strep throat, tuberculosis).
- Viruses: Tiny infectious agents that replicate inside living cells (e.g., common cold, flu, HIV).
- Fungi: Eukaryotic organisms that can cause infections (e.g., athlete's foot, ringworm).
- Parasites: Organisms that live on or in a host and derive nutrients at the host's expense (e.g., malaria, hookworm).
- Single Gene Disorders: Caused by a mutation in one gene (e.g., cystic fibrosis, sickle cell anemia).
- Chromosomal Disorders: Involve changes in the number or structure of chromosomes (e.g., Down syndrome).
- Complex (Multifactorial) Disorders: Result from a combination of genetic and environmental factors (e.g., heart disease, diabetes, some cancers).
- Physical Agents: Radiation, extreme temperatures, noise pollution, injury.
- Chemical Agents: Toxins, pollutants (e.g., lead poisoning, pesticide exposure), allergens.
- Nutritional Deficiencies or Excesses: Lack of essential nutrients (e.g., scurvy from vitamin C deficiency) or excessive intake (e.g., obesity).
- Diet: Unhealthy eating habits (high in processed foods, sugar, unhealthy fats).
- Physical Activity: Sedentary lifestyle.
- Smoking and Alcohol Consumption: Major risk factors for numerous diseases.
- Stress: Chronic stress can impact various bodily systems.
- Sleep: Insufficient or poor quality sleep.
- Autoimmune Diseases: Immune system attacks the body's own healthy cells (e.g., rheumatoid arthritis, lupus).
- Immunodeficiency: Weakened immune system making the body more susceptible to infections (e.g., HIV/AIDS).
Modes of Disease Transmission (for Communicable Diseases)
Understanding how infectious diseases spread is fundamental to their prevention.
Direct Contact:- Person-to-person: Touching, kissing, sexual contact (e.g., common cold, STIs).
- Droplet Spread: Respiratory droplets from coughing or sneezing (e.g., influenza).
- Airborne Transmission: Droplet nuclei or dust particles suspended in the air (e.g., measles, tuberculosis).
- Vehicle-borne Transmission: Contaminated inanimate objects (fomites) like doorknobs, toys, or contaminated food/water (e.g., food poisoning, cholera).
- Vector-borne Transmission: Living organisms (vectors) like mosquitoes, ticks, or fleas transmit the pathogen (e.g., malaria, Lyme disease).
Strategies for Disease Prevention and Control
A multi-faceted approach is often required for effective disease prevention.
- Immunization Programs: Widespread vaccination to achieve herd immunity.
- Sanitation and Hygiene: Ensuring safe water, proper waste disposal, and promoting personal hygiene practices.
- Disease Surveillance: Monitoring disease patterns and outbreaks to facilitate rapid response.
- Health Education and Promotion: Empowering individuals and communities with knowledge and skills to make healthy choices.
- Environmental Regulations: Controlling pollution and exposure to harmful substances.
- Healthy Lifestyle: Balanced diet, regular physical activity, adequate sleep, stress management.
- Personal Hygiene: Handwashing, proper food handling, respiratory etiquette.
- Seeking Medical Care: Regular check-ups, early symptom recognition, and adherence to treatment plans.
- Avoiding Risk Behaviors: Abstaining from smoking, limiting alcohol consumption, practicing safe sex.
- Vaccines: To prevent infectious diseases.
- Antimicrobials: Antibiotics, antivirals, antifungals for treating infections.
- Screening and Diagnostic Tests: For early detection.
- Medications: For managing chronic conditions.
- Surgery and Other Therapies: For treatment and management.
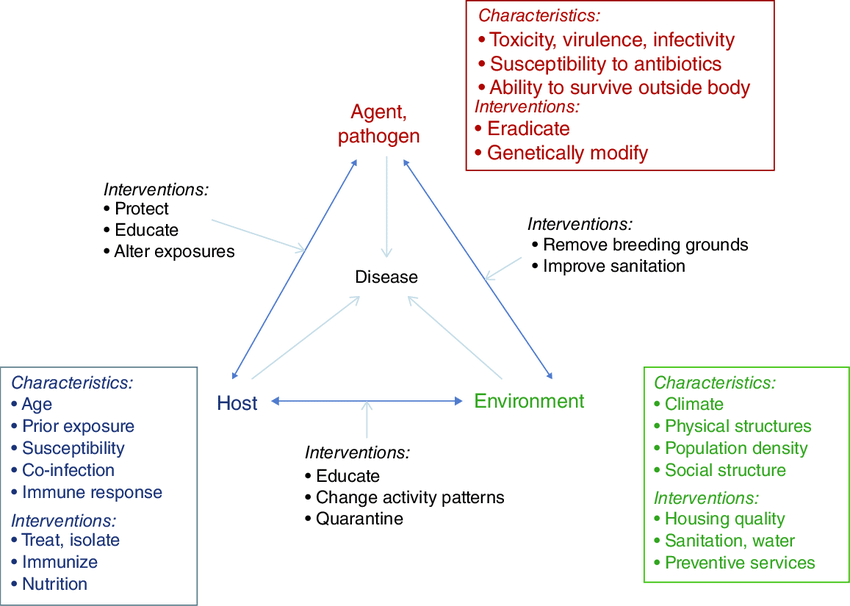
The Epidemiologic Triangle(The Epidemiological Triad)
This is the classic model for understanding infectious disease causation. It demonstrates that for a disease to occur, there must be an interaction between three components: an Agent, a Host, and an Environment.
Introduction
There are three elements that determine the etiology of health problems in a population: Agent, Host, and Environment. These are referred to as the epidemiological triad.
Epidemiology is the study of the distribution and determinants of diseases and health-related events in human populations.
A disease occurs when the agent is more powerful than the host, causing the host to weaken and the environment to become favorable for the growth, multiplication, and survival of the agent.
This is possible when the host becomes stronger, the agent is removed, and the environment becomes unfavorable to the agent.
Agent
It is a factor whose presence or absence causes a disease.
It is a specific factor without which a disease cannot occur.
- Biological: Bacteria, viruses, fungi, parasites.
- Chemical: Toxins, poisons, allergens.
- Physical: Trauma, radiation, heat.
- Nutritional: Lack or excess of certain nutrients.
A disease agent is defined as a substance, living or non-living, or a force, tangible or non-tangible, the excessive presence or relative lack of which is the immediate cause of a particular disease.
The disease agent is classified as follows:
- a) Endogenous: Some chemicals may be produced in the body as a result of decayed function, e.g., urea (uraemia), ketones, ketosis, sodium, bilirubin (jaundice), uric acid (gout), CaCO3 (kidney stones), among others.
- b) Exogenous Agents: These arise from outside the human host, such as allergens, metals, fumes, insecticides, etc. They may be acquired by inhalation, ingestion, or inoculation.
Host
Refers to humans or animals that come into contact with the agent.
Host factors influence the interaction with the agent and the environment.
- Age: The very young and the elderly are often more vulnerable.
- Sex: Some diseases are more common in one sex than another.
- Genetic Factors: Inherited traits can increase or decrease susceptibility.
- Immunity: Previous exposure or vaccination can provide protection.
- Lifestyle: Habits like diet, exercise, and smoking affect health.
Factors include age, sex, race, genetic factors, habits, nutrition, customs, human mobility, immunity, social status, economic status, educational status, and more.
Environment
Refers to the aggregate of all external conditions and influences affecting the life and development of organisms, human behavior, and society.
- Physical Environment: Climate, water and food quality, housing conditions.
- Social Environment: Cultural norms, socioeconomic status, access to healthcare.
- Biological Environment: Presence of insects (vectors) or other animals that can transmit the agent.
Includes physical environment (non-living things and physical factors), biological environment (living organisms), and social environment (cultural values, customs, habits, beliefs, attitudes, morals, religion, and other psychological factors).
Key Terms in Disease Causation
| Term | Definition |
|---|---|
| Infectivity | The ability of a pathogenic agent to enter, multiply, and establish an infection in a host. |
| Pathogenicity | The ability of an agent to cause disease in an infected host. |
| Virulence | The degree or severity of the disease caused by the agent. A highly virulent agent causes a more severe illness. |
| Susceptibility | The likelihood of a host becoming infected and developing the disease. A host with low immunity is highly susceptible. |
| Immunogenicity | The ability of an agent to produce an immune response in the host, which can lead to immunity. |
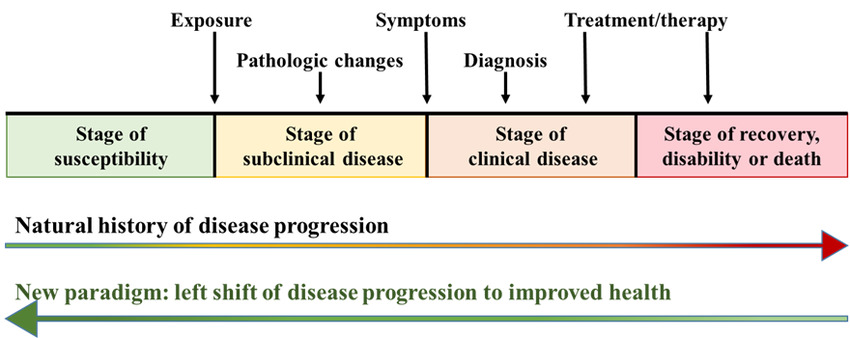
Natural History of Disease
The natural history of disease refers to the progression of a disease process in an individual over time, in the absence of intervention.
The process begins with exposure to or accumulation of factors capable of causing disease and ends with recovery, disability, or death.
Most diseases have a characteristic natural history, although the time frame and specific manifestations may vary from individual to individual.
Intervention can halt the usual course of a disease’s progression.
Main Stages of a Disease (Development of a Disease)
- Susceptible Stage: Conditions favoring disease development are present as risk factors, but the disease has not developed in the individual.
- Pre-symptomatic (Subclinical) Stage: Interaction of factors and pathogenic changes have occurred, but the disease has not manifested.
- Symptomatic (Clinical) Stage: Organ and functional changes have occurred, leading to recognizable signs and symptoms.
- Disability Stage: Inability stage, which may be partial or total disability.
Types of Diseases
- Communicable/Infectious Diseases
- Non-communicable/Non-infectious Diseases

Communicable/Infectious Diseases
Definition: Communicable disease is an illness due to specific infectious agents and their toxic products, which, under certain conditions, tend to spread among individuals in a community.
Period of Communicability: This refers to the time during which an infectious agent may be transferred directly or indirectly from an infected person to a susceptible person. This period is usually equal to the maximum known incubation period for that disease.
Examples of Communicable/Infectious Diseases:
- Tuberculosis
- Cholera
- Malaria
- Meningococcal meningitis and Niral meningitis
- Plague
- HIV
- Ebola virus and Marburg virus
- Hepatitis A, B, C, and E
Modes of Transmission of Communicable Diseases
The modes of transmission may be classified into two broad categories: direct and indirect.
Direct Transmission
- Direct Contact: e.g., sexual contact, kissing, and continued close contact. Diseases transmitted here include STIs/HIV, Leprosy, and Scabies.
- Droplet Infection: Through coughs, sneezing; diseases like common cold, TB, measles, whooping cough, meningitis, etc.
- Contact with Infected Soil: e.g., Tetanus infective hookworm larvae.
- Inoculation into Skin or Mucosa: e.g., animal bites (dog bites -rabies and HIV or Hepatitis B virus from contaminated needle pricks).
- Transplacental or Vertical Transmission: e.g., toxoplasmosis, HIV, rubella virus, syphilis.
Indirect Transmission
- Vehicle-Borne Transmission: The common vehicle of transmission is water, milk, or food; other vehicles may be blood, serum, plasma, and other biological products. This group includes waterborne, milk-borne, food-borne, and bloodborne infections, e.g., enteric fever, cholera, dysentery, diarrhea, hepatitis A, B, E, food poisoning.
- Vector-Borne Transmission: e.g., malaria, filarial, kala-azar, and plague are transmitted by insects. The mode of transmission is vector transmission.
- Airborne Transmission: e.g., Droplet nuclei (very small infective particles that float in the air, e.g., TB, infected dust; due to sweeping or dusty infected settled droplets on the ground.
- Fomite-Borne Transmission: Fomites are articles that convey infection to others because they have been contaminated, e.g., handkerchief, drinking glasses, doorknobs, clothing, etc. Highly infectious diseases, e.g., Ebola, can be easily transmitted by fomites.

Disease Transmission Cycle (The Chain of Infection)
For a communicable disease to spread, a series of linked events must occur. This is known as the Chain of Infection. Breaking any link in this chain can stop the spread of disease. As a nurse, understanding this cycle is fundamental to infection control.
- Infectious Agent: The pathogen (bacterium, virus, fungus, etc.) that causes the disease.
- Reservoir: The place where the infectious agent normally lives, grows, and multiplies. This can be humans, animals, or the environment (e.g., soil, water).
- Portal of Exit: The path by which the pathogen leaves the reservoir. Examples include respiratory tract (coughing, sneezing), gastrointestinal tract (feces, saliva), skin (wounds), or blood.
- Mode of Transmission: How the pathogen travels from the reservoir to the susceptible host.
- Direct Contact: Person-to-person physical contact (e.g., touching, kissing).
- Droplet Infection: Spread through respiratory droplets from coughing or sneezing that travel short distances.
- Indirect Contact: Spread via a contaminated intermediate object (called a fomite), such as a doorknob, medical equipment, or utensil.
- Airborne: Spread through tiny droplet nuclei that can remain suspended in the air for long periods and travel long distances.
- Vehicle-borne: Spread through a medium such as contaminated water, food, or blood.
- Vector-borne: Spread by an animal or insect, usually a biting arthropod (e.g., mosquito, tick).
- Portal of Entry: The path by which the pathogen enters a new host. This is often the same as the portal of exit (e.g., respiratory tract, broken skin, mucous membranes).
- Susceptible Host: An individual who is at risk of developing the infection. Factors increasing susceptibility include lack of vaccination, compromised immune system, malnutrition, and extreme age.
The nurse's role involves implementing strategies to break the chain, such as hand hygiene, using personal protective equipment (PPE), ensuring proper waste disposal, and patient education.
Other Terms Used in Communicable Diseases
- Zoonoses: An infectious disease transmissible under natural conditions from vertebrate animals to humans is called a zoonosis. There are over 150 diseases common to both humans and animals. Examples include anthrax, liver fluke, bovine TB, salmonellosis, brucellosis, rabies, plague, typhus, and yellow fever.
- Nosocomial Infections: An infection occurring in a patient in a hospital or other healthcare facility and in whom it was not present or incubating at the time of admission or arrival at a healthcare facility is called a nosocomial infection. It refers to diseases transmitted from a hospital. Usually, such infections are more difficult to manage as they are generally resistant to most common antibiotics. Nosocomial infections also include those infections contracted in the hospital but manifested after discharge and infections suffered by staff members if they were exposed to the infection from hospitalized patients.
- Herd Immunity: The immune status of a group of people/community is called herd immunity as it represents the immune status of the population. For many communicable diseases, an outbreak of the disease is only possible if the level of immunity is sufficiently low, and there are a large number of susceptible individuals in the population. In diseases like poliomyelitis, diphtheria, measles, etc., herd immunity plays an important role. However, in diseases like tetanus or rabies, where every individual is at risk unless specifically protected, herd immunity plays no role.
Factors Responsible for the Increased Risk of Infectious Diseases Are:
- Failure to control vectors, especially mosquitoes.
- Breakdown of the water and sanitation system.
- Failure to detect the disease early.
- Lack of immunization programs.
- High-risk human behavior.

Prevention & Control of Communicable Diseases
Methods/Approaches of Prevention and Control of Communicable Diseases
This refers to the reduction of the incidence and prevalence of communicable diseases to a level where they cannot be a major public health problem.
There are three main methods of controlling communicable diseases:
- Eliminating the reservoir (attacking the source)
- Interrupting transmission
- Primordial prevention
Eliminating the Reservoir (Attacking the Source)
- Detection and Adequate Treatment of Cases: This arrests the communicability of the disease, e.g., control of tuberculosis and leprosy and most sexually transmitted diseases.
- Isolation: This means that the person with the disease is not allowed to come into close contact with other people except those who are providing care, preventing the organism from spreading. It is used to control highly infectious diseases such as hemorrhagic viral fevers.
- Quarantine: Limitation of the movement of apparently well persons or animals who have been exposed to the infectious disease for the duration of the maximum incubation period of the disease.
- Reservoir Control: In diseases that have their main reservoir in animals, mass treatment, chemoprophylaxis, or immunization of the animals can be carried out, e.g., in brucellosis. Other methods include separating humans from animals or killing the animals and thus destroying the reservoir, e.g., plague, rabies, and hydatid disease.
- Notification: This means immediately informing the local health authorities (e.g., the District Medical Officer) if you suspect a patient is suffering from an infectious disease.
Interrupting Transmission
This involves the control of the modes of transmission from the reservoir to potential new hosts through:
- Environmental sanitation
- Personal hygiene and behavior change
- Vector control, e.g., mosquitoes
- Disinfection and sterilization
Protection of susceptible hosts
- Immunization: This increases host resistance by strengthening internal defenses. It is one of the most effective controls of communicable diseases in Africa. To be more effective, immunization has to be given to a high proportion of the population (at least 80%).
- Chemoprophylaxis: Drugs that protect the host may be used for suppressing malaria and preventing infection with diseases such as plague, meningitis, and tuberculosis.
- Personal Protection: The spread of some diseases may be limited by the use of barriers against infection, e.g., shoes to prevent the entry of hookworms from the soil, bed nets, and insect repellants to prevent mosquito bites.
- Better Nutrition: Malnourished children are more susceptible to infections and suffer more severe complications. Prevention and actions aimed at eradicating, eliminating, or minimizing the impact of disease and disability.
Primordial Prevention
This consists of actions and measures that inhibit the emergence of risk factors in a country or population. It begins with changes in social and environmental conditions.
Examples of primordial prevention actions:
- National policies and programs on nutrition involving the agricultural sector and the food industry.
- Comprehensive policies to discourage smoking.
- Programs to promote regular physical activity.
Screening of Diseases
Screening denotes the search for unrecognized diseases or defects in apparently healthy persons through the application of rapid diagnostic tests, examinations, or procedures. The basic objective of screening is to facilitate an early diagnosis so that the prognosis can be improved by remedial action.
Types of Epidemiological Disease Screening
- Mass Screening: When all members of a population are screened for disease, it is called mass screening. This is very costly, and the yield of cases is usually too small to warrant such a screening procedure.
- High-Risk Screening: High risk or selective screening refers to the situation where tests are offered only to those individuals who are at high risk of developing a specific disease. This makes the screening process more focused and reduces overall costs, as a large number of people with extremely remote chances of developing a disease are not screened.
The Sensitivity and Specificity of the Screening Test
- Sensitivity: This refers to the proportion of truly diseased individuals in the population who have been correctly identified as diseased by the screening test. A test with high sensitivity gives only a few false negatives.
- Specificity: This refers to the proportion of normal individuals who are correctly labeled as non-diseased by the screening test. A test with high specificity will only give a few false positives. It is desirable that a screening test should have high sensitivity and specificity.

Disease Outbreak
Introduction
An epidemic is the occurrence of a disease clearly in excess of normal expectations.
The number of cases that should be diagnosed before declaring an epidemic status depends on the number of cases routinely seen in that area. In an area where a disease has not been seen for many years, even the occurrence of a single case may be sufficient to call it an epidemic.
Epidemic diseases need not necessarily be communicable diseases; therefore, WHO also looks at smoking as an epidemic. A pandemic is an epidemic that breaks out across many continents, occurring across the world. Some pandemic diseases include HIV/AIDS, Multi-drug Resistant Tuberculosis, and smoking, as they have affected millions of people across the world. Plague was also pandemic in historical times.
Endemic diseases:
The constant, continuous, or usual presence of a disease in a defined geographic area or delimited territory is called an endemic disease. An endemic disease may become an epidemic if the number of cases usually seen suddenly increases in proportion. Malaria, tuberculosis, leprosy, filariasis, etc., are examples of endemic diseases.
Causes of Epidemics
- Unplanned and under-planned urbanization.
- Overcrowding.
- Poor sanitation.
- Deteriorating public health infrastructure, e.g., blocked sewage.
- Resistance to antibiotics.
- Increased exposure of humans to disease vectors and reservoirs.
Other important factors responsible for epidemics include:
- Illiteracy.
- Ignorance.
- Low socioeconomic status.
- High population growth, etc.
Management of an Epidemic in a Community
Individual Cases
- Managing individual cases demands a proper history and meticulous physical examination to clinically rule out all possible causes of fever in that area.
- Consideration of appropriate laboratory investigation will also assist in narrowing down the list of possible differential diagnoses and arriving at the right diagnosis.
- Once the diagnosis is confirmed, treatment should be promptly instituted accordingly (see the satellite module for health officers’ algorithm).
- While managing individual cases, one should make note of their addresses and see if there is any clustering of the cases.
Epidemic (Outbreaks)
Surveillance for Early Detection of Epidemics
Surveillance is an ongoing collection, analysis, and interpretation of data about people’s health.
Health officials use the information to plan, implement, and evaluate health programs and activities.
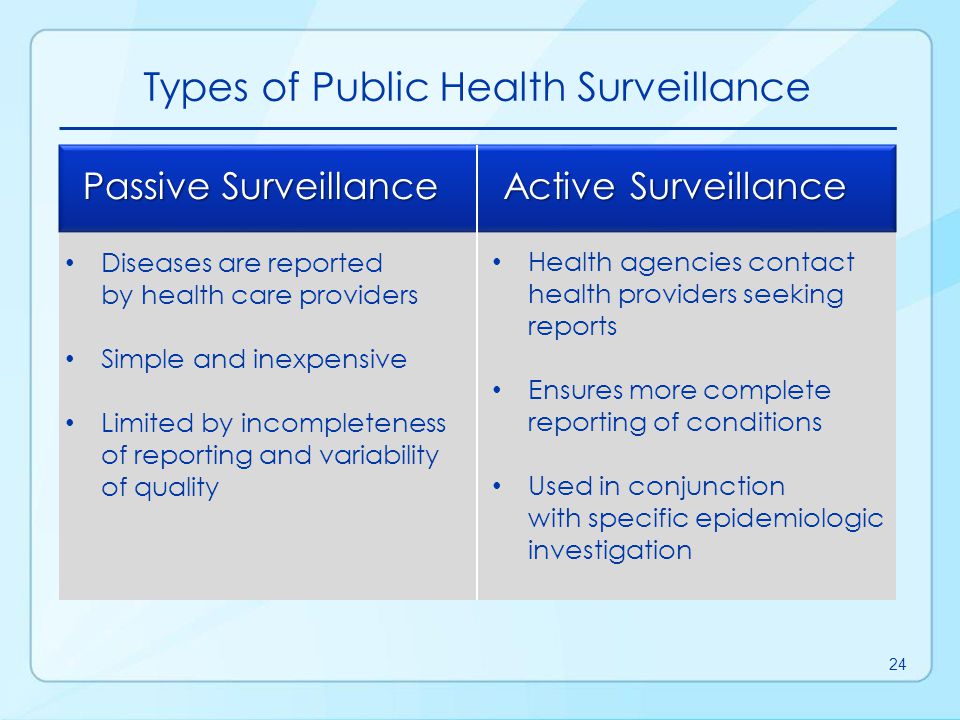
Types of Disease Surveillance
| No. | Passive | Active |
|---|---|---|
| 1. | Gathers disease data without stimulating healthcare workers to report disease | Gathers disease data that requires a stimulus to healthcare workers in the form of feedback or incentives. |
| 2. | Data requested is minimal | Requires more time and resources |
| 3. | Most common type | Data is more complete than passive surveillance |
| 4. | Data is often incomplete because there are few incentives for healthcare workers to report the required data | Example: trawling questionnaire for local infectious disease outbreak |
| 5. | Example: Vaccination uptake |
| No. | Sentinel | Syndromic |
|---|---|---|
| 1. | Selection of health workers/services from whom data is gathered, e.g., selection of General Practices | Monitors disease indicators in real-time or near real-time to detect clusters or outbreaks of disease earlier than would normally be possible |
| 2. | Requires more time and resources | Based on syndromes or clinical features, NOT diagnosis |
| 3. | Can produce more detailed and more complete data, particularly if healthcare workers have volunteered to participate | Inexpensive and rapid |
| 4. | Example: Influenza surveillance | Lacks specificity |
| 5. | Example: Early detection of communicable and non-communicable disease outbreaks during the 2012 Olympic Games in London |
Syndromic Surveillance is the process of collecting, analyzing, and interpreting health-related data to provide an early warning of human or veterinary public health threats that require public health action.
Uses of Disease Surveillance
- Monitor, determine, and describe the magnitude and natural history (trends) of disease incidence and prevalence.
- Identify key risk groups/populations, important risk factors, and etiological factors.
- Timely detection of epidemics, outbreaks, incidents, and other untoward events.
- Enable prediction of future trends (i.e., predictive modeling).
- Inform or evaluate health improvement programs.
Surveillance Loop
Data Sources
- Healthcare professionals.
- Hospital activity data.
- Laboratory data.
- Mortality data.
- Disease registers.
- Internet.
- Paper.
- Telephone.
- Electronic – emails.
- Online portals.
- Direct access via secure network.
Data Collation and Analysis
- Microsoft Excel & Access databases.
- De-duplication and de-notification.
- Time, place, person (Descriptive epidemiology).
- Statistical algorithms.
- Automated exceedance calculations.
- Statistical process control charts (C-charts).
- Statistical modeling.
Data Interpretation
Key considerations in interpreting trends:
- Natural and random variation.
- Data artifact – batched reporting, data entry errors, etc.
- Clinical & system changes – changes in case definition, increased awareness/ascertainment, improved diagnostics.
- Corroborate findings with other datasets and explore alternative explanations – highlight caveats (if any).
- Decide if these are real changes.
Key considerations in associations:
- Bias e.g. self-selection of the sample.
- Chance i.e. pure chance association.
- Confounding e.g. association explainable by a third factor.
Dissemination of Findings
- Ad-hoc and routine reports.
- Routine (weekly, monthly, or quarterly) epidemiological summaries.
- Web-based datasets/summaries.
- Special reports, guidelines, briefings, and queries.
- Research articles.
Evaluation
Steps in Evaluating a Surveillance System
- Usefulness.
- Simplicity.
- Flexibility.
- Data quality.
- Acceptability.
- Sensitivity.
- Predictive positive value.
- Representativeness.
- Timeliness.
- Stability.
Challenges Faced by Disease Surveillance
- Secular trends.
- Defining the population at risk.
- Magnitude.
- Changes from background incidence (outbreaks).
- Trajectory.
Disease Surveillance: Summary
- Information for action.
- Collect, collate, analyze, interpret, and disseminate.
- Understand epidemiology, identify problems, guide policy, monitor changes, etc.
- Cyclical in nature.
- Should be regularly evaluated.
- A key component of Public Health practice.
Purpose of Surveillance
- Detect outbreaks early.
- Plan vaccination campaigns.
- Estimate how many people become sick or die.
- Assess the extent of the outbreak.
- See if the outbreak is spreading and where.
- Decide whether the control measures are working.
It is essential to detect the epidemic early enough for preventive measures like vaccination campaigns to have an impact. Provide feedback of the surveillance data to peripheral levels to promote cooperation and interest in the surveillance system.
Investigation of an Epidemic
In the investigation of an epidemic, it is wise to follow a systematic approach, although public reaction, urgency, and the local situation may make this difficult.
The following list of steps need not always be undertaken in the order given, and some are done concurrently.
- Verification of the Diagnosis
- Take a detailed history as possible from the informants.
- Make tentative differential diagnoses.
- Make all arrangements, including laboratory equipment, for ascertaining the tentative differential diagnosis.
- Conduct clinical and laboratory studies to confirm the diagnosis. This should be done except in a few situations where the urgency demands immediate action based on clinical diagnosis alone.
- Verify the Existence of an Epidemic
- The existence of an epidemic could be ascertained by comparing the current incidence of the disease with its usual incidence in the community.
- Approximate estimates of previous incidence of the disease could be obtained from clinical and hospital data and by questioning the local people.
- Identification of Affected Persons and Their Characteristics
- Establish a case definition.
- Record details of each confirmed or suspected case, including age, sex, occupation, address, recent movements, symptoms, and other relevant details.
- Actively search for additional cases by interviewing all persons related in time and place to already known cases.
- For food poisoning, identify and interview all persons who attended the meal.
- Visit all health facilities, including dispensaries and village health workers, for unreported cases.
- General Management of the Epidemic
- Begin by treating individual cases.
- Prevent the spread and initiate control measures depending on the type of disease. Immediate measures may include chemoprophylaxis for immediate contacts, immunization, isolation of affected persons (quarantine), and measures to protect water sources, ensure food hygiene, and control vectors.
- Health education plays a significant role in preventing the spread of the epidemic.
- Continue surveillance of the population to detect further changes in incidence and ensure the effectiveness of selected control measures.
- Prevention
- Proper disposal of feces in a well-maintained sanitary latrine that is screened or vented to discourage fly access.
- Use of drinking water from protected sources, pot storage, exposure of drinking water to sunlight, or boiling before drinking.
- Washing of cooking and eating utensils using soap and hot water, drying them on a rack, and storing them in a cabinet out of the reach of children and animals such as dogs, cats, and chickens.
- Conduct hygiene education for the general public and especially for food handlers in mass catering institutions like prisons, restaurants, and hospitals.
- Periodically check cooks from such institutions to restrict carriers from working in food preparation areas.
Case Management
In Healthcare Setting
- Isolation of patients.
- Implementation of barrier nursing practices (wearing gloves, masks).
- Replenishment of fluid and electrolytes.
- Administration of appropriate prescribed therapy.
- Detection and prompt management of complications.
At the Community Level
- Visiting health posts and the community at large.
- Performing home, school, and prison visits.
- Following up at the homes of patients discharged from health centers.
- Providing health education and demonstrations.
- Offering immunizations and other preventive health programs.
Role of the Public Health Nurse in Epidemic Management
- Accurate diagnosis of cases.
- Prompt provision of treatment.
- Continuous follow-up.
- Accurate reporting to the concerned body.
- Active participation in the epidemic control system.
- Investigation of cases.
- Mobilization of the community for prevention activities.
- Analysis of data from the peripheral level for epidemiological links, trends, and achievement of control targets.
- Providing feedback to the peripheral level.
- Organizing essential logistics.
Sample of Management of a Cholera Epidemic
Management of Cholera Epidemic in a Community
Epidemic management activities include taking appropriate control measures, such as treating those who are ill to reduce the reservoir of infection, and providing health education to limit the transmission of the disease to others.
Case Management:
- Patients are admitted to a temporary facility (e.g., school, tents, cholera camp) in the community in the case of cholera.
- Appropriate laboratory investigations are considered to narrow down possible differential diagnoses and confirm the diagnosis.
- Patients are managed with water and electrolyte replacement in case of dehydration and electrolyte depletion.
- The cause is treated with appropriate antimicrobials (e.g., Cotrimoxazole, erythromycin, ciprofloxacin, and doxycycline).
Disease Prevention and Control Measures:
- Proper disinfection and disposal of body fluids such as vomitus and stool.
- Water purification, including sterilization by boiling or chlorination in areas where cholera may be present.
- Ensuring food safety, avoiding uncooked food, covering leftovers to prevent fly contamination, and temporarily stopping food vendors until the epidemic is controlled.
- Chemoprophylaxis for immediate contacts (e.g., Cotrimoxazole) as prophylaxis in the case of cholera.
- Inspection of markets and other public institutions.
Health Education to the Community/Public
- Proper washing of cooking and eating utensils using soap and hot water, followed by drying and storage in a cabinet out of the reach of children and animals.
- Hygiene education, especially for food handlers in mass catering institutions like prisons, restaurants, and hospitals.
- Improving sanitation.
- Promoting proper use of pit latrines.
Disease Surveillance:
This is continuous monitoring of all aspects of diseases, including field investigations such as culturing. It describes the magnitude and distribution of diseases by place, time, and personal characteristics such as age and sex.
Public health surveillance of communicable diseases involves continuous data collection, data analysis, interpretation of the data, and dissemination of the information to concerned bodies such as the District Health Office and nearby Health Centers. Disease Surveillance helps evaluate progress toward control measures.
Summary on Prevention of Infectious Diseases:
This depends on:
- The reservoir or source of infection.
- Routes of transmission of infection.
- Susceptible hosts (people at risk).
The primary aim behind controlling and preventing a disease is to:
- Eliminate the source of infection.
- Interrupt the routes of transmission.
- Strengthen the defense mechanisms of people at risk.
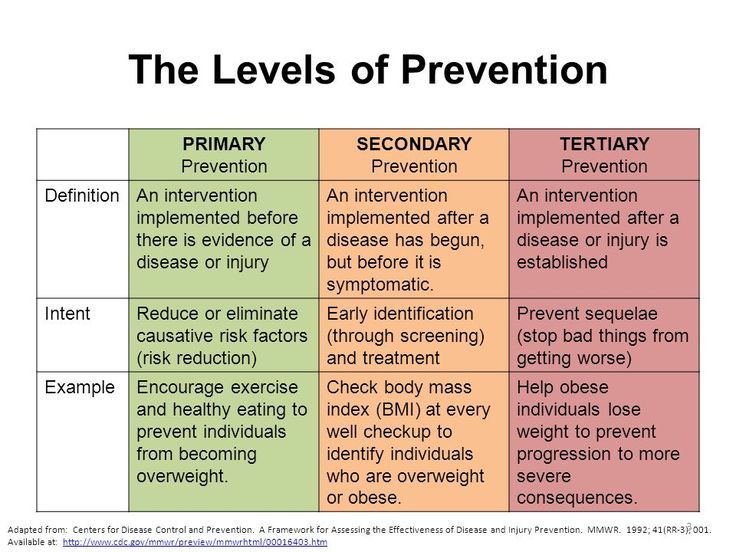
Levels of Disease Prevention:
Primary (1°) Prevention:
- Prevention that occurs before disease or dysfunction and is applied to individuals considered physically and emotionally healthy.
- It aims at intervention before pathological diseases have begun during the stage of susceptibility.
- It includes activities directed at reducing the probability of specific illnesses or impairments.
- 1° prevention includes both general health promotion and specific protection.
General health promotion includes:
- Health education.
- Good standards of nutrition adjusted to developmental stages of life.
- Attention to personality development.
- Provision of adequate housing, recreation, and agreeable working conditions.
- Genetic screening.
- Marriage and sex education.
- Periodic selective examination.
Specific Protection refers to measures aimed at protecting individuals against specific agents, e.g.:
- Immunization.
- Vaccination.
- Attention to personal hygiene for self-care.
- Use of environmental sanitation, e.g., chlorination of wells.
- Protection from accidents, e.g., wearing helmets.
- Use of specific nutrients.
- Protection or avoidance of allergens.
- Protection from carcinogens.
Any specific disease or health problem is the result of interactions between specific or associated risk factors that can be classified as Agent, Host, and Environmental factors. This interaction can be understood by visualizing the concepts of positive health and disease.
Secondary Prevention (2°):
Activities are directed at:
- Early Diagnosis and Treatment:
- Case finding measures, both individual and mass.
- Screening surveys.
- Selective exams.
- Cure and prevention of the disease process to prevent the spread of communicable diseases, prevent conditions, and shorten the period of disability.
- Limitation of Disability:
- Adequate treatment to arrest the disease process and prevent conditions.
- Provision of facilities to limit disability and prevent death.
Tertiary (3°) Prevention:
- Occurs when the defect or disability is permanent.
- It includes rehabilitation for those individuals who have already experienced residual damage.
- Tertiary prevention activities focus on the middle to latter phases of clinical disease, where irreversible pathological damage produces disability (e.g., post-stroke rehabilitation).
Activities include:
- Provision of hospital and community facilities for training and education to maximize the use of remaining capacities.
- Education of the public and industries to use rehabilitated individuals to the fullest extent.
- Selective placement.
- Work therapy and hospital-based interventions.
In 3° prevention, activities mainly aim at rehabilitation rather than diagnosis and treatment. The goal at this level is to help patients achieve the highest level of functioning possible despite limitations caused by illness or impaired functions.
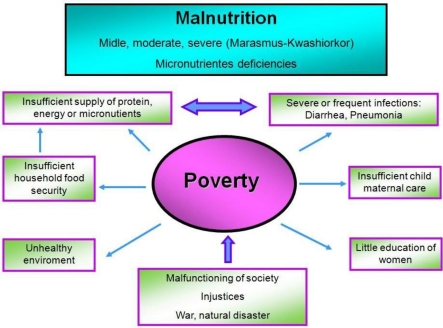
Malnutrition in the Community
Definition of Malnutrition: Malnutrition is a disparity between the amount of food and other nutrients that the body needs and the amount that is received. This imbalance can result in undernutrition or overnutrition.
Causes of Malnutrition in the Community:
- Age: Basal metabolic rate (BMR) and physical energy expenditure vary with age, e.g., kwashiorkor is common in children.
- Sex: Pregnant mothers usually suffer from nutritional anemia.
- Habits and Traditional Beliefs: For example, the habit of consuming fast food rather than traditional foods.
- Socioeconomic Factors: People with lower incomes are more likely to suffer from undernutrition, while the affluent may suffer from overnutrition.
- Physical Factors: Climate, geographic location, and home environment can affect nutrition.
- Population Density: Overpopulated areas compete for resources, including food, and are more likely to suffer from malnutrition.
- Prevalence of Communicable and Parasitic Infestations: For example, measles in children and intestinal worms.
- Unfavorable Climate Conditions: Such as droughts.
- Lifestyles: Consuming excessive alcohol (alcoholism) and smoking can cause malnutrition.
- Political Instability.
- Natural Disasters, etc.
Roles of a Nurse/Midwife in the Prevention of Community Malnutrition:
These roles can be divided into three levels:
- Health Education: Providing community education about preventive, curative, and rehabilitative measures for malnutrition.
- Immunization: Encouraging community members to immunize their children against communicable diseases.
- Promoting Income-Generating Activities: To help individuals earn a living.
- Family Planning: Encouraging people to have smaller families they can care for.
- Promotion of Girl Child Education.
- Advocating for Adequate Food Storage.
- Proper Weaning Practices.
- Encouraging a Well-Balanced Diet.
- Early Detection of Congenital Abnormalities.
- Maintaining Hygiene to Prevent Illness.
- Conducting Population Screening to identify individuals with malnutrition and providing immediate referrals to prevent illness from becoming severe.
- Case Management: Starting patients on nutritional intervention programs.
- Maintaining Personal and Communal Sanitation.
- Encouraging Drug Compliance.
- Promoting Girl Child Education.
- Encouraging Follow-up to Assess the Effectiveness of Interventions.
- Educating the Public on Various Economic Activities to Earn a Living.
- Improving Medical Facilities, Including Maternal and Child Health Services in the Community.
Role of the Family in Health Promotion:
- Child Spacing.
- Engaging in Income-Generating Activities.
- Improving Nutrition.
- Providing Good Housing.
- Ensuring Immunization.
- Practicing Enhanced Personal Hygiene.
- Creating a Safe Environment.
Role of the Community in Health Promotion:
- Proper Excreta Disposal.
- Appropriate Refuse Disposal.
- Contact Tracing.
- Health Education.
- Screening.
- Rehabilitation.
- Enhancing School Health.
- Encouraging Community Participation and Involvement.
Role of Government in Health Promotion:
- Conducting Health Education.
- Implementing Health Awareness and Enlightenment Programs.
- Facilitating Inter-Sectoral Collaboration.
- Establishing National Policies.
- Enforcing Rules and Regulations to Protect Children Against Child Abuse.
- Monitoring and Evaluating Programs.
Role of Community Health in Disease Prevention and Health Promotion:
- Maintaining Good Sanitation and Access to Clean Water.
- Providing Health Education on Healthcare and Nutrition.
- Controlling Both Communicable and Non-Communicable Diseases.
- Organizing Adequate Medical and Nursing Services.
- Improving Living Standards with the Help of Other Sectors and Active Involvement of Beneficiaries and the Community.
Revision Questions:
- Explain the three components of the Epidemiological Triad and give an example of each for a common cold.
- What is the difference between Pathogenicity and Virulence?
- List the six links in the Chain of Infection in order. For each link, provide one example of a nursing intervention to break it.
- Describe the goal of each of the three levels of prevention.
- Giving a patient a vaccination is an example of which level of prevention? Why?
HEALTH AND DISEASE Read More »








 : End poverty in all its forms everywhere.
: End poverty in all its forms everywhere. : End hunger, achieve food security and improved nutrition, and promote sustainable agriculture.
: End hunger, achieve food security and improved nutrition, and promote sustainable agriculture. : Ensure healthy lives and promote well-being for all at all ages.
: Ensure healthy lives and promote well-being for all at all ages. : Ensure inclusive and equitable quality education and promote lifelong learning opportunities for all.
: Ensure inclusive and equitable quality education and promote lifelong learning opportunities for all. : Achieve gender equality and empower all women and girls.
: Achieve gender equality and empower all women and girls. : Ensure availability and sustainable management of water and sanitation for all.
: Ensure availability and sustainable management of water and sanitation for all. : Ensure access to affordable, reliable, sustainable, and modern energy for all.
: Ensure access to affordable, reliable, sustainable, and modern energy for all. : Promote sustained, inclusive, and sustainable economic growth, full and productive employment, and decent work for all.
: Promote sustained, inclusive, and sustainable economic growth, full and productive employment, and decent work for all. : Build resilient infrastructure, promote inclusive and sustainable industrialization, and foster innovation.
: Build resilient infrastructure, promote inclusive and sustainable industrialization, and foster innovation. : Make cities and human settlements inclusive, safe, resilient, and sustainable.
: Make cities and human settlements inclusive, safe, resilient, and sustainable. : Ensure sustainable consumption and production patterns.
: Ensure sustainable consumption and production patterns. : Take urgent action to combat climate change and its impacts.
: Take urgent action to combat climate change and its impacts. : Conserve and sustainably use the oceans, seas, and marine resources for sustainable development.
: Conserve and sustainably use the oceans, seas, and marine resources for sustainable development. : Protect, restore, and promote sustainable use of terrestrial ecosystems, sustainably manage forests, combat desertification, halt and reverse land degradation, and halt biodiversity loss.
: Protect, restore, and promote sustainable use of terrestrial ecosystems, sustainably manage forests, combat desertification, halt and reverse land degradation, and halt biodiversity loss. : Promote peaceful and inclusive societies for sustainable development, provide access to justice for all, and build effective, accountable, and inclusive institutions at all levels.
: Promote peaceful and inclusive societies for sustainable development, provide access to justice for all, and build effective, accountable, and inclusive institutions at all levels. : Strengthen the means of implementation and revitalize the global partnership for sustainable development.
: Strengthen the means of implementation and revitalize the global partnership for sustainable development. have
have