Opioid Abuse & Opioid Toxicity
Toxicology is the scientific study of the adverse effects of chemicals or poisons on living systems. Poisoning refers to the bodily entry of a toxic substance in amounts that cause dysfunction of body systems.
- Poisoning: Voluntary or accidental ingestion, inhalation, or absorption of a toxic substance.
- Antidote: A chemical substance that specifically stops, reverses, or counteracts the effects of a poison.
- Microorganisms: e.g., bacterial toxins in food poisoning.
- Inorganic sources: e.g., lead, mercury, copper metal poisoning.
- Organic sources: e.g., agricultural chemicals (organophosphates), paraffin, petrol.
- Drug abuse / Overdose: e.g., alcohol, opioids, or medicines in excess amounts (paracetamol, aspirin).
Optimal management depends on the specific poison taken, presenting and suspected illness, and the time that has elapsed between exposure and presentation. Rule of thumb: In a hospital setting, admit all patients with a history or signs of poisoning even if they currently appear well.
- Supportive Care (ABCs & Vitals):
- Airway and Breathing: Position the patient in a semi-prone (lateral recovery) position to minimize the risk of aspiration of vomitus. Maintain a patent airway and if necessary, assist in ventilation. Administer oxygen.
- Blood Pressure (Circulation): If hypotensive, raise the foot of the bed and start IV Normal Saline (N/S). If hypertensive, manage appropriately.
- Temperature Control: If hypothermic, cover with heavy blankets. If hyperthermic, perform tepid sponging and give antipyretics.
- Convulsion Management: Give Diazepam 10mg rectally or 5-10mg as slow IV in adults (Max dose is 30mg). In children, give 0.5mg/kg rectally or 0.2mg/kg as IV.
- Decontamination (Removal and Elimination):
Decontamination must be implemented after the stabilization of vitals.
- Gastric Emptying: Do not induce vomiting. Balance the dangers of gastric emptying against the likely toxicity of the swallowed medicine. Insert an NG tube and perform gastric lavage. It is highly useful if done within 2 hours of ingestion. Contraindicated in: comatose patients (without a protected airway), and in corrosive or petroleum product ingestion.
- Prevention of Absorption: Administer Activated Charcoal to bind the poison in the stomach and reduce absorption. Give 50g (or 25g-50g) repeated every 4 hours if necessary. Grind the tablets into fine powder then mix with 100mls of water. In children, give 0.5-1g/kg. This is effective within 2 hours of ingestion. Contraindicated in: intestinal obstruction, corrosive/petroleum products, toxins poorly absorbed by charcoal (e.g., metals, alcohol), and depressed mental status (late presentation without an airway).
- Specific Antidote Therapy (Discussed in sections below).
- Counseling: Counsel patients and families on poisoning prevention and mental health support.
Opiophobia in Africa (The New York Times / Katzung Basic Pharmacology)
"Despite that risk, under no circumstances should adequate pain relief ever be withheld simply because an opioid exhibits potential for abuse or because legislative controls complicate the process of prescribing narcotics."
- Opioids: All natural, synthetic, and semisynthetic agents with morphine-like actions.
- Opiates: Naturally occurring opioids derived from the poppy plant.
- Opium: (Greek for juice) in reference to poppy juice from the opium poppy (Papaver sp.).
- Morphine (the prototype) was isolated by Sertürner in 1803 and named after Morpheus (the Greek god of dreams). It produces profound analgesia, sedation, and euphoria.
- Endorphins: Endogenous opioid peptides (endomorphins, dynorphins, enkephalins) produced naturally in the body.
- Narcotic: Broadly refers to any agent that induces sleep (nonspecific).
- The global prevalence of opiate use (heroin, morphine, and opium) is roughly 0.4% of the population aged 15-64 years.
- The global number of opiate users increased from 17.7 million in 2015 to 19.4 million in 2016.
- 70,000 to 100,000 people die from opioid overdose each year globally.
- In Africa, massive seizures of counterfeit tramadol occur regularly (e.g., 40 million pills seized in Cotonou, Benin; heavy illicit trade in Nigeria, Ghana, Togo, Niger, Sierra Leone, Cameroon).
- In the US (CDC 2010), enough opioid analgesics were sold to medicate every American adult with a typical dose of 5 mg of hydrocodone every 4 hours for 1 month.
- Morphine: M, Miss Emma, Monkey, China Girl, Murder-8.
- Heroine: The Dragon, Snowball, Tar, White, White Nurse.
- Tramadol: Chill pill, Tramal Lite, Trammies. (The Super Tramadol-X 200 brand is known in Cameroon as 'tomatoes').
| Classification by Source | Classification by Potency |
|---|---|
|
|
- Absorption: Well absorbed enterally or parenterally. Routes include transdermal patches, rectal suppositories, buccal transmucosal (lozenges), and oral (subject to high 1st pass effect). Serum therapeutic doses are reached 1 to 2 hrs after oral ingestion. Heroin peaks extremely fast: IV (1 min), inhalation (3-5 min), SC (10 min).
- Distribution: High volume of distribution; easily crosses the Blood-Brain Barrier (BBB). Predilection for highly perfused tissues (brain, lungs, liver, kidneys, spleen). Adipose tissues are poorly perfused but serve as dangerous reservoirs for lipophilic opioids (like fentanyl).
- Metabolism: All opioids undergo hepatic metabolism via Cytochrome P450 enzymes.
- Morphine undergoes glucuronidation into morphine-3-glucuronide (M3G - neuroexcitatory properties) and morphine-6-glucuronide (M6G - 4 to 6 times more potent analgesia).
- Heroin is rapidly hydrolyzed to morphine.
- Pethidine and Fentanyl undergo hepatic oxidation.
- CYP2D6 Polymorphism: Codeine and Tramadol are metabolized by CYP2D6 into active forms (Morphine & O-desmethyltramadol respectively). Oxycodone is also metabolized by CYP2D6 (into less active metabolites). Fentanyl is metabolized by CYP3A5 into inert metabolites. Genetic polymorphism causes massive interindividual variability and dangerous drug interactions.
- Excretion: Predominantly renal elimination. Renal impairment heavily increases the risk of toxicity. Dialysis cannot clear opioids effectively.
- Receptors: 3 main types: mu (μ), kappa (κ), and delta (δ). Present in the CNS (dorsal horn of spinal cord, areas of nociception, respiratory center, and reward/euphoria centers) and Systemically (sensory nerves, GIT, CVS endothelium, immune cells).
- Mechanism: They close voltage-gated Ca2+ channels on the presynaptic nerve to drastically reduce neurotransmitter release (Glutamate, Acetylcholine, Norepinephrine, Serotonin, and Substance P). They also hyperpolarize postsynaptic neurons by opening K+ channels. This activates descending inhibitory pathways that block pain transmission.
- Analgesia (Myocardial Infarction, renal colic, cancer patients, obstetrics).
- Antidiarrheal effects (e.g., Loperamide, Lomotil).
- Antitussives (e.g., Codeine in cough mixtures).
- Anti-Shivering (e.g., Pethidine).
- Anaesthesia (Pre-medicant due to sedative, anxiolytic, and analgesic effects; as an adjunct intra-operatively; or for regional epidural/subarachnoid block).
- People at risk: Opioid-dependent individuals, especially those with reduced tolerance (e.g., recently released from incarceration or rehab); people on prescribed opioids; users combining opioids with other sedatives (alcohol, benzos); people with lung, liver, or renal impairment; household members (accidental ingestion by children).
- Source of history: Witnesses, friends, families, health care workers, police, emergency service workers, outreach/peer workers. Note the time of ingestion, quantity, and co-ingestants.
- Clues: Pill bottles, drug paraphernalia (spoons, lighters, syringes, tourniquets), or eyewitness accounts.
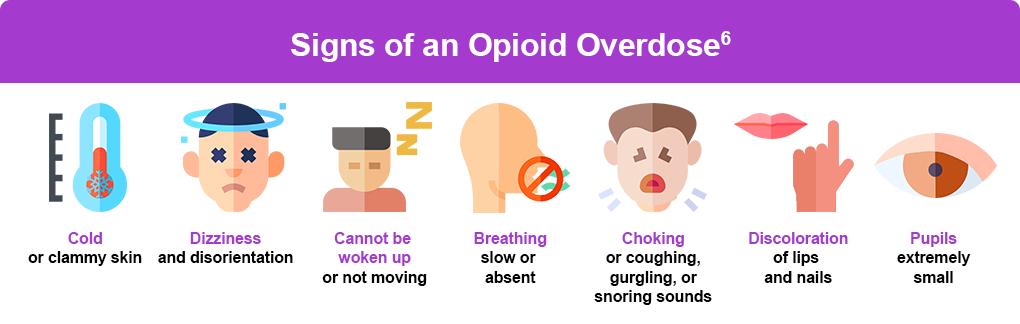
A voluntary or accidental overdose leads to life-threatening physiological changes. The hallmark is the Opioid Toxidrome.
THE OPIOID TOXIDROME (Classic Triad)
- 1. CNS Depression: Decreased mental status, extreme drowsiness, progressing to coma.
- 2. Respiratory Depression: Bradypnea (4 to 6 cycles/min), hypopnea (reduced tidal volumes), hypoxia. This is the primary cause of death.
- 3. Pupillary Miosis: Pinpoint pupils. (Note: Mydriasis/dilation can sometimes occur with specific opioids like pethidine, propoxyphene, or due to extreme CNS hypoxia).
Other Systemic Features:
- Physical/Dermatological: Needle tracks are often evident (Skin-popping/SC injections, and Mainlining/IV). Powdery substances around the nose. Pruritus (itching), flushed skin, and urticaria due to histamine release.
- Respiratory: Acute Lung Injury (ALI), presenting with pink frothy sputum, severe dyspnea, bronchospasm, and muscular rigidity (wooden chest).
- Cardiovascular: Hypotension (Orthostatic), bradycardia, and arrhythmias. Exception: Pethidine, cocaine co-ingestion, or severe cerebral hypoxia can cause paradoxical tachycardia and hypertension.
- Gastrointestinal: Nausea, vomiting, severe constipation, and in severe cases, paralytic ileus (absent bowel sounds).
- Renal: Urinary retention due to urethral sphincter spasm and decreased detrusor tone. Heroin nephropathy.
- Special CNS Features:
- Seizures: Specifically seen with Pethidine, Propoxyphene, and Tramadol overdoses.
- Parkinsonian symptoms: Bradykinesia, resting tremors, rigidity, and postural instability. (Often seen with Pethidine produced in street labs containing MPTP metabolites, causing focal lesions in the Substantia nigra).
- Heroin Associated Spongiform Leukoencephalopathy (HASL): Causes psychomotor retardation, dysarthria, ataxia, tremor.
- Serotonin Syndrome: Caused by ingesting opioids with serotonergic properties (Pethidine, Tramadol, Fentanyl, Oxycodone, Methadone) alongside MAOIs, SSRIs, or TCAs. Presents with altered mental status, autonomic instability (hyperthermia, diaphoresis), and neuromuscular hyperactivity (hyperreflexia, clonus, rigidity).
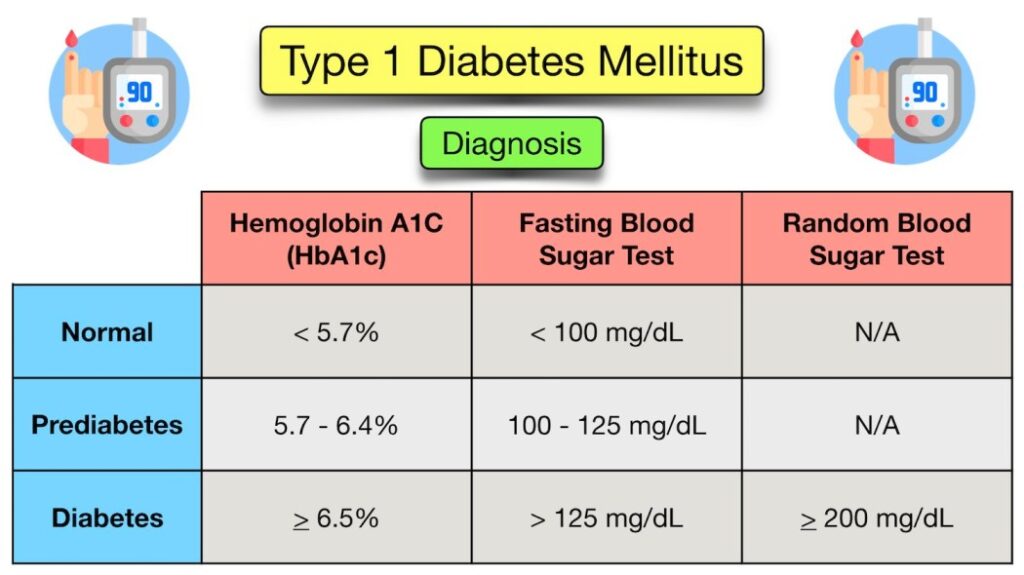
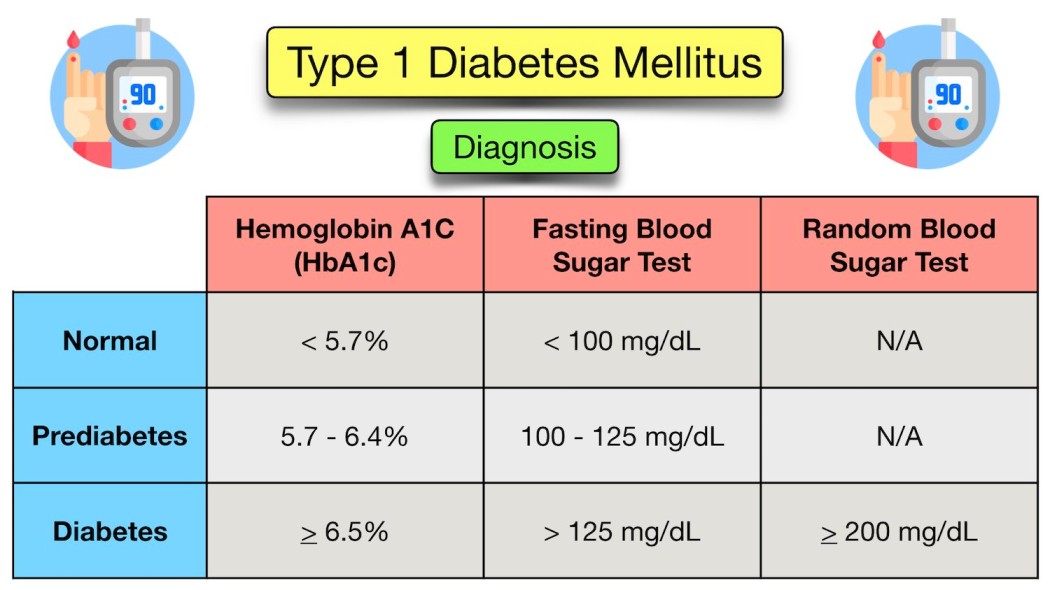
- Biochemistries: RBS (Random Blood Sugar to rule out hypoglycemia), BUE (Urea), and Creatinine (Renal function).
- Continuous SPO2 monitoring and Arterial Blood Gases (ABGs) to check for hypoxia/hypercapnia.
- 12-lead ECG: Crucial for detecting QRS widening, QT prolongation, or Torsades de pointes (especially dangerous with propoxyphene or methadone).
- Chest X-ray (CXR): To detect hypoxemia complications, pulmonary edema, and coarse crackles (rales).
- Abdominal X-ray: Mandatory to rule out "Body packers/mules" (drug smuggling via swallowed packets).
- Urine Toxicology Screen: Remains positive for days after last use.
- Serum acetaminophen and salicylate levels (frequently co-ingested).
- Benzodiazepine and Barbiturate toxicity
- Hypoglycemia (always check blood sugar!)
- Gamma-hydroxybutyrate (GHB) toxicity ("liquid ecstasy")
- Clonidine toxicity
- Alcohol toxicity
- Cannabinoid poisoning
- Meningitis
The primary aim is restoring respiration, not necessarily restoring full consciousness.
- Airway & Breathing: Provide Supplemental Oxygen via Bag-Valve-Mask (BVM). If the airway is unprotected or respiratory failure is profound, proceed to Endotracheal intubation. Continuous cardio-respiratory monitoring.
- Circulation & Fluids: Correction of dehydration and/or electrolyte imbalance using IV Ringer's Lactate (RL) or Normal Saline (NS).
- Metabolic: Immediate correction of Hypoglycemia with IV Dextrose.
- Seizure Control: Abortion of any active seizures using IV Diazepam.
- GIT Decontamination: If the patient is a body packer, has taken a multi-drug ingestion, or an opioid combination product, use whole-bowel irrigation and activated charcoal (only if the airway is secure).
Indicated in cases of significant CNS and respiratory depression.
- Naloxone (Narcan): A pure competitive antagonist.
- Onset: 1-2 minutes. Maximal effect: 5-10 minutes. Duration of action: 1 to 2 hours (often shorter than the opioid, requiring repeat dosing).
- Adult Dose: 0.4 to 2 mg IV, IM, or SC. Repeat every 2-3 minutes if not improving, up to a maximum of 10 mg. (Also available as an Intranasal spray at 0.4mg/spray).
- Pediatric Dose: 0.1 mg/kg IV in children < 5 yrs; OR 0.1-2mg/dose in children > 5 yrs.
- Chronic Users / Dependent Patients: Give tiny aliquots of 0.04 to 0.2 mg IV and slowly titrate up. This avoids precipitating an acute, explosive withdrawal syndrome.
- Contraindication: Naloxone must be used with extreme caution or is relatively contraindicated in opioid-induced respiratory depression in chronic opioid use, such as in palliative care for terminal cancer patients, as it will cause a massive, intractable pain crisis.
- Diagnostic check: Reconsider the diagnosis if the patient completely fails to respond after 10 mg of Naloxone.
- Nalmefene: A longer-acting alternative antagonist.
- Asymptomatic adults: Must be observed for at least 4 hours post-ingestion or post-Naloxone.
- Asymptomatic children: Must be observed for at least 24 hours.
- Adults with respiratory depression: Admitted to ICU/HDU for 12-24 hours.
- Length of detention: Highly dependent on the half-life of the specific opioid. (e.g., Diphenoxylate-atropine / Lomotil has a very long T1/2 and requires prolonged monitoring).
- Body Packers: Discharged only after definitively passing out all packets (confirmed by clear imaging).
- Psychiatric Follow-up: Mandatory psychiatric evaluation or drug abuse counseling prior to discharge. Discharge only to a stable social setting.
- Acute Lung Injury (ALI) / Non-cardiogenic pulmonary edema
- Cellulitis and Osteomyelitis (from dirty needles)
- Horner Syndrome
- Infective Endocarditis
- Heroin Associated Spongiform Leukoencephalopathy (HASL)
- Heroin Nephropathy
- Parkinsonian disorder
- Severe Withdrawal syndrome
Benzodiazepines (e.g., Diazepam, Midazolam) are used for anxiety and as sedatives. Overdose can be intentional or accidental.
- Clinical Presentations: Confusion, severe drowsiness, hypotension, unresponsiveness/coma, respiratory depression (especially when mixed with alcohol or opioids), nystagmus, slurred speech, and body weakness/hypotonia.
- Management:
- Supportive care (Airway, Breathing).
- Administer activated charcoal if presentation is recent (within 1-2 hours) and airway is protected.
- Specific Antidote: Flumazenil. Give 0.2 mg IV over 30 seconds. Repeat if necessary. (Use with caution in chronic users as it can precipitate life-threatening seizures).
- Management: Obtain a baseline prothrombin time and international normalized ratio (PT/INR) and arrange for repeat measurements.
- Specific Antidote: If the INR is dangerously elevated or there is active bleeding, reverse the effects with Vitamin K1 (Phytomenadione). Give 10mg orally or by slow IV infusion.
- For urgent, immediate reversal of life-threatening bleeding, administer Fresh Frozen Plasma (FFP) or Prothrombin Complex Concentrate (PCC) (also known as factor IX complex).
Accidental or intentional consumption. The toxic dose is >150mg/kg or >7.5g in adults.
- Clinical Features (Stages):
- First 24 hours: The individual may be asymptomatic or present with non-specific nausea, vomiting, malaise, and abdominal pain.
- 24-72 hours: Progressive signs of severe hepatotoxicity appear (right upper quadrant pain, enlarged tender liver, and drastically raised Liver Function Tests/LFTs).
- After 72 hours: Either recovery after 5-7 days or progression to fulminant hepatic failure, coagulopathy, encephalopathy, and death.
- Management:
- If ingestion occurred less than 2 hours ago, perform gastric lavage and give repeated doses of activated charcoal (25-50g every 4 hours).
- Specific Antidote: N-acetylcysteine (NAC). Best if started within 8 hours of ingestion. It reduces toxicity by providing cysteine for glutathione synthesis (a powerful antioxidant). Glutathione reacts with the toxic metabolite (NAPQI) so it can be safely excreted without destroying liver cells.
- NAC IV Protocol: 150mg/kg (max 15g) in 200mls D5W over 60 minutes; followed by 50mg/kg (max 5g) in 500ml D5W over 4 hours; followed by 100mg/kg (max 10g) in 1000ml D5W over 16 hours.
Overdose occurs with consumption of > 10g in adults and > 3g in children.
- Clinical Features: Mild to moderate toxicity features hyperventilation (causing primary respiratory alkalosis), nausea, vomiting, vasodilation, and tinnitus (ringing in ears). Severe toxicity leads to hyperpyrexia, convulsions, altered mental status, and a profound metabolic acidosis.
- Management: Activated charcoal. Correct fluid and electrolyte imbalances. Alkalinization of urine using IV Sodium Bicarbonate enhances the excretion of salicylates. Hemodialysis is required for severe, life-threatening toxicity.
Methanol is an industrial solvent and an ingredient in methylated spirits. It is heavily associated with home-distilled crude alcohol. Ingestion of >1g/kg is lethal. It is transformed by alcohol dehydrogenase into toxic formic acid, causing severe anion-gap metabolic acidosis.
- Clinical Features: Initially presents with headache, dizziness, nausea, vomiting, and visual disturbances ("snowstorm" vision). Later causes CNS depression, respiratory failure, coma, and irreversible retinal optical nerve damage (blindness).
- Management: Gastric lavage if within 1 hour. Charcoal is not effective. Give IV fluids to manage shock. Hemodialysis is highly effective.
- Specific Antidote: Fomepizole or Ethanol (which competitively inhibits alcohol dehydrogenase, stopping the conversion of methanol into toxic acid).
- Presents with severe hemorrhagic gastroenteritis, shock, and hepatotoxicity.
- Specific Antidote: Deferoxamine. Give a continuous infusion of 5mg/kg/hr to 15mg/kg/hr in N/S or D5W until metabolic acidosis clears or symptoms improve. Avoid in cases of severe renal failure.
Includes paraffin, petrol, paint thinners, and organic solvents.
- Clinical Features: Smell of hydrocarbons on breath, burning sensation in the mouth/throat, pallor, severe dyspnea, tachypnea, coughing, lethargy, vomiting, and bloody stool.
- Management: Remove contaminated clothes and wash skin with soap and water. Administer oxygen if hypoxic. Treatment is strictly supportive.
- CRITICAL WARNING: Strictly avoid gastric lavage, use of enemas, or induction of vomiting. Do not give charcoal. These hydrocarbons have low viscosity and high volatility; attempting to empty the stomach leads to a massive risk of aspiration, resulting in fatal chemical pneumonitis.
| Toxin / Poison | Specific Antidote |
|---|---|
| Opioids / Narcotics (Morphine, Heroin, Tramadol) | Naloxone (Narcan) or Nalmefene |
| Benzodiazepines (Diazepam, Midazolam) | Flumazenil |
| Paracetamol (Acetaminophen) | N-acetylcysteine (NAC) |
| Warfarin | Vitamin K1 (Phytomenadione) / FFP |
| Methanol / Ethylene Glycol | Fomepizole or Ethanol |
| Iron | Deferoxamine |
| Organophosphates (Insecticides) | Atropine and Pralidoxime (2-PAM) |
| Carbon Monoxide | 100% Oxygen (Hyperbaric Oxygen if severe) |
| No. | Nursing Diagnosis | Interventions & Rationale |
|---|---|---|
| 1 | Ineffective Breathing Pattern related to CNS and respiratory center depression secondary to drug overdose (e.g., opioids, benzodiazepines). |
|
| 2 | Risk for Aspiration related to depressed level of consciousness, absent gag reflex, or forceful emesis post-poisoning. |
|
| 3 | Decreased Cardiac Output related to myocardial depression, hypovolemia, or toxin-induced arrhythmias (e.g., methadone prolonging QT). |
|
| 4 | Deficient Knowledge / Ineffective Coping related to psychological dependence, lack of problem-solving skills, and risk of relapse. |
|
- Rosen Emergency Medicine 8th Edition, Opioids.
- Katzung Basic & Clinical Pharmacology 12th Edition.
- World Health Organization (WHO) Community Management of Opioid Overdose (2014) & Critical Review Report: Tramadol (2018).
- Nelson Textbook of Paediatrics 20th Edition (2015).
- Medscape Clinical Guidelines: Opioid Toxicity and General Poisoning Management.
Quick Quiz
Narcotic Abuse Quiz
Pharmacology - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
Narcotic Abuse Quiz
Pharmacology
Preparing questions...
Choose your answer and keep your streak alive.
Great effort.
Here is your quick performance summary.
Opioid Abuse & Opioid Toxicity Read More »